
Effect of Propolis Paste and Mouthwash Formulation on Healing after Teeth Extraction in Periodontal Disease

 and
and
Abstract
:1. Introduction
2. Results
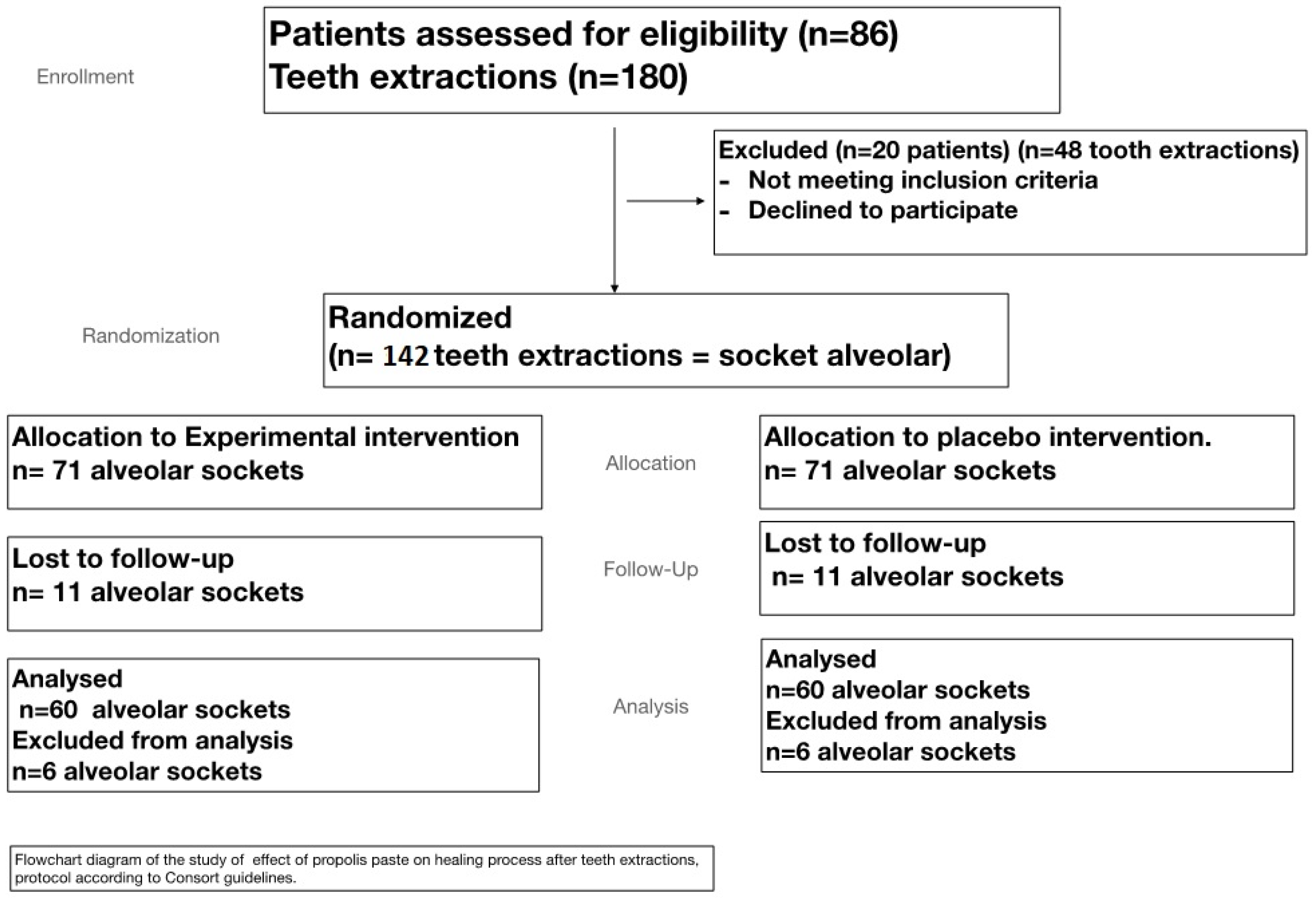
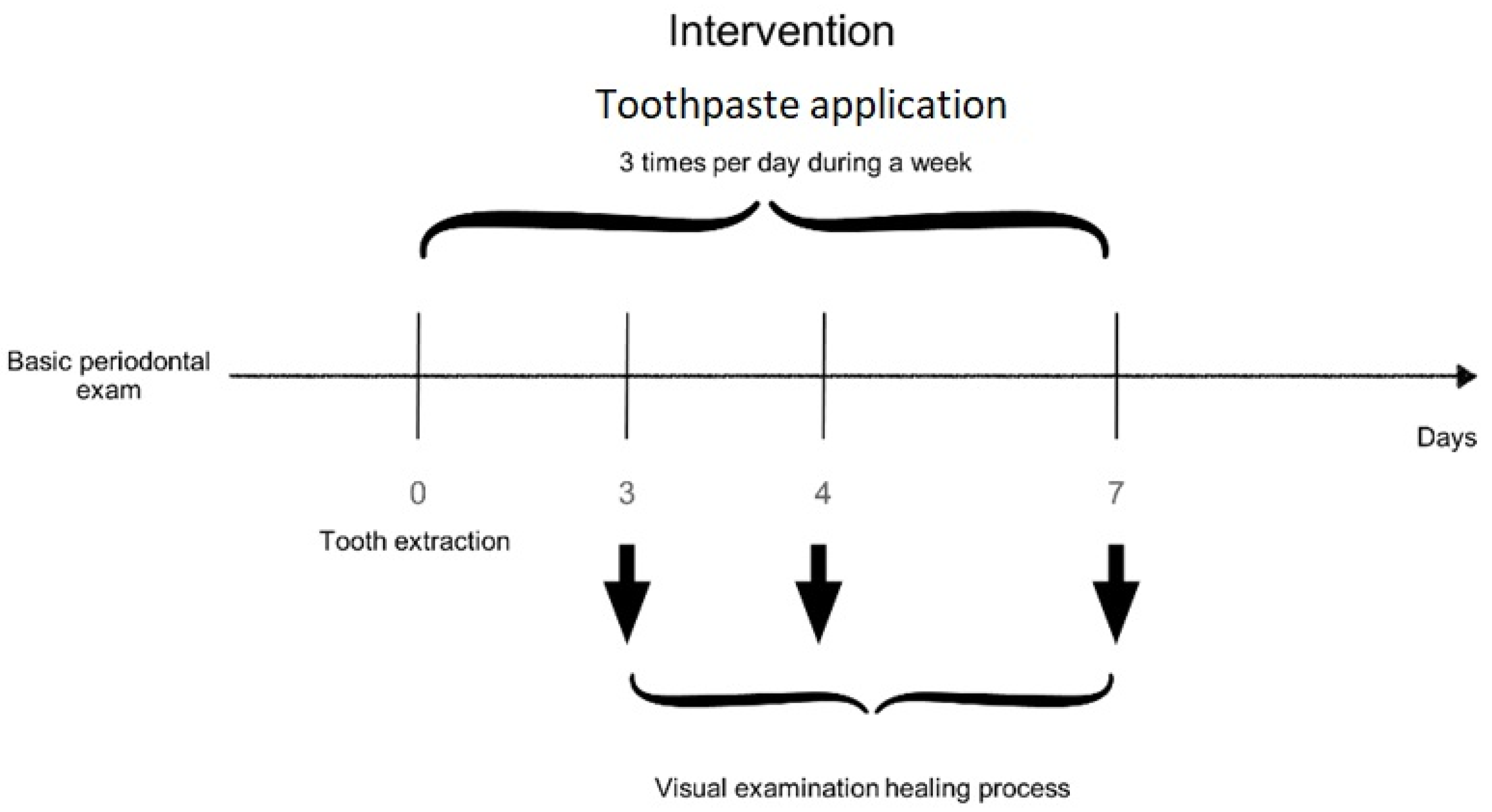
2.1. Toothpaste Assay
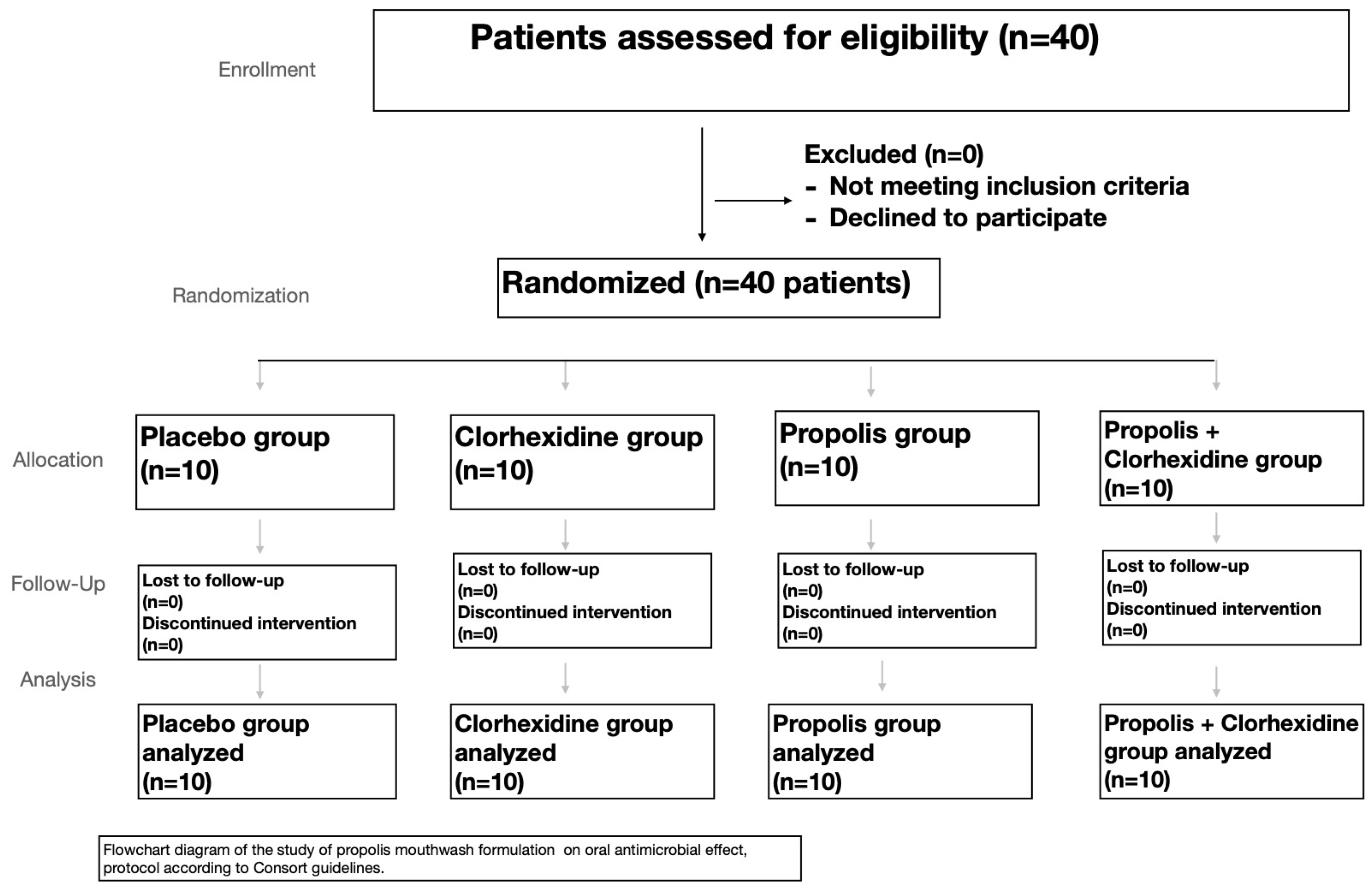
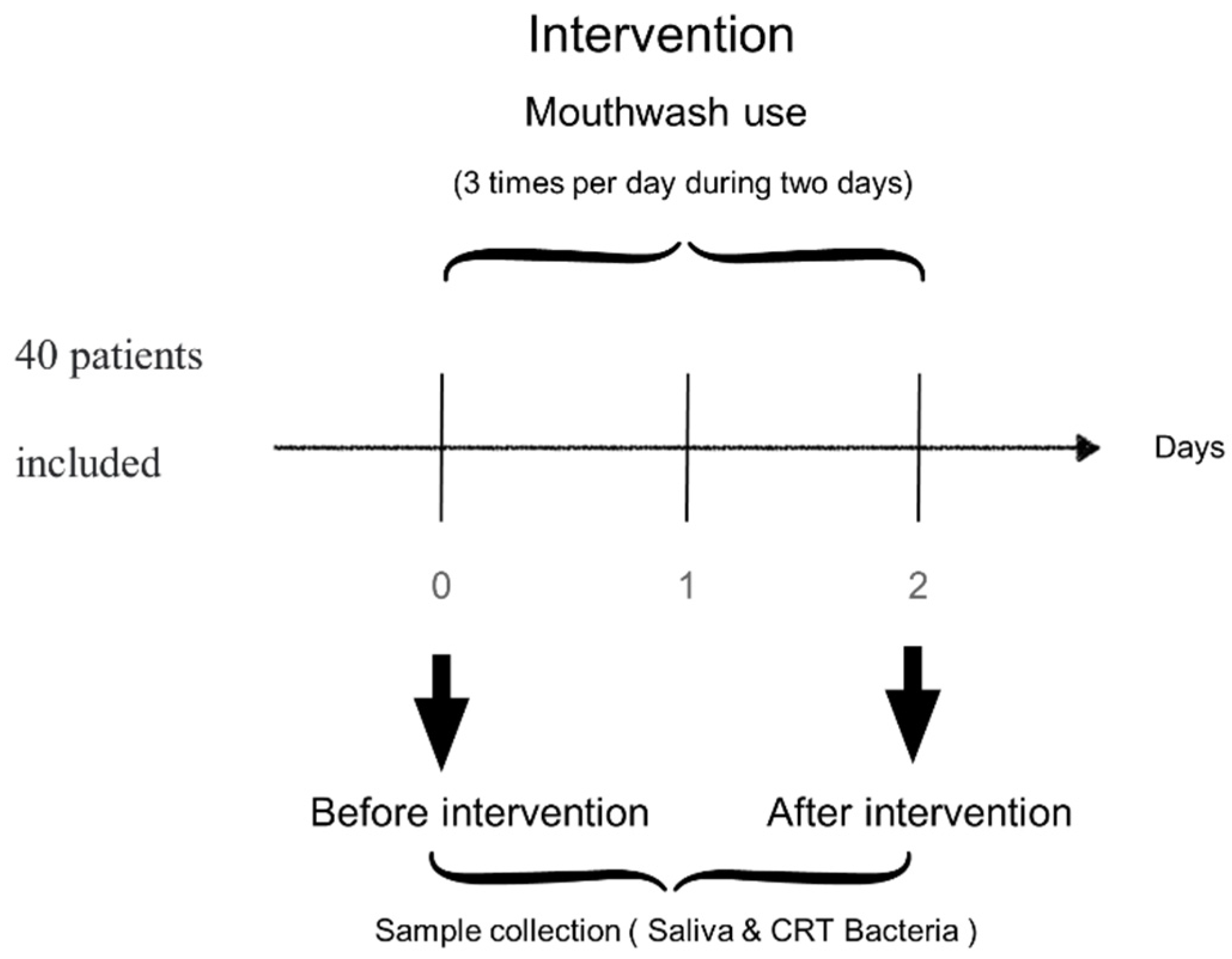
2.2. Mouthwash Assay
3. Discussion
4. Materials and Methods
4.1. Study Protocol and Patients
4.2. Propolis
4.3. Total Phenolic Assay
4.4. Total Flavonoid Assay
4.5. Treatment Methods
4.6. Follow-Up Examination
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Garlet, G.P.; Cardoso, C.R.; Silva, T.A.; Ferreira, B.R.; Ávila-Campos, M.J.; Cunha, F.Q.; Silva, J.S. Cytokine pattern determines the progression of experimental periodontal disease induced by Actinobacillus actinomycetemcomitans through the modulation of MMPs, RANKL, and their physiological inhibitors. Oral Microbiol. Immunol. 2006, 21, 12–20. [Google Scholar] [CrossRef]
- Lockhart, P.B.; Bolger, A.F.; Papapanou, P.N.; Osinbowale, O.; Trevisan, M.; Levison, M.E.; Taubert, K.A.; Newburger, J.W.; Gornik, H.L.; Gewitz, M.H.; et al. Periodontal Disease and Atherosclerotic Vascular Disease: Does the Evidence Support an Independent Association? A scientific statement from the American Heart Association. Circulation 2012, 125, 2520–2544. [Google Scholar] [CrossRef] [PubMed]
- Elkhouli, A.M. The efficacy of host response modulation therapy (omega-3 plus low-dose aspirin) as an adjunctive treatment of chronic periodontitis (Clinical and biochemical study). J. Periodontal Res. 2011, 46, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Dziedzic, A.; Kubina, R.; Wojtyczka, R.D.; Kabała-Dzik, A.; Tanasiewicz, M.; Morawiec, T. The Antibacterial Effect of Ethanol Extract of Polish Propolis on Streptococci mutans and Lactobacilli Isolated from Saliva. Evid. Based Complement. Altern. Med. 2013, 2013, 681891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pretzl, B.; Sälzer, S.; Ehmke, B.; Schlagenhauf, U.; Dannewitz, B.; Dommisch, H.; Eickholz, P.; Jockel-Schneider, Y. Administration of systemic antibiotics during non-surgical periodontal therapy—a consensus report. Clin. Oral Investig. 2019, 23, 3073–3085. [Google Scholar] [CrossRef]
- Hägi, T.; Hofmänner, P.; Salvi, G.; Ramseier, C.A.; Sculean, A. Clinical outcomes following subgingival application of a novel erythritol powder by means of air polishing in supportive periodontal therapy: A randomized, controlled clinical study. Quintessence Int. 2013, 44, 753–761. [Google Scholar] [CrossRef]
- Nilsson, B.O. Mechanisms involved in regulation of periodontal ligament cell production of pro-inflammatory cytokines: Implications in periodontitis. J. Periodontal Res. 2021, 56, 249–255. [Google Scholar] [CrossRef]
- Varoni, E.M.; Lodi, G.; Sardella, A.; Carrassi, A.; Iriti, M. Plant polyphenols and oral health: Old phytochemicals for new fields. Curr. Med. Chem. 2012, 19, 1706–1720. [Google Scholar] [CrossRef]
- Curuțiu, C.; Dițu, L.M.; Grumezescu, A.M.; Holban, A.M. Polyphenols of Honeybee Origin with Applications in Dental Medicine. Antibiotics 2020, 9, 856. [Google Scholar] [CrossRef]
- Al-Hatamleh, M.A.I.; Boer, J.C.; Wilson, K.L.; Plebanski, M.; Mohamud, R.; Mustafa, M.Z. Antioxidant-Based Medicinal Properties of Stingless Bee Products: Recent Progress and Future Directions. Biomolecules 2020, 10, 923. [Google Scholar] [CrossRef]
- Santiago, K.B.; Conti, B.J.; Cardoso, E.D.O.; Golim, M.D.A.; Sforcin, J.M. Immunomodulatory/anti-inflammatory effects of a propolis-containing mouthwash on human monocytes. Pathog. Dis. 2016, 74, ftw081. [Google Scholar] [CrossRef] [Green Version]
- Sforcin, J.M. Biological Properties and Therapeutic Applications of Propolis. Phytother. Res. 2016, 30, 894–905. [Google Scholar] [CrossRef] [PubMed]
- Wade, C.; Friedrich, J.A. Propolis Power Plus: The Health-Promoting Properties of the Amazing Beehive Energizer; Keats Publishing: New Canaan, CT, USA, 1996. [Google Scholar]
- González-Masís, J.; Cubero-Sesin, J.M.; Corrales-Ureña, Y.R.; González-Camacho, S.; Mora-Ugalde, N.; Baizán-Rojas, M.; Loaiza, R.; Vega-Baudrit, J.R.; Gonzalez-Paz, R.J. Increased Fibroblast Metabolic Activity of Collagen Scaffolds via the Addition of Propolis Nanoparticles. Materials 2020, 13, 3118. [Google Scholar] [CrossRef]
- Loureiro, K.C.; Barbosa, T.C.; Nery, M.; Chaud, M.V.; Da Silva, C.F.; Andrade, L.N.; Corrêa, C.B.; Jaguer, A.; Padilha, F.F.; Cardoso, J.C.; et al. Antibacterial activity of chitosan/collagen membranes containing red propolis extract. Pharmazie 2020, 75, 75–81. [Google Scholar] [PubMed]
- Baumann, J.; Wurm, G.; Von Bruchhausen, F. Hemmung der Prostaglandinsynthetase durch Flavonoide und Phenolderivate im Vergleich mit deren O2−•-Radikalfänger-eigenschaften. Arch. Pharm. 1980, 313, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Koo, H.; Gomes, B.P.F.A.; Rosalen, P.L.; Ambrosano, G.M.B.; Park, Y.K.; Cury, J.A. In vitro antimicrobial activity of propolis and Arnica montana against oral pathogens. Arch. Oral Biol. 2000, 45, 141–148. [Google Scholar] [CrossRef]
- Przybyłek, I.; Karpiński, T.M. Antibacterial Properties of Propolis. Molecules 2019, 24, 2047. [Google Scholar] [CrossRef] [Green Version]
- Marcucci, M.C. Propolis: Chemical composition, biological properties and therapeutic activity. Apidologie 1995, 26, 83–99. [Google Scholar] [CrossRef]
- Afra, B.; Mohammadi, M.; Soleimani, M.; Mahjub, R. Preparation, statistical optimization, in vitro characterization, and in vivo pharmacological evaluation of solid lipid nanoparticles encapsulating propolis flavonoids: A novel treatment for skin edema. Drug Dev. Ind. Pharm. 2020, 46, 1163–1176. [Google Scholar] [CrossRef]
- Al-Shaher, A.; Wallace, J.; Agarwal, S.; Bretz, W.; Baugh, D. Effect of Propolis on Human Fibroblasts from the Pulp and Periodontal Ligament. J. Endod. 2004, 30, 359–361. [Google Scholar] [CrossRef]
- Blonska, M.; Bronikowska, J.; Pietsz, G.; Czuba, Z.P.; Scheller, S.; Krol, W. Effects of ethanol extract of propolis (EEP) and its flavones on inducible gene expression in J774A.1 macrophages. J. Ethnopharmacol. 2004, 91, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Song, H.S.; Park, T.W.; Sohn, U.D.; Shin, Y.K.; Choi, B.C.; Kim, C.J.; Sim, S.S. The Effect of Caffeic Acid on Wound Healing in Skin-incised Mice. Korean J. Physiol. Pharmacol. 2008, 12, 343–347. [Google Scholar] [CrossRef] [Green Version]
- Almuhayawi, M.S. Propolis as a novel antibacterial agent. Saudi J. Biol. Sci. 2020, 27, 3079–3086. [Google Scholar] [CrossRef] [PubMed]
- Barroso, P.R.; Lopes-Rocha, R.; Pereira, E.M.; Marinho, S.A.; De Miranda, J.L.; Lima, N.L.; Verli, F.D. Effect of propolis on mast cells in wound healing. Inflammopharmacology 2012, 20, 289–294. [Google Scholar] [CrossRef]
- Moreno, M.I.; Isla, M.I.; Sampietro, A.R.; Vattuone, M.A. Comparison of the free radical-scavenging activity of propolis from several regions of Argentina. J. Ethnopharmacol. 2000, 71, 109–114. [Google Scholar] [CrossRef]
- Castaldo, S.; Capasso, F. Propolis, an old remedy used in modern medicine. Fitoterapia 2002, 73 (Suppl. 1), S1–S6. [Google Scholar] [CrossRef]
- Paulino, N.; Abreu, S.R.; Uto, Y.; Koyama, D.; Nagasawa, H.; Hori, H.; Dirsch, V.; Vollmar, A.M.; Scremin, A.; Bretz, W.A. Anti-inflammatory effects of a bioavailable compound, Artepillin C, in Brazilian propolis. Eur. J. Pharmacol. 2008, 587, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, É.W.; Message, D.; Negri, G.; Salatino, A.; Stringheta, P.C. Seasonal Variation, Chemical Composition and Antioxidant Activity of Brazilian Propolis Samples. Evid. Based Complement. Altern. Med. 2010, 7, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Anjum, S.I.; Ullah, A.; Khan, K.; Attaullah, M.; Khan, H.; Ali, H.; Bashir, M.A.; Tahir, M.; Ansari, M.J.; Ghramh, H.A.; et al. Composition and functional properties of propolis (bee glue): A review. Saudi J. Biol. Sci. 2019, 26, 1695–1703. [Google Scholar] [CrossRef] [PubMed]
- Egozi, E.I.; Bs, A.M.F.; Burns, A.L.; Gamelli, R.L.; DiPietro, L.A. Mast cells modulate the inflammatory but not the proliferative response in healing wounds. Wound Repair Regen. 2003, 11, 46–54. [Google Scholar] [CrossRef]
- Steinberg, D.; Kaine, G.; Gedalia, I. Antibacterial effect of propolis and honey on oral bacteria. Am. J. Dent. 1996, 9, 236–239. [Google Scholar] [PubMed]
- Aabed, K.; Bhat, R.S.; Al-Dbass, A.; Moubayed, N.; Algahtani, N.; Merghani, N.M.; Alanazi, A.; Zayed, N.; El-Ansary, A. Bee pollen and propolis improve neuroinflammation and dysbiosis induced by propionic acid, a short chain fatty acid in a rodent model of autism. Lipids Heal. Dis. 2019, 18, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Ali, K.M.; Saleh, Z.; Jalal, J. Effect of local propolis irrigation in experimental periodontitis in rats on inflammatory markers (IL-1β and TNF-α) and oxidative stress. Indian J. Dent. Res. 2020, 31, 893–898. [Google Scholar] [CrossRef] [PubMed]
- Samet, N.; Laurent, C.; Susarla, S.; Samet-Rubinsteen, N. The effect of bee propolis on recurrent aphthous stomatitis: A pilot study. Clin. Oral Investig. 2007, 11, 143–147. [Google Scholar] [CrossRef]
- Carbajal, D.; Molina, V.; Valdés, S.; Arruzazabala, M.; Más, R.; Magraner, J. Anti-inflammatory activity of D-002: An active product isolated from beeswax. Prostaglandins Leukot. Essent. Fat. Acids 1998, 59, 235–238. [Google Scholar] [CrossRef]
- Khayyal, M.T.; El-Ghazaly, M.A.; El-Khatib, A.; Hatem, A.M.; De Vries, P.J.F.; El-Shafei, S.; Khattab, M.M. A clinical pharmacological study of the potential beneficial effects of a propolis food product as an adjuvant in asthmatic patients. Fundam. Clin. Pharmacol. 2003, 17, 93–102. [Google Scholar] [CrossRef] [Green Version]
- Santos, F.A.; Bastos, E.M.; Uzeda, M.; Carvalho, M.A.; Farias, L.M.; Moreira, E.S.; Braga, F.C. Antibacterial activity of Brazilian propolis and fractions against oral anaerobic bacteria. J. Ethnopharmacol. 2002, 80, 1–7. [Google Scholar] [CrossRef]
- Sonmez, S.; Kirilmaz, L.; Yucesoy, M.; Yücel, B.; Yilmaz, B. The effect of bee propolis on oral pathogens and human gingival fibroblasts. J. Ethnopharmacol. 2005, 102, 371–376. [Google Scholar] [CrossRef]
- Paula, A.M.B.; Gomes, R.T.; Santiago, W.K.; Dias, R.S.; Cortes, M.E.; Santos, V.R. Susceptibility of oral pathogenic bacteria and fungi to brazilian green propolis extract. Pharm. Online 2006, 3, 467–473. [Google Scholar]
- Akca, A.E.; Akca, G.; Topçu, F.T.; Macit, E.; Pikdöken, L.; Özgen, I.S. The Comparative Evaluation of the Antimicrobial Effect of Propolis with Chlorhexidine against Oral Pathogens: An In Vitro Study. BioMed Res. Int. 2016, 2016, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Al-Ani, I.; Zimmermann, S.; Reichling, J.; Wink, M. Antimicrobial Activities of European Propolis Collected from Various Geographic Origins Alone and in Combination with Antibiotics. Medicines 2018, 5, 2. [Google Scholar] [CrossRef] [Green Version]
- De Luca, M.; Franca, J.R.; Macedo, F.A.F.F.; Grenho, L.; Cortés, M.E.; Faraco, A.A.G.; Moreira, A.; Santos, V.R. Propolis Varnish: Antimicrobial Properties against Cariogenic Bacteria, Cytotoxicity, and Sustained-Release Profile. BioMed Res. Int. 2014, 2014, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Özan, F.; Sümer, Z.; Polat, Z.A.; Er, K.; Özan, Ü.; Değer, O. Effect of Mouthrinse Containing Propolis on Oral Microorganisms and Human Gingival Fibroblasts. Eur. J. Dent. 2007, 1, 195–201. [Google Scholar] [CrossRef] [Green Version]
- Galvao, J.; Abreu, J.; Cruz, T.; Machado, G.; Niraldo, P.; Daugsch, A.; Moraes, C.; Fort, P.; Park, Y. Biological Therapy Using Propolis as Nutritional Supplement in Cancer Treatment. Int. J. Cancer Res. 2006, 3, 43–53. [Google Scholar] [CrossRef]
- De Moura, S.A.L.; Ferreira, M.A.N.D.; Andrade, S.P.; Reis, M.L.C.; Noviello, M.D.L.; Cara, D.C. Brazilian Green Propolis Inhibits Inflammatory Angiogenesis in a Murine Sponge Model. Evid. Based Complement. Altern. Med. 2011, 2011, 197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elgamily, H.; Safy, R.; Makharita, R. Influence of Medicinal Plant Extracts on the Growth of Oral Pathogens Streptococcus mutans and Lactobacillus acidophilus: An In-Vitro Study. Open Access Maced. J. Med Sci. 2019, 7, 2328–2334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Awawdeh, L.; Al-Beitawi, M.; Hammad, M. Effectiveness of propolis and calcium hydroxide as a short-term intracanal medicament againstEnterococcus faecalis: A laboratory study. Aust. Endod. J. 2009, 35, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Kandaswamy, D.; Venkateshbabu, N.; Gogulnath, D.; Kindo, A.J. Dentinal tubule disinfection with 2% chlorhexidine gel, propolis, morinda citrifolia juice, 2% povidone iodine, and calcium hydroxide. Int. Endod. J. 2010, 43, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Lisbona, C.; Díaz-Castro, J.; Alférez, M.J.M.; Guisado, I.M.; Guisado, R.; López-Aliaga, I. Positive influence of a natural product as propolis on antioxidant status and lipid peroxidation in senescent rats. J. Physiol. Biochem. 2013, 69, 919–925. [Google Scholar] [CrossRef]
- Lisbona-González, M.J.; Reyes-Botella, C.; Muñoz-Soto, E.; Vallecillo-Rivas, M.; Moreno-Fernández, J.; Díaz-Castro, J. Efecto positivo de un suplemento de propóleo sobre el perfil lipídico, la glucemia y el estado antioxidante hepático en un modelo animal experimental. Nutr. Hosp. 2020, 37, 770–775. [Google Scholar]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89 (Suppl. 1), S159–S172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singleton, V.L.; Orthofer, R.; Lamuela-Raventós, R.M. Analysis of total phenols and other oxidation substrates and an-tioxidants by means of folin-ciocalteu reagent. In Methods in Enzymology; Academic Press: Cambridge, MA, USA, 1999; Volume 299, pp. 152–178. [Google Scholar]
- Madrazo-Jiménez, M.; Rodríguez-Caballero, Á.; Serrera-Figallo, M.; Garrido-Serrano, R.; Gutiérrez-Corrales, A.; Gutiérrez-Pérez, J.L.; Torres-Lagares, D. The effects of a topical gel containing chitosan, 0.2% chlorhexidine, allantoin and despanthenol on the wound healing process subsequent to impacted lower third molar extraction. Med. Oral Patol. Oral Cir. Bucal 2016, 21, e696–e702. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Day 3 | Day 4 | Day 7 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| n (% Sockets) | p-Value | n (% Sockets) | p-Value | n (% Sockets) | p-Value | ||||
| Control | Test | Control | Test | Control | Test | ||||
| Completely healed | 8 (13.3) | 38 (63.3) | <0.001 | 14 (23.4) | 42 (70.0) | <0.001 | 36 (60.0) | 60 (100) | <0.001 |
| Partial closure | 18 (30.0) | 16 (26.7) | 0.096 | 38 (60.0) | 18 (30.0) | <0.001 | 24 (40.0) | - | <0.001 |
| Granulation tissue | 34 (56.7) | 6 (10.0) | <0.001 | 8 (13.3) | - | 0.03 | - | - | - |
| Mouthwash | Baseline | 48 h | ||
|---|---|---|---|---|
| Score (%) | Score (%) | |||
| S. mutans | Lactobacillus spp. | S. mutans | Lactobacillus spp. | |
| Placebo n = 10 | 2 (100) | 3 (100) | 2 (100) | 3 (100) |
| Clorhexidine 0.2% n = 10 | 2 (100) | 3 (100) | 2 (20) 1 (80) | 2 (100) |
| Propolis 2% n = 10 | 2 (100) | 3 (100) | 2 (40) 1 (60) | 2 (50) 3 (50) |
| Clorhexidina 0.2% + Propolis 2% n = 10 | 2 (100) | 3 (100) | 1 (100) | 1 (100) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lisbona-González, M.J.; Muñoz-Soto, E.; Lisbona-González, C.; Vallecillo-Rivas, M.; Diaz-Castro, J.; Moreno-Fernandez, J. Effect of Propolis Paste and Mouthwash Formulation on Healing after Teeth Extraction in Periodontal Disease. Plants 2021, 10, 1603. https://doi.org/10.3390/plants10081603
Lisbona-González MJ, Muñoz-Soto E, Lisbona-González C, Vallecillo-Rivas M, Diaz-Castro J, Moreno-Fernandez J. Effect of Propolis Paste and Mouthwash Formulation on Healing after Teeth Extraction in Periodontal Disease. Plants. 2021; 10(8):1603. https://doi.org/10.3390/plants10081603
Chicago/Turabian StyleLisbona-González, Maria Jesús, Esther Muñoz-Soto, Cristina Lisbona-González, Marta Vallecillo-Rivas, Javier Diaz-Castro, and Jorge Moreno-Fernandez. 2021. "Effect of Propolis Paste and Mouthwash Formulation on Healing after Teeth Extraction in Periodontal Disease" Plants 10, no. 8: 1603. https://doi.org/10.3390/plants10081603