
Alveolar Bone Ridge Augmentation Using Polymeric Membranes: A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Development of the Protocol
2.2. Search Strategy, Data Extraction, and Studies Quality Assessment
2.3. Data Analyses
3. Results
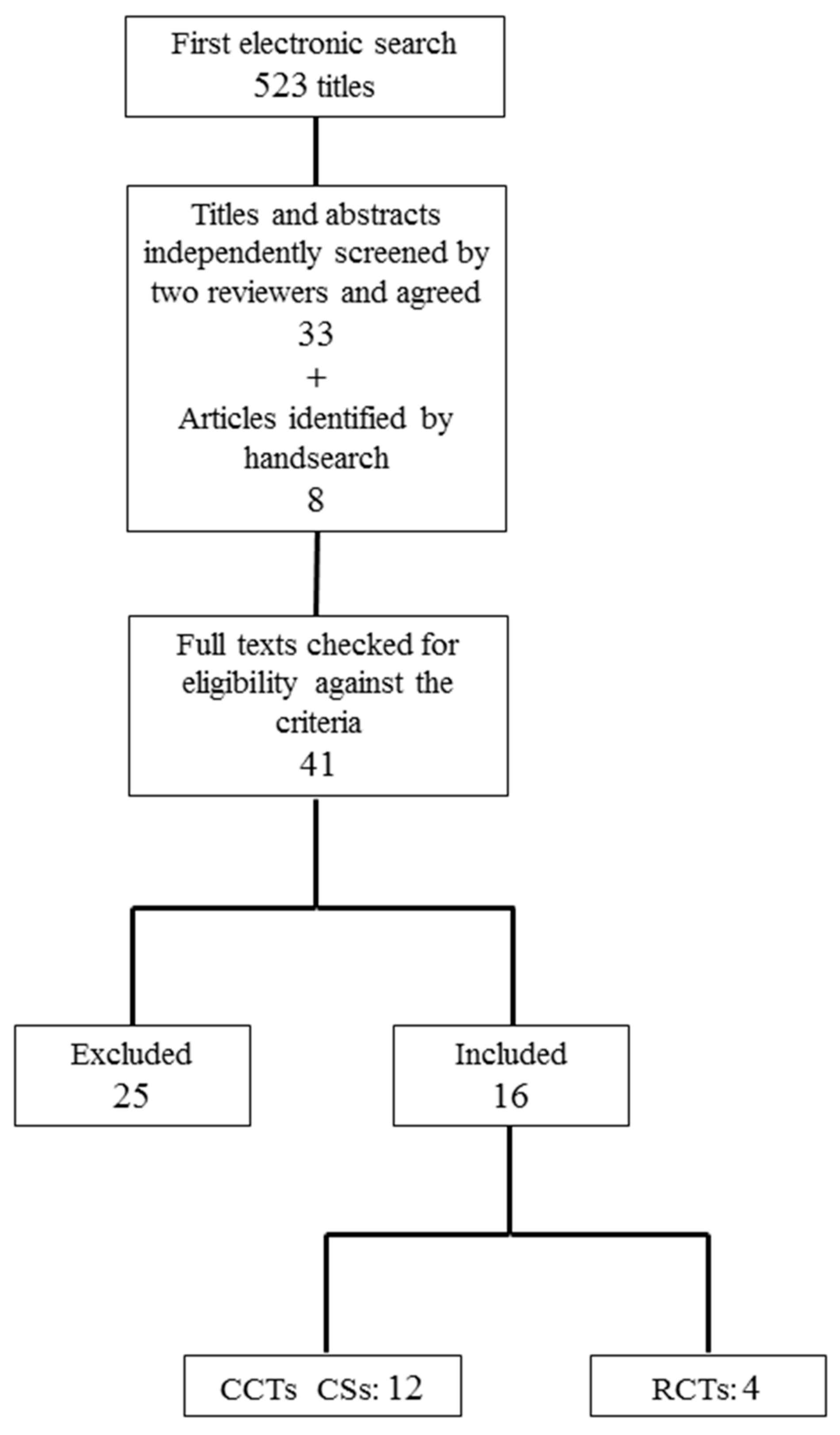
3.1. Search Results
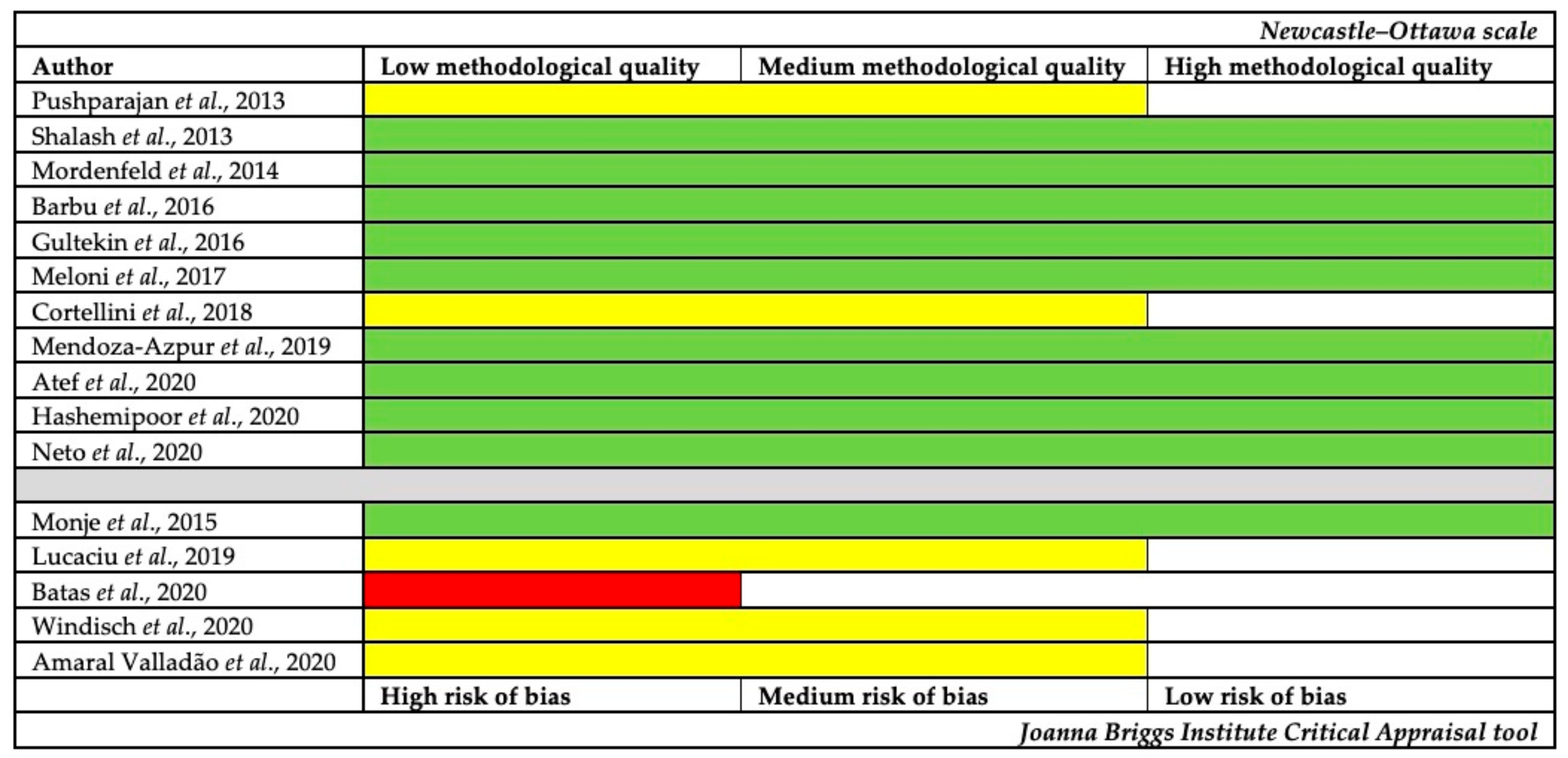
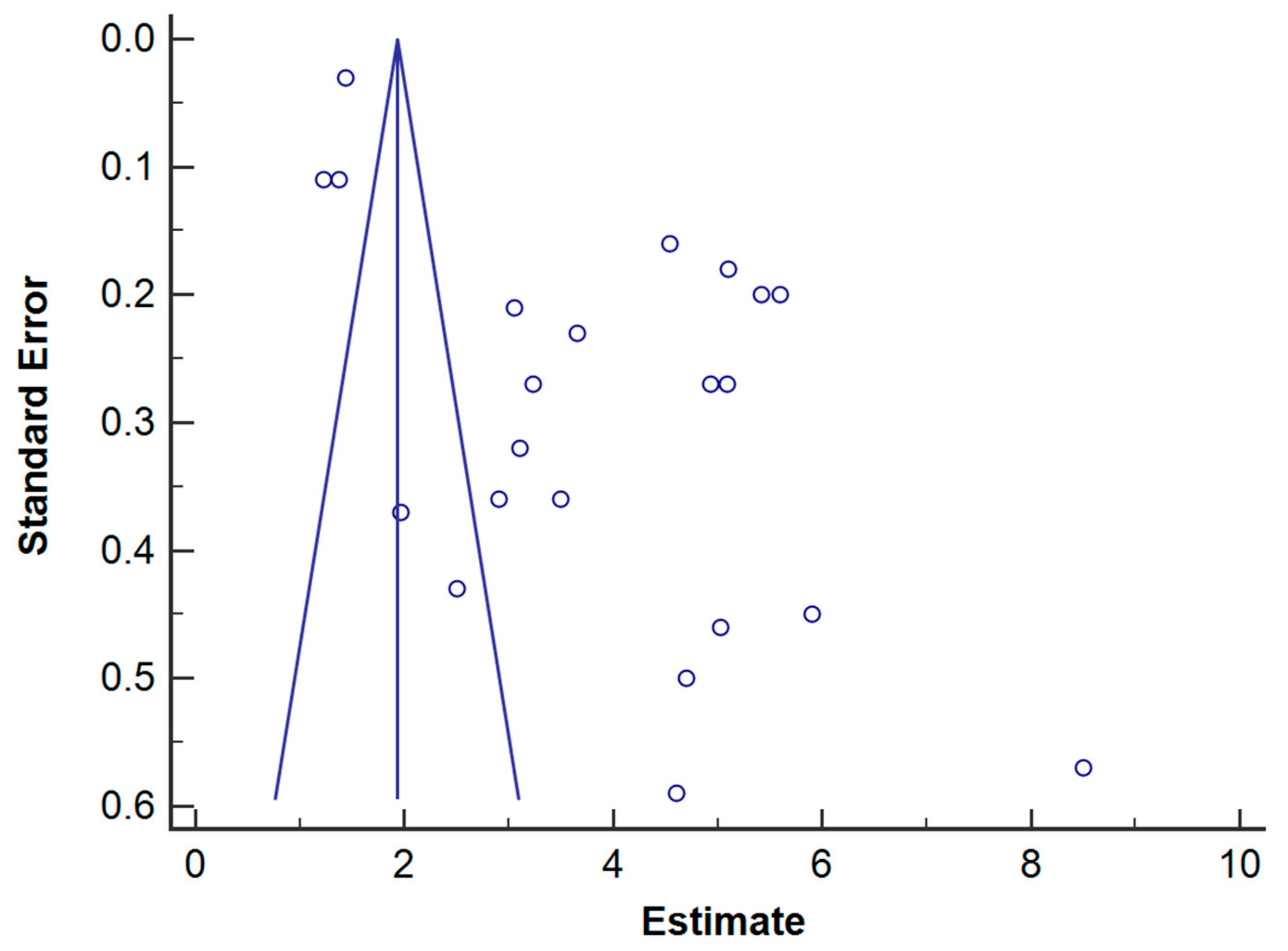
3.2. Studies Quality Assessment and Risk of Bias
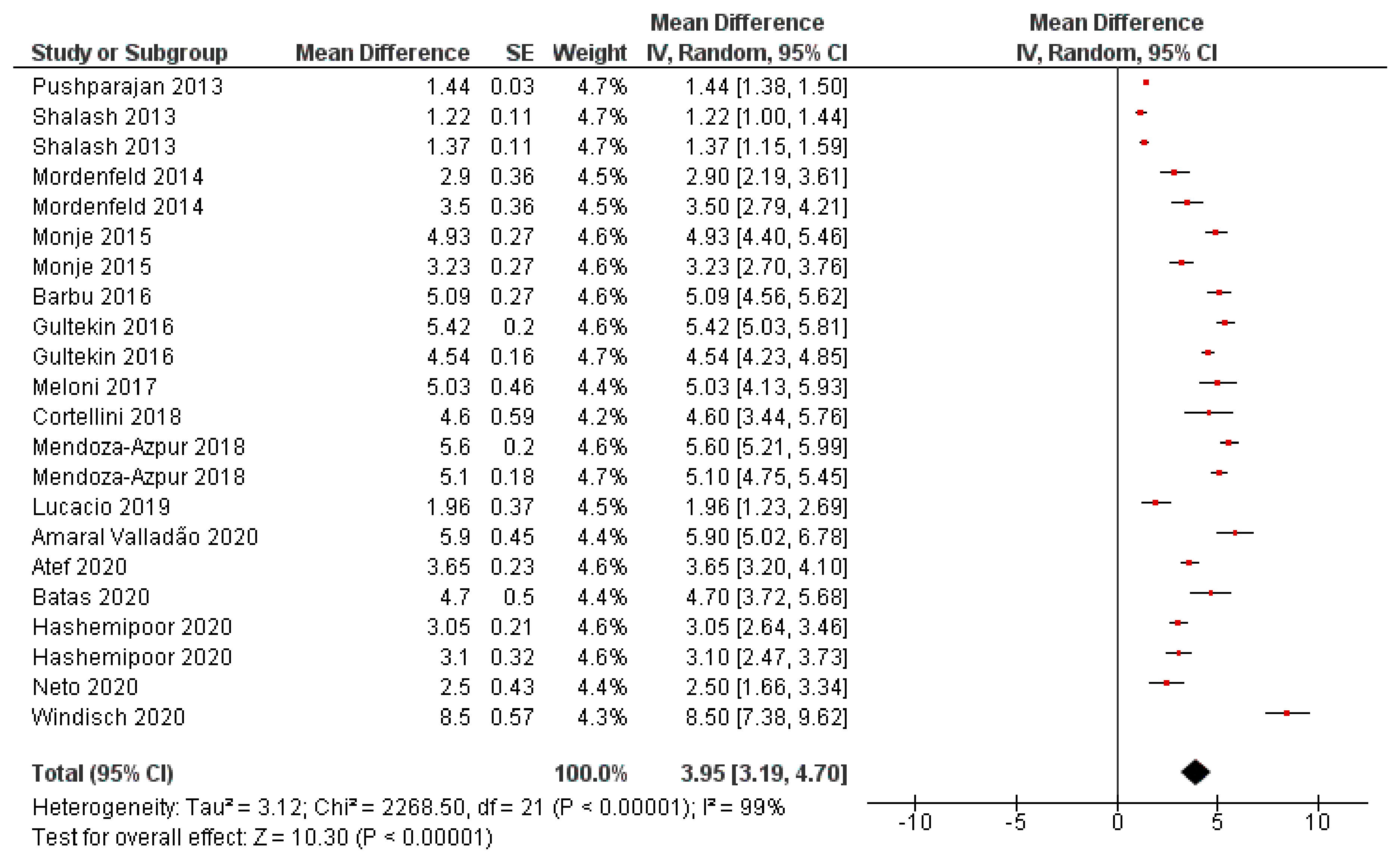
3.3. Primary and Secondary Outcomes: Horizontal Bone Gain and Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barbu, H.M.; Andreescu, C.F.; Lorean, A.; Kolerman, R.; Moraru, L.; Mortellaro, C.; Mijiritsky, E. Comparison of Two Techniques for Lateral Ridge Augmentation in Mandible With Ramus Block Graft. J. Craniofac. Surg. 2016, 27, 662–667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Azambuja Carvalho, P.H.; Dos Santos Trento, G.; Moura, L.B.; Cunha, G.; Gabrielli, M.A.C.; Pereira-Filho, V.A. Horizontal Ridge Augmentation Using Xenogenous Bone Graft-Systematic Review. Oral. Maxillofac. Surg. 2019, 23, 271–279. [Google Scholar] [CrossRef]
- Garaicoa, C.; Suarez, F.; Fu, J.-H.; Chan, H.-L.; Monje, A.; Galindo-Moreno, P.; Wang, H.-L. Using Cone Beam Computed Tomography Angle for Predicting the Outcome of Horizontal Bone Augmentation. Clin. Implant Dent. Relat. Res. 2015, 17, 717–723. [Google Scholar] [CrossRef]
- Sbricoli, L.; Guazzo, R.; Annunziata, M.; Gobbato, L.; Bressan, E.; Nastri, L. Selection of Collagen Membranes for Bone Regeneration: A Literature Review. Materials 2020, 13, 786. [Google Scholar] [CrossRef] [Green Version]
- Sanz, M.; Dahlin, C.; Apatzidou, D.; Artzi, Z.; Bozic, D.; Calciolari, E.; Bruyn, H.D.; Dommisch, H.; Donos, N.; Eickholz, P.; et al. Biomaterials and Regenerative Technologies Used in Bone Regeneration in the Craniomaxillofacial Region: Consensus Report of Group 2 of the 15th European Workshop on Periodontology on Bone Regeneration. J. Clin. Periodontol. 2019, 46, 82–91. [Google Scholar] [CrossRef]
- Thoma, D.S.; Bienz, S.P.; Figuero, E.; Jung, R.E.; Sanz-Martín, I. Efficacy of Lateral Bone Augmentation Performed Simultaneously with Dental Implant Placement: A Systematic Review and Meta-Analysis. J. Clin. Periodontol. 2019, 46 (Suppl. S21), 257–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melcher, A.H. On the Repair Potential of Periodontal Tissues. J. Periodontol. 1976, 47, 256–260. [Google Scholar] [CrossRef]
- Zitzmann, N.U.; Naef, R.; Schärer, P. Resorbable versus Nonresorbable Membranes in Combination with Bio-Oss for Guided Bone Regeneration. Int. J. Oral Maxillofac. Implants 1997, 12, 844–852. [Google Scholar] [PubMed]
- Makvandi, P.; Gu, J.T.; Zare, E.N.; Ashtari, B.; Moeini, A.; Tay, F.R.; Niu, L. Polymeric and Inorganic Nanoscopical Antimicrobial Fillers in Dentistry. Acta Biomater. 2020, 101, 69–101. [Google Scholar] [CrossRef]
- Makvandi, P.; Josic, U.; Delfi, M.; Pinelli, F.; Jahed, V.; Kaya, E.; Ashrafizadeh, M.; Zarepour, A.; Rossi, F.; Zarrabi, A.; et al. Drug Delivery (Nano)Platforms for Oral and Dental Applications: Tissue Regeneration, Infection Control, and Cancer Management. Adv. Sci. 2021, 2004014. [Google Scholar] [CrossRef]
- Bueno, J.; Sánchez, M.d.C.; Toledano-Osorio, M.; Figuero, E.; Toledano, M.; Medina-Castillo, A.L.; Osorio, R.; Herrera, D.; Sanz, M. Antimicrobial Effect of Nanostructured Membranes for Guided Tissue Regeneration: An in Vitro Study. Dent. Mater. 2020, 36, 1566–1577. [Google Scholar] [CrossRef] [PubMed]
- Toledano, M.; Toledano-Osorio, M.; Osorio, R.; Carrasco-Carmona, Á.; Gutiérrez-Pérez, J.-L.; Gutiérrez-Corrales, A.; Serrera-Figallo, M.-A.; Lynch, C.D.; Torres-Lagares, D. Doxycycline and Zinc Loaded Silica-Nanofibrous Polymers as Biomaterials for Bone Regeneration. Polymers 2020, 12, 1201. [Google Scholar] [CrossRef]
- Toledano, M.; Gutierrez-Pérez, J.L.; Gutierrez-Corrales, A.; Serrera-Figallo, M.A.; Toledano-Osorio, M.; Rosales-Leal, J.I.; Aguilar, M.; Osorio, R.; Torres-Lagares, D. Novel Non-Resorbable Polymeric-Nanostructured Scaffolds for Guided Bone Regeneration. Clin. Oral Investig. 2020, 24, 2037–2049. [Google Scholar] [CrossRef]
- Mir-Mari, J.; Wui, H.; Jung, R.E.; Hämmerle, C.H.F.; Benic, G.I. Influence of Blinded Wound Closure on the Volume Stability of Different GBR Materials: An in Vitro Cone-Beam Computed Tomographic Examination. Clin. Oral Implants Res. 2016, 27, 258–265. [Google Scholar] [CrossRef]
- Tavelli, L.; Ravidà, A.; Barootchi, S.; Chambrone, L.; Giannobile, W.V. Recombinant Human Platelet-Derived Growth Factor: A Systematic Review of Clinical Findings in Oral Regenerative Procedures. JDR Clin. Trans. Res. 2020. [Google Scholar] [CrossRef]
- Pushparajan, S.; Thiagarajan, R.; Namasi, A.; Emmadi, P.; Saravanan, H. Efficacy of Guided Bone Regeneration Using Composite Bone Graft and Resorbable Collagen Membrane in Seibert’s Class I Ridge Defects: Radiological Evaluation. J. Oral Implantol. 2013, 39, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Shalash, M.A.; Rahman, H.A.; Azim, A.A.; Neemat, A.H.; Hawary, H.E.; Nasry, S.A. Evaluation of Horizontal Ridge Augmentation Using Beta Tricalcium Phosphate and Demineralized Bone Matrix: A Comparative Study. J. Clin. Exp. Dent. 2013, 5, e253–e259. [Google Scholar] [CrossRef] [PubMed]
- Mordenfeld, A.; Johansson, C.B.; Albrektsson, T.; Hallman, M. A Randomized and Controlled Clinical Trial of Two Different Compositions of Deproteinized Bovine Bone and Autogenous Bone Used for Lateral Ridge Augmentation. Clin. Oral Implants Res. 2014, 25, 310–320. [Google Scholar] [CrossRef]
- Monje, A.; Monje, F.; Hernández-Alfaro, F.; Gonzalez-García, R.; Suárez-López del Amo, F.; Galindo-Moreno, P.; Montanero-Fernández, J.; Wang, H.-L. Horizontal Bone Augmentation Using Autogenous Block Grafts and Particulate Xenograft in the Severe Atrophic Maxillary Anterior Ridges: A Cone-Beam Computerized Tomography Case Series. J. Oral Implants 2015, 41, 366–371. [Google Scholar] [CrossRef]
- Gultekin, B.A.; Bedeloglu, E.; Kose, T.E.; Mijiritsky, E. Comparison of Bone Resorption Rates after Intraoral Block Bone and Guided Bone Regeneration Augmentation for the Reconstruction of Horizontally Deficient Maxillary Alveolar Ridges. Biomed. Res. Int. 2016, 2016, 4987437. [Google Scholar] [CrossRef] [Green Version]
- Meloni, S.M.; Jovanovic, S.A.; Urban, I.; Canullo, L.; Pisano, M.; Tallarico, M. Horizontal Ridge Augmentation Using GBR with a Native Collagen Membrane and 1:1 Ratio of Particulated Xenograft and Autologous Bone: A 1-Year Prospective Clinical Study. Clin. Implant Dent. Relat. Res. 2017, 19, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, S.; Castro, A.B.; Temmerman, A.; Van Dessel, J.; Pinto, N.; Jacobs, R.; Quirynen, M. Leucocyte- and Platelet-Rich Fibrin Block for Bone Augmentation Procedure: A Proof-of-Concept Study. J. Clin. Periodontol. 2018, 45, 624–634. [Google Scholar] [CrossRef]
- Mendoza-Azpur, G.; de la Fuente, A.; Chavez, E.; Valdivia, E.; Khouly, I. Horizontal Ridge Augmentation with Guided Bone Regeneration Using Particulate Xenogenic Bone Substitutes with or without Autogenous Block Grafts: A Randomized Controlled Trial. Clin. Implant Dent. Relat. Res. 2019, 21, 521–530. [Google Scholar] [CrossRef]
- Lucaciu, O.; Apostu, D.; Mester, A.; Campian, R.S.; Gheban, D.; Miron, R.J. Atelo-Collagen Type I Bovine Bone Substitute and Membrane in Guided Bone Regeneration: A Series of Clinical Cases and Histopathological Assessments. Histol. Histopathol. 2019, 34, 1061–1071. [Google Scholar] [CrossRef]
- Amaral Valladão, C.A.; Freitas Monteiro, M.; Joly, J.C. Guided Bone Regeneration in Staged Vertical and Horizontal Bone Augmentation Using Platelet-Rich Fibrin Associated with Bone Grafts: A Retrospective Clinical Study. Int. J. Implant Dent. 2020, 6, 72. [Google Scholar] [CrossRef] [PubMed]
- Atef, M.; Tarek, A.; Shaheen, M.; Alarawi, R.M.; Askar, N. Horizontal Ridge Augmentation Using Native Collagen Membrane vs Titanium Mesh in Atrophic Maxillary Ridges: Randomized Clinical Trial. Clin. Implant Dent. Relat. Res. 2020, 22, 156–166. [Google Scholar] [CrossRef] [PubMed]
- Batas, L.; Anagnostou, E.; Vouros, I. Evaluation of a Double Layer Technique to Enhance Bone Formation in Atrophic Alveolar Ridge: Histologic Results of a Pilot Study. J. Oral Maxillofac. Surg. 2020, 78, 2195–2207. [Google Scholar] [CrossRef] [PubMed]
- Hashemipoor, M.; Asghari, N.; Mohammadi, M.; Kalantari, M.; Arabsolghar, M.; Ranjbar, H. Radiological and Histological Evaluation of Horizontal Ridge Augmentation Using Corticocancellous Freeze-Dried Bone Allograft with and without Autogenous Bone: A Randomized Controlled Clinical Trial. Clin. Implant Dent. Relat. Res. 2020, 22, 582–592. [Google Scholar] [CrossRef]
- César Neto, J.B.; Cavalcanti, M.C.; Sapata, V.M.; Pannuti, C.M.; Hämmerle, C.H.F.; Naenni, N.; Thoma, D.S.; Romito, G.A. The Positive Effect of Tenting Screws for Primary Horizontal Guided Bone Regeneration: A Retrospective Study Based on Cone-Beam Computed Tomography Data. Clin. Oral Implants Res. 2020, 31, 846–855. [Google Scholar] [CrossRef] [PubMed]
- Windisch, P.; Orban, K.; Salvi, G.E.; Sculean, A.; Molnar, B. Vertical-Guided Bone Regeneration with a Titanium-Reinforced d-PTFE Membrane Utilizing a Novel Split-Thickness Flap Design: A Prospective Case Series. Clin. Oral Investig. 2020. [Google Scholar] [CrossRef]
- Ritter, L.; Elger, M.C.; Rothamel, D.; Fienitz, T.; Zinser, M.; Schwarz, F.; Zöller, J.E. Accuracy of Peri-Implant Bone Evaluation Using Cone Beam CT, Digital Intra-Oral Radiographs and Histology. Dentomaxillofac. Radiol. 2014, 43, 20130088. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, E.; Elluru, S.V. Cone Beam Computed Tomography: Basics and Applications in Dentistry. J. Istanb. Univ. Fac. Dent. 2017, 51, S102–S121. [Google Scholar] [CrossRef] [PubMed]
- Almog, D.M.; LaMar, J.; LaMar, F.R.; LaMar, F. Cone Beam Computerized Tomography-Based Dental Imaging for Implant Planning and Surgical Guidance, Part 1: Single Implant in the Mandibular Molar Region. J. Oral Implants 2006, 32, 77–81. [Google Scholar] [CrossRef]
- Nickenig, H.-J.; Eitner, S. Reliability of Implant Placement after Virtual Planning of Implant Positions Using Cone Beam CT Data and Surgical (Guide) Templates. J. Craniomaxillofac. Surg. 2007, 35, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Tischler, M. In-Office Cone Beam Computerized Tomography: Technology Review and Clinical Examples. Dent. Today 2008, 27, 102–106. [Google Scholar] [PubMed]
- Zhang, Y.; Zhang, X.; Shi, B.; Miron, R. Membranes for Guided Tissue and Bone Regeneration. Oral Maxillofac. Surg. 2013, 1, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Calciolari, E.; Ravanetti, F.; Strange, A.; Mardas, N.; Bozec, L.; Cacchioli, A.; Kostomitsopoulos, N.; Donos, N. Degradation Pattern of a Porcine Collagen Membrane in an in Vivo Model of Guided Bone Regeneration. J. Periodontal. Res. 2018, 53, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Kilinc, A.; Ataol, M. How Effective Is Collagen Resorbable Membrane Placement after Partially Impacted Mandibular Third Molar Surgery on Postoperative Morbidity? A Prospective Randomized Comparative Study. BMC Oral Health 2017, 17, 126. [Google Scholar] [CrossRef] [Green Version]
- Toledano, M.; Asady, S.; Toledano-Osorio, M.; García-Godoy, F.; Serrera-Figallo, M.-A.; Benítez-García, J.A.; Osorio, R. Differential Biodegradation Kinetics of Collagen Membranes for Bone Regeneration. Polymers 2020, 12, 1290. [Google Scholar] [CrossRef]
- Urban, I.A.; Montero, E.; Monje, A.; Sanz-Sánchez, I. Effectiveness of Vertical Ridge Augmentation Interventions: A Systematic Review and Meta-Analysis. J. Clin. Periodontol. 2019, 46 (Suppl. S21), 319–339. [Google Scholar] [CrossRef] [Green Version]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sideri, S.; Papageorgiou, S.N.; Eliades, T. Registration in the International Prospective Register of Systematic Reviews (PROSPERO) of Systematic Review Protocols Was Associated with Increased Review Quality. J. Clin. Epidemiol. 2018, 100, 103–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Study Design | Patients GBRs | Bone Substitute | Membrane | Follow-Up Time | BG (mm) Mean (SD) | Complications |
|---|---|---|---|---|---|---|---|
| Pushparajan et al., 2013 [16] | CCT | 10 patients 10 GBRs | DBBM particles Autogenous | Collagen | 6 months | 1.44 (0.09) | Not reported |
| Shalash et al., 2013 [17] | CCT | 10 patients 10 GBRs | β-TCP particles | d-PTFE | 6 months | 1.22 (0.35) | 2 membrane exposures |
| 10 patients 10 GBRs | β-TCP particles DBBM particles | d-PTFE | 1.37 (0.35) | ||||
| Mordenfeld et al., 2014 [18] | RCT | 13 patients 13 GBRs | DBBM particles (90) Autogenous (10) | Collagen | 7.5 months | 2.9 (1.3) | 7 dehiscences |
| 13 patients 13 GBRs | DBBM particles (60) Autogenous (40) | Collagen | 3.5 (1.3) | ||||
| Monje et al., 2015 [19] | CS | 6 patients 9 GBRs | Illiac crest block DBBM particles | Collagen | 5 months | 4.93 (0.65) | Not reported |
| 8 patients 10 GBRs | Mandib ramus block DBBM particles | Collagen | 3.23 (0.76) | ||||
| Barbu et al., 2016 [1] | RCT | 11 patients 11 GBRs | Mandib ramus block DBBM particles + Autogenous | Pericardium | 4 months | 5.10 (0. 91) | 3 patients with pain in donor site |
| Gultekin et al., 2016 [20] | CCT | 12 patients 15 GBRs | DBBM particles Autogenous | Collagen | 4–7 months | 5.42 (0.76) | 1 dehiscence |
| 12 patients 13 GBRs | Mandib ramus block DBBM particles | Collagen | 4.54 (0.59) | ||||
| Meloni et al., 2017 [21] | CCT | 18 patients 22 GBRs | DBBM particles Autogenous | Collagen | 7 months | 5.03 (2.15) | 3 membrane exposures |
| Cortellini et al., 2018 [22] | CCT | 10 patients 15 GBRs | L-PRF + DBBM particles | Collagen | 5–8 months | 4.6 (2.3) | 1 dehiscence |
| Mendoza-Azpur et al., 2019 [23] | RCT | 20 patients 20 GBRs | DBBM particles Autogenous | Collagen | 6 months | 5.6 (0.89) | 6 membrane exposures 1 infection |
| 19 patients 19 GBRs | Mandib ramus block DBBM particles | Collagen | 5.10 (0.77) | ||||
| Lucaciu et al., 2019 [24] | CS | 13 patients 20 GBRs | ABBM particles Autogenous | Collagen | 4 months | 1.96 (1.64) | Not reported |
| Amaral Valladão et al., 2020 [25] | CS | 18 patients 29 GBRs | L-PRF DBBM particles Autogenous | Collagen | 7.5–8.5 months | 5.9 (2.4) | Not reported |
| Atef et al., 2020 [26] | RCT | 10 patients 10 GBRs | ABBM particles Autogenous | Collagen | 6 months | 3.65 (1.04) | 1 membrane exposure 1 infection |
| Batas et al., 2020 [27] | CS | 6 patients 6 GBRs | Allogenic bone DBBM particles | Collagen | 5 months | 4.7 (1.22) | Not reported |
| Hashemipoor et al., 2020 [28] | RCT | 21 patients 21 GBRs | FDBA | Collagen | 6 months | 3.05 (0.98) | 1 membrane exposure |
| 19 patients 19 GBRs | FDBA Autogenous | Collagen | 3.10 (1.4) | ||||
| Neto et al., 2020 [29] | CCT | 18 patients 22 GBRs | DBBM particles | Collagen | 6–8 months | 2.5 (2.02) | 1 membrane exposure |
| Windisch et al., 2020 [30] | CS | 15 patients 18 GBRs | DBBM particles Autogenous | d-PTFE | 9 months | 8.5 (2.4) | 1 membrane exposure |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toledano-Osorio, M.; Toledano, M.; Manzano-Moreno, F.J.; Vallecillo, C.; Vallecillo-Rivas, M.; Rodriguez-Archilla, A.; Osorio, R. Alveolar Bone Ridge Augmentation Using Polymeric Membranes: A Systematic Review and Meta-Analysis. Polymers 2021, 13, 1172. https://doi.org/10.3390/polym13071172
Toledano-Osorio M, Toledano M, Manzano-Moreno FJ, Vallecillo C, Vallecillo-Rivas M, Rodriguez-Archilla A, Osorio R. Alveolar Bone Ridge Augmentation Using Polymeric Membranes: A Systematic Review and Meta-Analysis. Polymers. 2021; 13(7):1172. https://doi.org/10.3390/polym13071172
Chicago/Turabian StyleToledano-Osorio, Manuel, Manuel Toledano, Francisco Javier Manzano-Moreno, Cristina Vallecillo, Marta Vallecillo-Rivas, Alberto Rodriguez-Archilla, and Raquel Osorio. 2021. "Alveolar Bone Ridge Augmentation Using Polymeric Membranes: A Systematic Review and Meta-Analysis" Polymers 13, no. 7: 1172. https://doi.org/10.3390/polym13071172