Enhanced Accuracy of Continuous Glucose Monitoring during Exercise through Physical Activity Tracking Integration


1
Centro de Investigación Biomédica en Red de Diabetes y Enfermedades Metabólicas Asociadas (CIBERDEM), Instituto de Salud Carlos III, 28029 Madrid, Spain
2
Institut Universitari d’Automàtica i Informàtica Industrial, Universitat Politècnica de València, Camino de Vera, s/n, 46022 València, Spain
3
Diabetes Unit, Endocrinology and Nutrition Department, Hospital Clínic Universitari, IDIBAPS (Institut d’investigacions Biomèdiques August Pi i Sunyer), 08036 Barcelona, Spain
*
Author to whom correspondence should be addressed.
Sensors 2019, 19(17), 3757; https://doi.org/10.3390/s19173757
Submission received: 29 July 2019
/
Revised: 21 August 2019
/
Accepted: 27 August 2019
/
Published: 30 August 2019
(This article belongs to the Special Issue Wearable Sensors in Healthcare: Methods, Algorithms, Applications)
Abstract
:Current Continuous Glucose Monitors (CGM) exhibit increased estimation error during periods of aerobic physical activity. The use of readily-available exercise monitoring devices opens new possibilities for accuracy enhancement during these periods. The viability of an array of physical activity signals provided by three different wearable devices was considered. Linear regression models were used in this work to evaluate the correction capabilities of each of the wearable signals and propose a model for CGM correction during exercise. A simple two-input model can reduce CGM error during physical activity (17.46% vs. 13.8%, p < 0.005) to the magnitude of the baseline error level (13.61%). The CGM error is not worsened in periods without physical activity. The signals identified as optimal inputs for the model are “Mets” (Metabolic Equivalent of Tasks) from the Fitbit Charge HR device, which is a normalized measurement of energy expenditure, and the skin temperature reading provided by the Microsoft Band 2 device. A simpler one-input model using only “Mets” is also viable for a more immediate implementation of this correction into market devices.
1. Introduction
Diabetes Mellitus is a disease characterized by a dysregulation of the natural homeostasis of glucose concentration in the body. It has a projected prevalence of 9.9% of the global population by 2045 (629 million people affected), and the estimated yearly cost in healthcare expenditure by the same year is 776 billion USD [1]. Approximately 10% of the people that have diabetes suffer from type 1 diabetes, which has a very early onset, usually manifesting during childhood or adolescence, and requires intensive supervision and treatment of the disease. Type 1 Diabetes (T1D) is defined by the inability of the beta cells of the pancreas to produce insulin in the bloodstream partially or totally, which leads to abnormally high levels of blood glucose. This problem worsens during periods of meal ingestion, in which glucose is poured into the bloodstream through the gut, or during physical activity or stress, which alter uptake or production of glucose in different parts of the body.
An Artificial Pancreas (AP) is a device that feeds continuous glucose measurements into an insulin pump in real time and continuously adjusts insulin dosage delivered to the patient. It is one the most promising solutions to the complications of T1D, and several prototypes have been under development over the last few years, including commercially-available [2] devices. Physical activity has been linked to changes in glucose trends and variability in patients with diabetes [3,4]. The accuracy of glucose measurement is of great importance for the correct performance of AP devices, since it drives the decision making of the algorithms behind it. The accuracy of Continuous Glucose Monitoring (CGM) devices has been observed to be affected during exercise periods. Taleb et al. [5] showed that both Dexcom G4 and Medtronic Enlite devices’ accuracy dropped during aerobic physical activity when compared to reference glucose measurements. Increased CGM error has been found consistently during aerobic exercise, even among the more recently distributed devices in the market [6]. Biagi et al. [7] showed that the accuracy of Medtronic Enlite 2 devices dropped both during aerobic and anaerobic exercise, but only the results during aerobic exercise were significantly different. This conclusion has also been reported in the literature before [5,8], which suggests an underlying problem with the mechanism of glucose estimation in the subcutaneous tissue during periods of physical activity.
Exercise monitoring is widespread today in most parts of the world, with many different devices designed and marketed to provide estimation of the intensity, type, and duration of physical activity. Integration of all available signals from wearable physical activity monitors (wearables) remains an open issue [9], and many of the wearable signals are only able to be extracted as processed variables. The use of wearable devices to improve T1D management has been reviewed before [10], and many studies have been conducted by adding different isolated wearable variables into AP controller algorithms [11], supervision algorithms [12], or prediction and classification algorithms [13,14]. Turksoy [15] studied the influence of wearable signals (named biometric variables in the reference) in the context of their possible implementation in an artificial pancreas system, showing that the amount of information carried by each signal changes depending on the type of exercise performed and placing special importance on the estimation of total energy spent by the physical activity.
The motivation for this work arises from the possibility of compensating the greater estimation error shown during exercise periods. Our working hypothesis is that exercise monitoring devices could provide information to a CGM device that allows for a real-time correction of the shift in glucose estimation during physical activity. The work presented in this paper analyzes the influence of the different signals provided by three different wearables (Fitbit Charge HR, Microsoft Band 2, and Polar HR) on the accuracy of a CGM device during aerobic exercise. Each wearable signal is critically selected or discarded as input for a multiple regression model designed to compensate the measurement error induced by the exercise session. The final regression model improves the accuracy of the CGM signal significantly during the exercise period, and baseline accuracy is maintained during the resting period. It is shown here that only two wearable signals are necessary to enhance the CGM measurements, and that redundancy of sensors only marginally increases the accuracy of the CGM estimations.
This paper is structured as follows. First, a breakdown of the methods, models, protocol, and datasets used is provided, including a brief description of all the devices employed in the study. Secondly, the results of the validation of the model utilized will be provided, along with the critical selection of signals to be used in the model. Then, a critical discussion of the results will be exposed, followed by the final conclusions.
2. Materials and Methods
2.1. Patients
The dataset used here was obtained from a longitudinal, prospective, interventional study with the goal of analyzing the performance of an exercise-challenged closed-loop controller in T1D people [16]. A total of six participants were enrolled at the Clinic University Hospital of Barcelona. The protocol was approved by the Ethics Committee of the hospital. Criteria for eligibility were: (1) age between 18 and 60 years old, (2) Body Mass Index (BMI) between 18 and 30 kg/m, (3) Glycated Hemoglobin A1c (HbA1C) between 6.0% and 8.5%, and (4) use of Continuous Subcutaneous Insulin Infusion (CSII) for at least six months. Exclusion criteria included: (1) pregnancy, (2) use of experimental drug or devices in the past 30 days, (3) onset of progressive fatal diseases, (4) hypoglycemia unawareness, (5) drug or alcohol abuse, and (6) other systematic diseases other than T1D, including hepatic, neurological, and endocrine-related illnesses. A summary of the patient demographics is shown in Table 1.
Each participant underwent three aerobic and three anaerobic exercise tests. The order of the type of exercise was randomized, but the same type was carried out for three consecutive trials. The subjects used Paradigm Veo® insulin pumps, and two Enlite-2® (Medtronic Minimed, Northridge, CA, USA) CGM sensors were inserted in different parts of the abdomen the day before the trial by the subjects. Plasma glucose (PG) as a reference value was measured using the YSI 2300 Stat Plus Glucose Analyzer (YSI Incorporated Life Sciences, Yellow Springs, OH, USA), with a frequency of 15 min. The exercise schedules were as follows:
- Aerobic routine: Patients exercised doing three bouts of 15 min on a cycloergometer at 60% of the patients maximum capacity with five minutes of rest between them.
- Anaerobic (resistance) routine: Patients exercised doing five bouts of eight repetitions of four different exercise sets of 15 min at 70% of the patients’ maximum capacity with 90 s of rest between sets.
The exercise intensity was converted into units of heart rate, which was different for each patient and calculated as follows:
where is the intensity of the exercise in terms of heart rate for patient i, stands for the percentage intensity of the exercise (60 for aerobic exercise, 70 for anaerobic), and stands for the maximum heart rate of patient i, defined as for women, and for men, where is the age of patient i in years. Lastly, is the resting heart rate of patient i as measured at the beginning of the experiment.
2.2. Exercise Monitoring Devices
Off-the-shelf physical activity monitors were used to obtain the different biometric variables registered in the study. Patients wore three different devices simultaneously:
- Fitbit Charge HR™(Fitbit, San Francisco, CA, USA): a physical activity monitor that tracks several exercise signals: (1) heart rate, (2) steps, (3) floor level, (4) Metabolic equivalents (METs), and (5) calories burned.
- Microsoft® Band 2 (Microsoft, Redmond, WA, USA): a multipurpose device that tracks physiological variables such as: (1) heart rate, (2) steps, (3) galvanic skin response, (4) skin temperature and (5) movements.
- Polar heart rate monitor, Model RCX3® (Polar, Kempele, Finland): a commercially-established heart rate monitor.
The above listed variables were recorded with a sample rate of one minute and downloaded at the end of each trial. Each device provided a different number of signals, which will be listed next, for a total of 11 signals. The nomenclature of each signal needs to be defined in advance, since they will be referred to using this notation from here on. For each signal, a three-letter code was defined representative of the nature of that signal. The first letter of the triplet was the initial letter of the device that provided that signal, and the second and third letters were an abbreviation of the name of the signal itself. For example, the signal named FHR stands for F from the Fitbit Device and HR from the Heart Rate signal.
- FHR: Fitbit Heart Rate; measured in beats per minute; can be used to estimate exercise intensity.
- FST: Fitbit STeps; the number of steps walked.
- FLV: Fitbit LeVel; the number of floors of stairs climbed.
- FME: Fitbit MEts; the metabolic equivalent of tasks; an estimation of exercise intensity normalized for each patient.
- FCA: Fitbit CAlories; calories burned.
- MHR: Microsoft Band Heart Rate.
- MTM: Microsoft Band TeMperature; skin temperature.
- MGS: Microsoft Band Galvanic Skin Response; an estimation of the skin electrodermal activity, also known as the conductance level of the skin.
- MST: Microsoft Band STeps; number of steps walked.
- MMO: Microsoft Band MOvements; accumulated movement magnitude registered by the accelerometer.
- PHR: Polar Heart Rate.
2.3. Data Filtering and Pre-Processing
Thirty six trials were completed, and data were collected for all of them. In order to align CGM and YSI data, CGM data were linearly interpolated and rounded to one sample per minute. Following the rationale described in [7], data arrays corresponding to either CGM or YSI malfunction, error outliers, or more than 30% of data samples flagged as faulty were discarded. A total of 665 sampled pairs were available, distributed among 27 streams of data out of the 36 corresponding to paired errors of CGM vs. YSI following the rule:
where represents the CGM estimation error for data stream i at timestamp k. Similarly, and are the CGM data and plasma glucose data measured with the YSI. Each data stream i is a time series corresponding to a particular experiment and CGM signal.
CGM accuracy was evaluated using the Mean Absolute Relative Deviation (MARD), calculated as:
where is the average percent error of the data stream i and n is the total number of samples available for i.
Wearable data were pre-processed by removing the baseline value of each wearable signal and trial from the signal itself. The baseline of each signal was calculated as the median value of that particular variable for each data stream evaluated only in the resting period. In an out-of-clinic environment, this value is trivial to obtain since it would be the equilibrium value of the signal during resting or sleeping periods.
The availability of the different wearable variables, defined as the complementary value of the percentage of missing samples, varied from signal to signal. In Table 2, the availability of each one of the signals obtained from the wearables is provided.
2.4. Data Analysis
2.4.1. Model Fit
Linear regression models were used to fit the CGM error data, using only the wearable signals as inputs. The intercept of the model was forced to be zero in order to better compensate only the error observed in the exercise period. The linear regression model follows the following equation:
where is the vector of regression parameters, of a length equal to the number of wearable signals used. Each of the components of , corresponding to each of the wearable signals, is a column vector of length n. Finally, the new enhanced CGM (eCGM) estimations, corrected using the new estimated error, is calculated as follows:
where represents the enhanced CMG values for data stream i, are the original sensor glucose estimations, and are the output of the linear regression above.
2.4.2. Exercise Signal Selection
In order to determine which of the wearable signals in the study were more relevant for our purposes, a backwards elimination of variables approach was followed, in which variables were sequentially discarded as inputs to the correction model, based on:
- Lack of availability of synchronous data to the CGM-YSI available pairs.
- Lack of representation of the type of physical activity performed in the study: cycloergometer aerobic exercise.
- High correlation between wearable signals. A high correlation between two signals implies that the amount of information carried by each one of those signals is similar; thus, one of them can be eliminated without hindering the predictive capabilities of the model.
- MARD improvement evaluated in the validation sets (see Section 2.4.3 below). A wearable was removed from the input set if the MARD for the validation sets (both in the exercise period and in global terms) was improved by removing that wearable signal alone.
If a variable complied with the above rules, it was removed from the inputs of the multiple regression model, and the model was fit again to the data and the outputs re-evaluated, until no improvement of the error was achieved by removing any of the inputs.
2.4.3. Cross-Validation
The predictive power of the model was validated by performing a non-exhaustive leave nine-out cross-validation of the model. Out of the set of 27 streams of data, two thirds (i.e., 18 randomly-chosen streams out of 27) were selected as a fitting set, and the remaining data were used to validate the fitted model. Model accuracy was evaluated on the validation set, the results stored, and the process was repeated, randomly selecting new fitting and validation sets. This process was repeated 20 times. All the accuracy metrics shown onward were those averaging the results throughout all the 20 validation sets of nine streams of data.
3. Results
3.1. Wearable Selection
Any wearable with 30% or more samples not usable to fit the model, such as missing samples, disconnections, or out of bounds samples, was discarded from the fit. Following the backwards elimination philosophy previously detailed, the first two wearable signals discarded from the model fit were MST and PHR due to their low availability in Table 2, leaving the remaining matrix to fit the model:
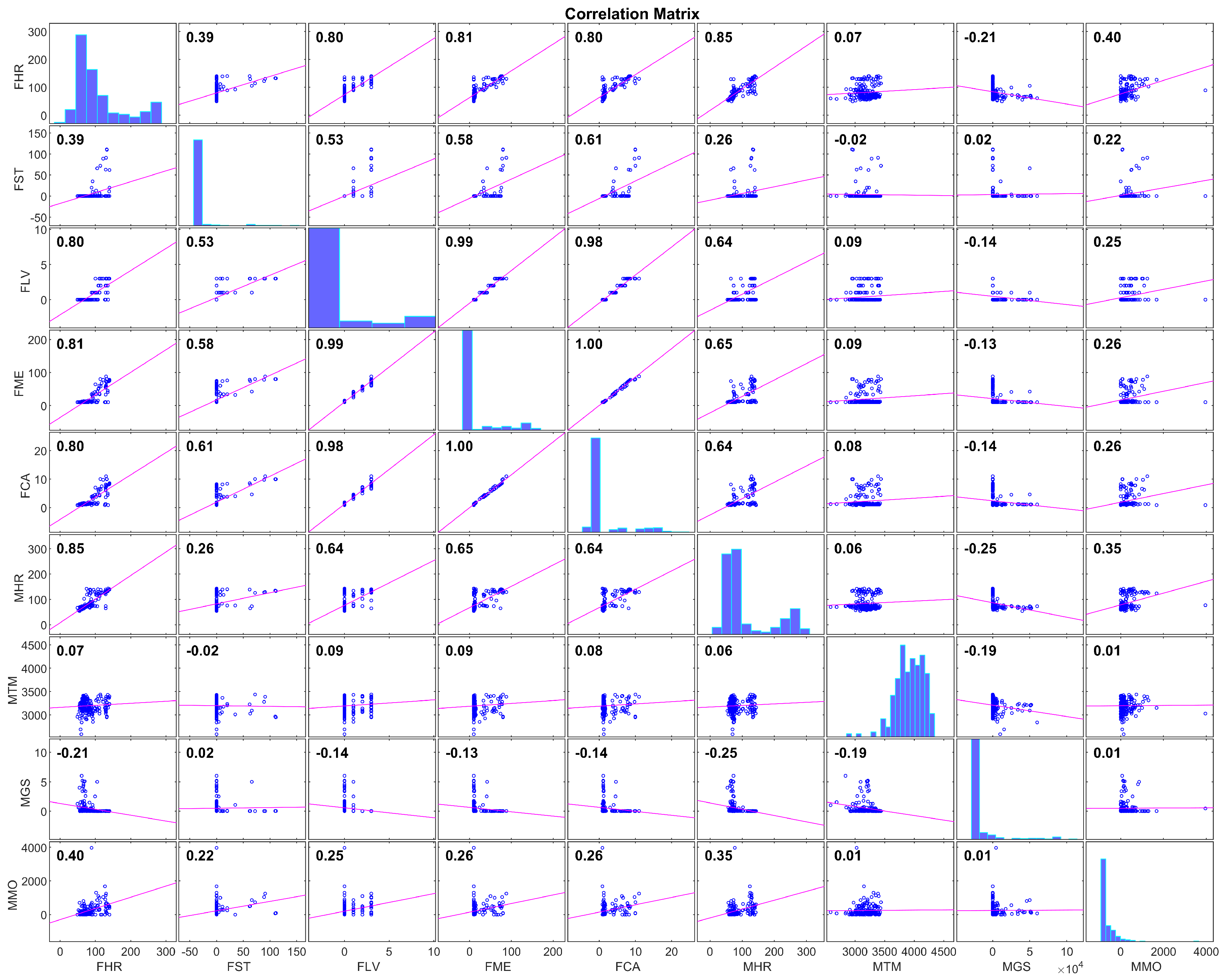
Next, the correlation between the remaining signals was computed, with the results in Figure 1.
The correlations between FLV, FME, and FCA (all derived from the accelerometer sensor) showed that those three variables carried essentially the same information. FME was deemed a more relevant variable than the other two due to its continuous nature (FLV is discrete by definition) and the fact that it was normalized by the baseline energy consumption of each patient, which suggests that a linear model using this variable as an input would require less individualization than one using the other variables. Thus, it was decided to discard FLV and FCA from the model fit.
Similarly, both FHR and MHR were highly correlated (), which is coherent with the nature of those variables, since both of them estimated the same physiological value. It was decided that FHR was more relevant than MHR for the linear model due to its higher availability, as shown in Table 2. Thus, MHR was discarded as an input to the model.
Finally, FST was deemed irrelevant for the type of exercise performed in the trials. FST estimates the intensity of physical activity and quantifies that value in the number of steps walked by the patient. The physical activity from this study (cycloergometer) rendered the patient static for most of the exercising period, which would result in inaccurate estimations of the steps. Furthermore, the histogram of the signal FST in Figure 1 shows that most of the FST values laid very close to zero. Removing FST from the inputs list left the input parameter array as:
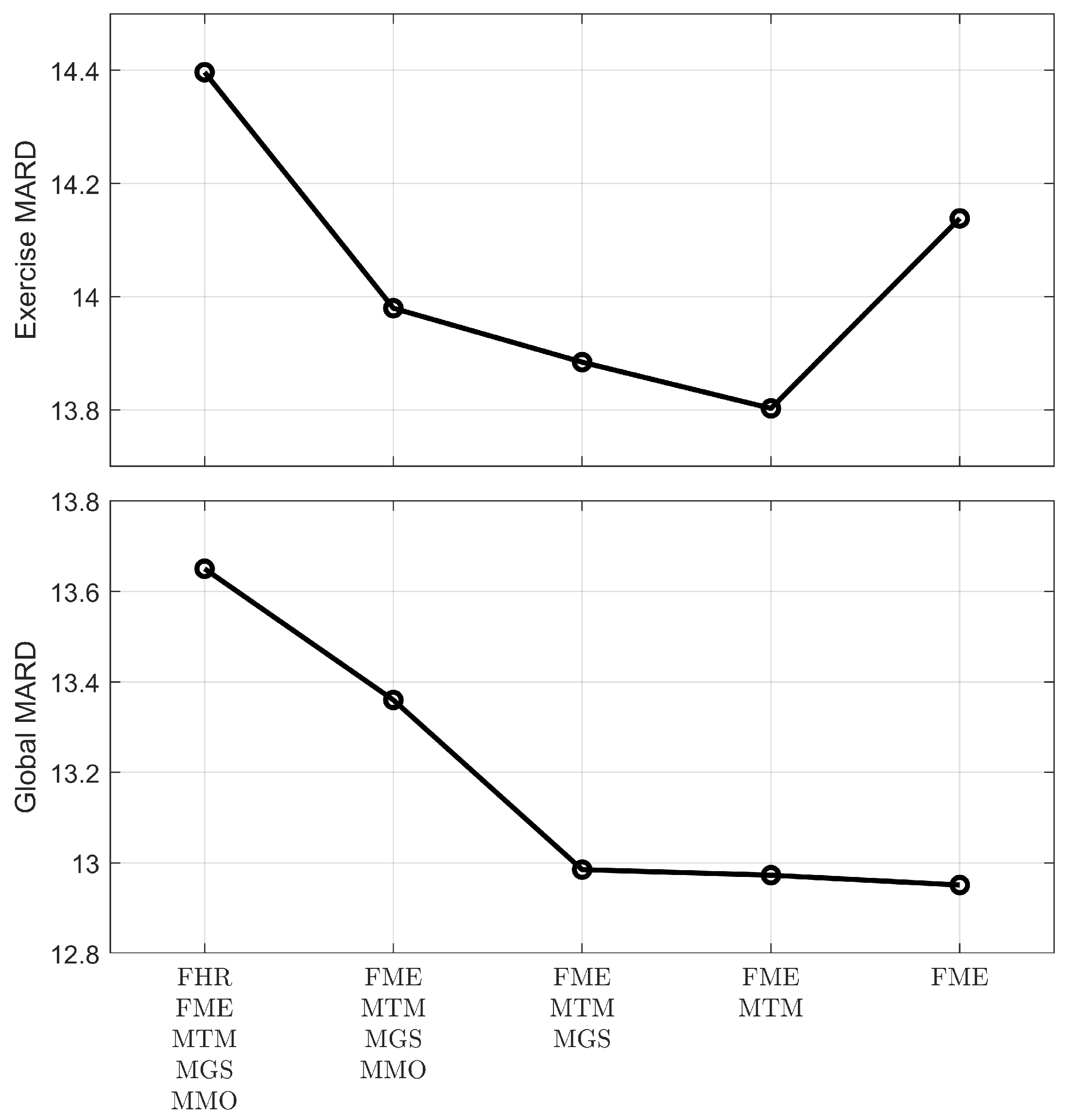
Using the five remaining signals as inputs, the linear model was fit, and the results of the MARD improvement in the validation sets were recorded. A single input was removed one at a time, the model’s performance recorded, and the cycle repeated, removing another input and using the others. The input elimination that further worsened the MARD in the exercise period, or the one that most worsened the MARD for the whole trial period in case of equal exercise MARD values, was permanently eliminated. The sequence of eliminations and the results on the MARD reduction are shown in Figure 2.
The model improved plasma glucose estimations as inputs were removed from the system, especially when looking at the whole period of monitoring (global MARD). However, the global MARD reduction from removing the two last signals, MTM and MGS, was minimal. MARD in the exercise period was also reduced by removing the same signals except when removing MTM. Thus, the final selected list of inputs for the model is:
3.2. Error Grid Analysis and Model Performance
The final order of the model was two, since only two signals were used as the input. The average values of coefficients for the model fit are shown in Table 3, along with the parameters of the model, fitting all available data and not separating any for validations.
MARD results for the proposed model are shown in Table 4, along with the Coefficient of Variation (CV; defined as CV , where stands for the standard deviation and stands for the mean value) to evaluate glycemic variability.
MARD during the exercise period was reduced drastically and significantly, from 17.46% to 13.8%, which was much closer to the average MARD of the original CGM of 13.61%. The total MARD (CGM error in the whole dataset, not separating resting and exercise periods) was reduced slightly to 12.97%, and the error during the resting period was increased marginally to 12.88%, but both figures were not significantly different than those presented by the original CGM.
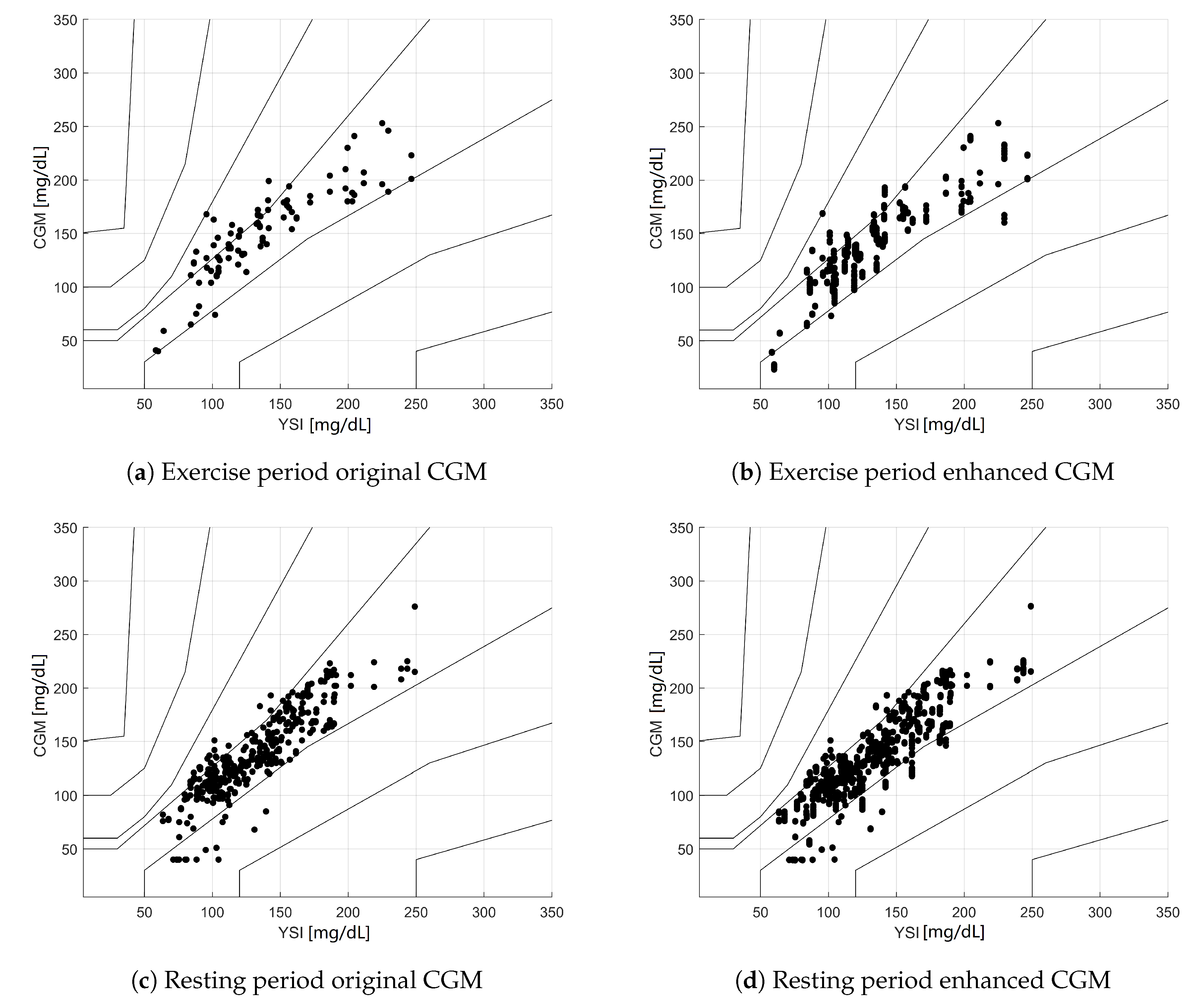
The validation data were evaluated using different acceptability criteria. The Clarke error grid analysis of the data [17] is depicted in Figure 3. Note that since 20 iterations of the fit-validate cycle were performed, there were several data points corresponding to the same PG value, displaying vertical patterns in the eCGM subplots. This also means that the point density of the eCGM subplots was much higher than those of the original CGM.
The numeric values of the results for the Clarke EGA can be seen in Table 5. The results showed a displacement towards the A zone, especially during exercise, as a response to the proposed correction.
In addition to the Clarke EGA analysis, Figure 4 shows the results of the Parkes EGA [18], which classifies the same pairs of data into different zones, with the advantage of showing more continuous transitions between adjacent zones in the PG-CGM plane. Table 6 shows the numeric results for the same EGA analysis.
4. Discussion
The first outcome that can be extracted from the results is that further integration of physiological signals in CGM devices is desired. CGM devices use algorithmic rules to fit the chemical measurements of the subcutaneous probe into relatively accurate plasma glucose values. If the data extracted from wearable devices were to be integrated in those algorithms, glucose estimation would benefit greatly.
The proposed linear regression model (composed of only two parameters) achieved a reduction in the MARD during aerobic exercise that practically nullified the influence of the exercise on the CGM estimation error. Indeed, the MARD was significantly reduced from 17.46% to 13.8%, much closer to the global average MARD value for the original CGM readings of 13.61%. This achievement was the main reason to choose a regression model for error compensation, which validated the starting hypothesis.
The regression model presented here differed from other studies involving wearables in the AP (see [11,12]) in the fact that the work presented here supposed a more general result, its application being not only limited to closed loop studies; the work presented here can be used to provide better estimations to an AP device, but it is not limited to that. It can also be used to provide simply more accurate continuous glucose readings to people with diabetes regardless of whether or not they are using an AP device or undergoing CSII treatment.
The Clarke EGA shown in Figure 3 indicated very encouraging results for the exercise period; while the original CGM already had 100% of the samples in the A + B zone, eCGM showed a shift of the data points towards the A zone for the exercise period (72.4% → 85.7%). However, Clarke’s analysis also showed a very small rise of points in Zone D during the rest period (0.2% → 0.6%), while no points were present in Zone C. This is a consequence of the discontinuity in the zones defined for Clarke’s EGA, where Zone D can be accessed directly from Zone A or B. This is one of the main criticisms [18] against Clarke’s EGA, and it was the reason that motivated the comparison with other analysis methodologies.
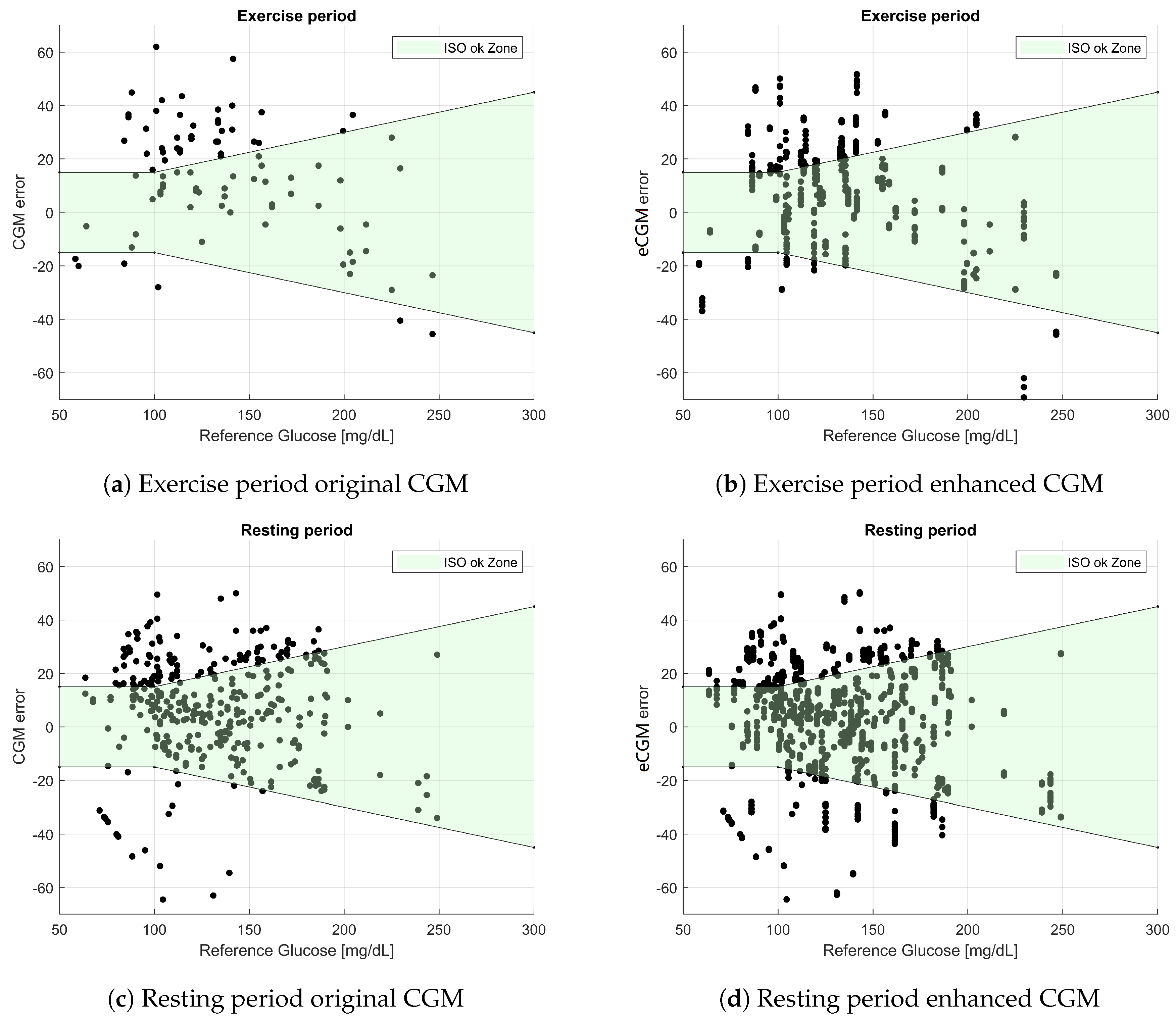
The results shown in Table 6 are even more positive, showing an increase of points in Zone A (79.2% → 89.2%), while showing no points in Zones C + D + E. ISO results from Table 7 also showed better results for eCGM than the original sensor, increasing the amount of “OK” samples 55.2% → 64.4% during the exercise period, as well as increasing the total samples in the ISO zone 66.6% → 68.8%
Figure 2 compares MARD between different proposed models of decreasing complexity, showing also increasing performance in the validation error. The difference in the global MARD values in the last two models was almost non-existent, while the MARD during the exercise phase of the study actually worsened. However, these differences were very small when compared to the MARD reduction achieved by utilizing any of those models versus not using any model to compensate for exercise (17.46% → 13.8% and 17.46% → 14.14%). It can be argued that using a model with only one parameter is preferable than the more complex option of a two-parameter model, especially when looking at the fact that both input signals came from different devices on the market: FME was provided by the Fitbit device, and MTM was extracted from the Microsoft device.
This work did not focus on the nature of the signals used in the model. Rather, the focus here was on the user-level data that can be easily extracted from a device, which translates into a more straightforward implementation of the model in portable devices. This implies that some of the signals that were estimated from each of the devices using hidden algorithms might not be reproducible from other raw data, e.g., FME was an energy expenditure estimation by the Fitbit device calculated from its sensors, which can differ from implementations in other devices. In a recent study comparing different research and consumer devices, an error range of 10% was found for heart rate and energy expenditure measurements [20].
It must be noted that the current approach has some drawbacks due to its intentional simplicity. First, while the CGM error was reduced significantly in the exercise period, this was achieved by means of a direct algebraic link to the signals of the wearable devices, which may transport noise from the wearable into the CGM, but that problem was not observed in our data. Additionally, it must be mentioned that more complex dynamic models might have further enhanced CGM accuracy, but the design of such models is beyond the scope of this work.
5. Conclusions
This paper showed that continuous glucose estimation can benefit from the integration of signals readily available from wearables. CGM estimation error was improved during the exercise period and was not significantly increased otherwise. The model proposed was composed of two parameters; however, a simpler model composed of only one parameter can also yield acceptable results, and the technology is readily available with off-the-self devices.
Author Contributions
Conceptualization, A.J.L.S. and J.B.; methodology, A.J.L.S., J.L.D. and J.B.; software, A.J.L.S.; validation, A.J.L.S., J.L.D. and J.B.; formal analysis, A.J.L.S.; investigation, A.J.L.S., J.L.D., M.G. and J.B.; resources, M.G. and J.B.; data curation, A.J.L.S., J.L.D. and M.G.; writing, original draft preparation, A.J.L.S.; writing, review and editing, A.J.L.S., J.L.D., M.G. and J.B.; visualization, A.J.L.S.; supervision, A.J.L.S. and J.B.; project administration, J.B.; funding acquisition, A.J.L.S., J.L.D., M.G. and J.B.
Funding
This work was supported by the Spanish Ministry of Economy, Industry and Competitiveness (MINECO) (Grant Number DPI2016-78831-C2-1-R), the European Union (FEDER funds), and the Vicerectorate of Research, Innovation and Technology Transference from the Universitat Politècnica de València (Grant Number PAID-06-18).
Acknowledgments
We would like to acknowledge the work performed by Josep Vehí, Lyvia Biagi, Ignacio Conget and Carmen Quirós. We thank all the participants and clinical staff who participated in clinical acquisition and pre-formatting of data for study, without whom none of this work would have been possible.
Conflicts of Interest
The authors declare no conflict of interest.
Ethical Statements
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the Clinic University Hospital of Barcelona (Project Code DPI2016-78831-C2-1-R).
Abbreviations
The following abbreviations are used in this manuscript:
| MARD | Median Absolute Relative Deviation |
| PG | Plasma Glucose |
| CGM | Continuous Glucose Monitor |
| eCGM | Enhanced Continuous Glucose Monitor |
| AP | Artificial Pancreas |
| T1D | Type 1 Diabetes |
| BMI | Body Mass Index |
| HBA1c | Glycated Hemoglobin (A1c) |
| CSII | Continuous Subcutaneous Insulin Infusion |
| CV | Coefficient of Variation |
| EGA | Error Grid Analysis |
References
- International Diabetes Federation. IDF Diabetes Atlas, 8th ed.; International Diabetes Federation: Brussels, Belgium, 2017. [Google Scholar]
- Bergenstal, R.M.; Garg, S.; Weinzimer, S.A.; Buckingham, B.A.; Bode, B.W.; Tamborlane, W.V.; Kaufman, F.R. Safety of a Hybrid Closed-Loop Insulin Delivery System in Patients with Type 1 Diabetes. JAMA 2016, 316, 1407. [Google Scholar] [CrossRef] [PubMed]
- Zecchin, C.; Facchinetti, A.; Sparacino, G.; Dalla Man, C.; Manohar, C.; Levine, J.A.; Basu, A.; Kudva, Y.C.; Cobelli, C. Physical Activity Measured by Physical Activity Monitoring System Correlates with Glucose Trends Reconstructed from Continuous Glucose Monitoring. Diabetes Technol. Ther. 2013, 15, 836–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manohar, C.; Levine, J.A.; Nandy, D.K.; Saad, A.; Dalla Man, C.; McCrady-Spitzer, S.K.; Basu, R.; Cobelli, C.; Carter, R.E.; Basu, A.; et al. The Effect of Walking on Postprandial Glycemic Excursion in Patients with Type 1 Diabetes and Healthy People. Diabetes Care 2012, 35, 2493–2499. [Google Scholar] [CrossRef] [PubMed]
- Taleb, N.; Emami, A.; Suppere, C.; Messier, V.; Legault, L.; Chiasson, J.L.; Rabasa-Lhoret, R.; Haidar, A. Comparison of Two Continuous Glucose Monitoring Systems, Dexcom G4 Platinum and Medtronic Paradigm Veo Enlite System, at Rest and During Exercise. Diabetes Technol. Ther. 2016, 18, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Zaharieva, D.P.; Turksoy, K.; McGaugh, S.M.; Pooni, R.; Vienneau, T.; Ly, T.T.; Riddell, M.C. Lag Time Remains with Newer Real-Time Continuous Glucose Monitoring Technology During Aerobic Exercise in Adults Living with Type 1 Diabetes. Diabetes Technol. Ther. 2019, 21. [Google Scholar] [CrossRef] [PubMed]
- Biagi, L.; Bertachi, A.; Quirós, C.; Giménez, M.; Conget, I.; Bondia, J.; Vehí, J. Accuracy of continuous glucose monitoring before, during, and after aerobic and anaerobic exercise in patients with type 1 diabetes mellitus. Biosensors 2018, 8, 22. [Google Scholar] [CrossRef] [PubMed]
- Giani, E.; Macedoni, M.; Barilli, A.; Petitti, A.; Mameli, C.; Bosetti, A.; Cristiano, A.; Radovanovic, D.; Santus, P.; Zuccotti, G.V. Performance of the Flash Glucose Monitoring System during exercise in youth with Type 1 diabetes. Diabetes Res. Clin. Pract. 2018, 146, 321–329. [Google Scholar] [CrossRef] [PubMed]
- De Arriba-Pérez, F.; Caeiro-Rodríguez, M.; Santos-Gago, J.M. Collection and processing of data from wrist wearable devices in heterogeneous and multiple-user scenarios. Sensors 2016, 16, 1538. [Google Scholar] [CrossRef] [PubMed]
- Ding, S.; Schumacher, M. Sensor Monitoring of Physical Activity to Improve Glucose Management in Diabetic Patients: A Review. Sensors 2016, 16, 589. [Google Scholar] [CrossRef] [PubMed]
- Breton, M.D.; Brown, S.A.; Karvetski, C.H.; Kollar, L.; Topchyan, K.A.; Anderson, S.M.; Kovatchev, B.P. Adding Heart Rate Signal to a Control-to-Range Artificial Pancreas System Improves the Protection Against Hypoglycemia During Exercise in Type 1 Diabetes. Diabetes Technol. Ther. 2014, 16, 506–511. [Google Scholar] [CrossRef] [PubMed]
- Turksoy, K.; Quinn, L.T.; Littlejohn, E.; Cinar, A. An Integrated Multivariable Artificial Pancreas Control System. J. Diabetes Sci. Technol. 2014, 8, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Turksoy, K.; Paulino, T.M.L.; Zaharieva, D.P.; Yavelberg, L.; Jamnik, V.; Riddell, M.C.; Cinar, A. Classification of Physical Activity: Information to Artificial Pancreas Control Systems in Real Time. J. Diabetes Sci. Technol. 2015, 9, 1200–1207. [Google Scholar] [CrossRef] [PubMed]
- Stenerson, M.; Cameron, F.; Wilson, D.M.; Harris, B.; Payne, S.; Bequette, B.W.; Buckingham, B.A. The Impact of Accelerometer and Heart Rate Data on Hypoglycemia Mitigation in Type 1 Diabetes. J. Diabetes Sci. Technol. 2014, 8, 64–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turksoy, K.; Monforti, C.; Park, M.; Griffith, G.; Quinn, L.; Cinar, A.; Turksoy, K.; Monforti, C.; Park, M.; Griffith, G.; et al. Use of Wearable Sensors and Biometric Variables in an Artificial Pancreas System. Sensors 2017, 17, 532. [Google Scholar] [CrossRef] [PubMed]
- Quirós, C.; Bertachi, A.; Giménez, M.; Biagi, L.; Viaplana, J.; Viñals, C.; Vehí, J.; Conget, I.; Bondia, J. Control de la glucemia durante el ejercicio físico aeróbico y anaeróbico mediante un nuevo sistema de páncreas artificial. Endocrinol. Diabetes Y Nutr. 2018, 65, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Clarke, W.L.; Cox, D.J.; Gonder-Frederick, L.A.; Carter, W.; Pohl, S.L. Evaluating clinical accuracy of systems for self-monitoring of blood glucose. Diabetes Care 1987, 10, 622–628. [Google Scholar] [CrossRef] [PubMed]
- Parkes, J.L.; Slatin, S.L.; Pardo, S.; Ginsberg, B.H. A new consensus error grid to evaluate the clinical significance of inaccuracies in the measurement of blood glucose. Diabetes Care 2000, 23, 1143–1148. [Google Scholar] [CrossRef] [PubMed]
- Jendrike, N.; Baumstark, A.; Kamecke, U.; Haug, C.; Freckmann, G. ISO 15197: 2013 Evaluation of a Blood Glucose Monitoring System’s Measurement Accuracy. J. Diabetes Sci. Technol. 2017, 11, 1275. [Google Scholar] [CrossRef] [PubMed]
- Yavelberg, L.; Zaharieva, D.; Cinar, A.; Riddell, M.C.; Jamnik, V. A Pilot Study Validating Select Research-Grade and Consumer-Based Wearables Throughout a Range of Dynamic Exercise Intensities in Persons with and without Type 1 Diabetes: A Novel Approach. J. Diabetes Sci. Technol. 2018, 12, 569–576. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Correlation matrix of the wearable signals from the subset of valid variables selected. Note that the quantization of some of the variables renders point density in some of the subfigures very different from others. For example, most of FST values are located around zero, which makes linear regression plots look like the line does not fit the data, but this is not the case.
Figure 1.
Correlation matrix of the wearable signals from the subset of valid variables selected. Note that the quantization of some of the variables renders point density in some of the subfigures very different from others. For example, most of FST values are located around zero, which makes linear regression plots look like the line does not fit the data, but this is not the case.

Figure 2.
Sequence of MARD values for the exercise period (top panel) and for the whole trial (bottom panel), as each signal was removed from the model.
Figure 2.
Sequence of MARD values for the exercise period (top panel) and for the whole trial (bottom panel), as each signal was removed from the model.

Figure 3.
Clarke error grid analysis for the wearable-enhanced CGM data. (a) Subset of CGM-PG pairs before enhancement during the physical activity period. (b) Subset of CGM-PG pairs after enhancement with exercise monitoring devices during the physical activity period. (c) Subset of CGM-PG pairs before enhancement during the resting period. (d) Subset of CGM-PG pairs after enhancement with exercise monitoring devices during the resting period.
Figure 3.
Clarke error grid analysis for the wearable-enhanced CGM data. (a) Subset of CGM-PG pairs before enhancement during the physical activity period. (b) Subset of CGM-PG pairs after enhancement with exercise monitoring devices during the physical activity period. (c) Subset of CGM-PG pairs before enhancement during the resting period. (d) Subset of CGM-PG pairs after enhancement with exercise monitoring devices during the resting period.

Figure 4.
Figure 4. Parkes error grid analysis for the wearable-enhanced CGM estimations. (a) Subset of CGM-YSI pairs before enhancement during the physical activity period. (b) Subset of CGM-YSI pairs after enhancement with exercise monitoring devices during the physical activity period. (c) Subset of CGM-YSI pairs before enhancement during the resting period. (d) Subset of CGM-YSI pairs after enhancement with exercise monitoring devices during the resting period.
Figure 4.
Figure 4. Parkes error grid analysis for the wearable-enhanced CGM estimations. (a) Subset of CGM-YSI pairs before enhancement during the physical activity period. (b) Subset of CGM-YSI pairs after enhancement with exercise monitoring devices during the physical activity period. (c) Subset of CGM-YSI pairs before enhancement during the resting period. (d) Subset of CGM-YSI pairs after enhancement with exercise monitoring devices during the resting period.

Figure 5.
ISO acceptable region for the wearable-enhanced CGM errors. (a) Subset of error-YSI pairs before enhancement during the physical activity period. (b) Subset of error-YSI pairs after enhancement with exercise monitoring devices during the physical activity period. (c) Subset of error-YSI pairs before enhancement during the resting period. (d) Subset of error-YSI pairs after enhancement with exercise monitoring devices during the resting period.
Figure 5.
ISO acceptable region for the wearable-enhanced CGM errors. (a) Subset of error-YSI pairs before enhancement during the physical activity period. (b) Subset of error-YSI pairs after enhancement with exercise monitoring devices during the physical activity period. (c) Subset of error-YSI pairs before enhancement during the resting period. (d) Subset of error-YSI pairs after enhancement with exercise monitoring devices during the resting period.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Participants’ characteristics. Data expressed as the mean ± standard deviation.
| Number of Patients (Females) | 6 (1) |
|---|---|
| Age (years) | |
| HbA1c (%) | |
| BMI (kg/m) | |
| Time with T1D (years) | |
| Time with CSII (years) |
Table 2.
Wearable signals’ availability. FHR: Fitbit Heart Rate; FST: Fitbit STeps; FLV: Fitbit LeVel; FME: Fitbit MEts; FCA: Fitbit CAlories; MHR: Microsoft Band Heart Rate; MTM: Microsoft Band TeMperature; MGS: Microsoft Band Galvanic Skin Response; MST: Microsoft Band STeps; MMO: Microsoft Band MOvements; PHR: Polar Heart Rate.
Table 2.
Wearable signals’ availability. FHR: Fitbit Heart Rate; FST: Fitbit STeps; FLV: Fitbit LeVel; FME: Fitbit MEts; FCA: Fitbit CAlories; MHR: Microsoft Band Heart Rate; MTM: Microsoft Band TeMperature; MGS: Microsoft Band Galvanic Skin Response; MST: Microsoft Band STeps; MMO: Microsoft Band MOvements; PHR: Polar Heart Rate.
| FHR | FST | FLV | FME | FCA | MHR | MTM | MGS | MST | MMO | PHR | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Availability (%) | 96.4 | 100 | 100 | 100 | 100 | 78.7 | 73.3 | 78.7 | 14.7 | 73.3 | 55.3 |
Table 3.
Proposed model parameters. stands for the FME signal coefficient in and the coefficient for the MTM signal in .
Table 3.
Proposed model parameters. stands for the FME signal coefficient in and the coefficient for the MTM signal in .
| Parameter | ||
|---|---|---|
| Average parameter in cross-validation | 0.33 | −0.0017 |
| Parameter fitting all data | 0.297 | −0.0053 |
Table 4.
MARD and CV results for the selected model.
| Original CGM | Enhanced CGM | p-Value | ||
|---|---|---|---|---|
| MARD | Exercise period | 17.46% | 13.8% | <0.05 |
| Resting Period | 12.75% | 12.88% | 0.75 | |
| Total | 13.61 % | 12.97 % | 0.4 | |
| CV | 17% | 16% | 0.17 | |
Table 5.
Table of the results for the classification of the CGM samples in the different Clarke EGA zones. CGM-PG refers to paired CGM and PG data.
Table 5.
Table of the results for the classification of the CGM samples in the different Clarke EGA zones. CGM-PG refers to paired CGM and PG data.
| Zone | A | B | C | D | E | ||
|---|---|---|---|---|---|---|---|
| CGM-PG pair allocation (%) | Exercise Period | CGM | 72.4 | 27.6 | 0 | 0 | 0 |
| eCGM | 85.7 | 14.3 | 0 | 0 | 0 | ||
| Resting Period | CGM | 85.6 | 14.2 | 0 | 0.2 | 0 | |
| eCGM | 84.3 | 15.1 | 0 | 0.6 | 0 | ||
| Total | CGM | 82.6 | 17.2 | 0 | 0.2 | 0 | |
| eCGM | 84.6 | 15 | 0 | 0.4 | 0 | ||
Table 6.
Table of results for the classification of the CGM samples in the different Parkes EGA zones.
Table 6.
Table of results for the classification of the CGM samples in the different Parkes EGA zones.
| Zone | A | B | C | D | E | ||
|---|---|---|---|---|---|---|---|
| CGM-PG pair allocation (%) | Exercise Period | CGM | 79.2 | 20.8 | 0 | 0 | 0 |
| eCGM | 89.2 | 10.8 | 0 | 0 | 0 | ||
| Resting Period | CGM | 90.5 | 9.5 | 0 | 0 | 0 | |
| eCGM | 87.7 | 12.3 | 0 | 0 | 0 | ||
| Total | CGM | 88 | 12 | 0 | 0 | 0 | |
| eCGM | 88 | 12 | 0 | 0 | 0 | ||
Table 7.
Table of the results for the classification of the CGM samples within the bounds as defined in ISO 15197: 2013.
Table 7.
Table of the results for the classification of the CGM samples within the bounds as defined in ISO 15197: 2013.
| ISO Valid Samples | ||
|---|---|---|
| Original CGM | Enhanced CGM | |
| Exercise Period | 55.23 % | 64.4% |
| Resting Period | 69.9% | 70.1% |
| Total | 66.6% | 68.8% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Laguna Sanz, A.J.; Díez, J.L.; Giménez, M.; Bondia, J. Enhanced Accuracy of Continuous Glucose Monitoring during Exercise through Physical Activity Tracking Integration. Sensors 2019, 19, 3757. https://doi.org/10.3390/s19173757
AMA Style
Laguna Sanz AJ, Díez JL, Giménez M, Bondia J. Enhanced Accuracy of Continuous Glucose Monitoring during Exercise through Physical Activity Tracking Integration. Sensors. 2019; 19(17):3757. https://doi.org/10.3390/s19173757
Chicago/Turabian StyleLaguna Sanz, Alejandro José, José Luis Díez, Marga Giménez, and Jorge Bondia. 2019. "Enhanced Accuracy of Continuous Glucose Monitoring during Exercise through Physical Activity Tracking Integration" Sensors 19, no. 17: 3757. https://doi.org/10.3390/s19173757
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.