1.1. Clinical Background and State-of-the-Art
Of all worldwide deaths, 31.3% were caused by cardiovascular diseases (CVD) in 2016, making them the most common cause of death. Amongst the noncommunicable diseases, respiratory issues are the third leading cause of death worldwide with 6.7% [
1]. It is now a well-known fact, however, that respiration-related illnesses can also significantly increase the risk for CVD and other diseases. Especially in the case of obstructive sleep apnea (OSA), close relations to increased CVD such as hypertension [
2] and atrial fibrillation [
3] have been reported. At the same time, OSA is one of the most common sleep disorders with an estimated 936 million people affected worldwide [
4]. Respiratory parameters also play an important role in the clinical, postanesthetic routine. It has been shown that respiratory complications are major causes of prolonged hospital stay, poor overall outcomes, and increased mortality [
5,
6,
7]. Outbreaks of respiratory syndromes such as severe acute respiratory syndrome (SARS), Middle East respiratory syndrome (MERS), and the currently ongoing COVID-19 pandemic [
8] further emphasize the importance of tools for an early diagnosis [
9]. From the described situation, it becomes evident that cardiorespiratory monitoring is one of the major fields to be addressed in the future.
During the last two decades, rapid developments in battery technology, low-power embedded processors, and integrated sensors have led to technologies being increasingly wearable. Current generations of wearable, noninvasive biosignal acquisition systems can be roughly categorized by their runtime and the physiological parameters of interest [
10], as well as their implementation, biosignal selection, and whether or not they are organized into networks [
11]. The physiological parameters addressed are oriented on the identified large health issues of the present and future. It is therefore consequent that a large number of systems focus on the cardiovascular system, activity measures, the respiratory system, and the metabolism. The selection of biosignals varies with the use-case and implementation. Commonly found modalities are the ECG, accelerometry, gyrometry, photoplethysmography, galvanic skin response, body temperature, bioimpedance methods, blood glucose, and ambient parameters. Systems can be designed to operate on their own or in networks such as body area networks, body sensor networks, or wireless sensor networks. Due to a variety of materials available ranging from standard printed circuit boards (PCB) and flexible PCBs to textile integrated electronics [
12], implementations of wearable biosignal acquisition systems usually range from sensor shirts over chest straps, wrist-bands, and necklaces, to small adhesive patches implemented using flexible materials [
13].
The electrocardiogram (ECG) is widely considered as a gold standard for the non-invasive assessment of the cardiovascular system and detection of CVD. The resting ECG is an effective screening method for athletes [
14] and a tool for cardiovascular risk assessment in asymptomatic adults [
15]. In a chest pain emergency situation, obtaining an ECG within 10 min is recommended [
16]. Transient symptoms such as arrhythmias are monitored using 24 h Holter ECG systems or over days or weeks using long-term systems, especially preceding and following ablation therapy [
17]. Most of these systems still follow a traditional lead configuration with large inter-electrode spacing. It has been shown, however, that it is possible to synthesize multiple ECG leads from only a few standard measurements [
18]. Only a few studies have investigated the possibility to obtain standard leads from short inter-electrode ECG lead systems [
19], but some findings suggest that even a 12-channel ECG reconstruction could be possible using a single 5 cm patch device, which incorporates multiple small-distance ECG lead recordings [
20]. Even though the lead field theory seems to support the concept of short-distance ECG recordings, no recommendations on application-specific placements have been established yet, and the evaluation of methods beyond ECG lead estimation from short-distance ECG leads is yet sparse [
21].
While the ECG reflects the electrical properties of the heart, structural abnormalities or defects do not necessarily manifest themselves in the ECG, but in abnormal heart sounds and murmurs [
22]. These changes can be assessed by the phonocardiogram (PCG). While stethoscope auscultation is a valuable and oftentimes first applied tool in primary health care, its digitization is a relatively recent development leading to applications including classification of mitral valve prolapse [
23] and the detection of other abnormal heart sounds [
24]. Currently available digital stethoscopes are designed close to the traditional implementation [
25], with a few exceptions lately emerging [
26]. To the best knowledge of the authors, no wearable digital stethoscope implementation was available until very recently.
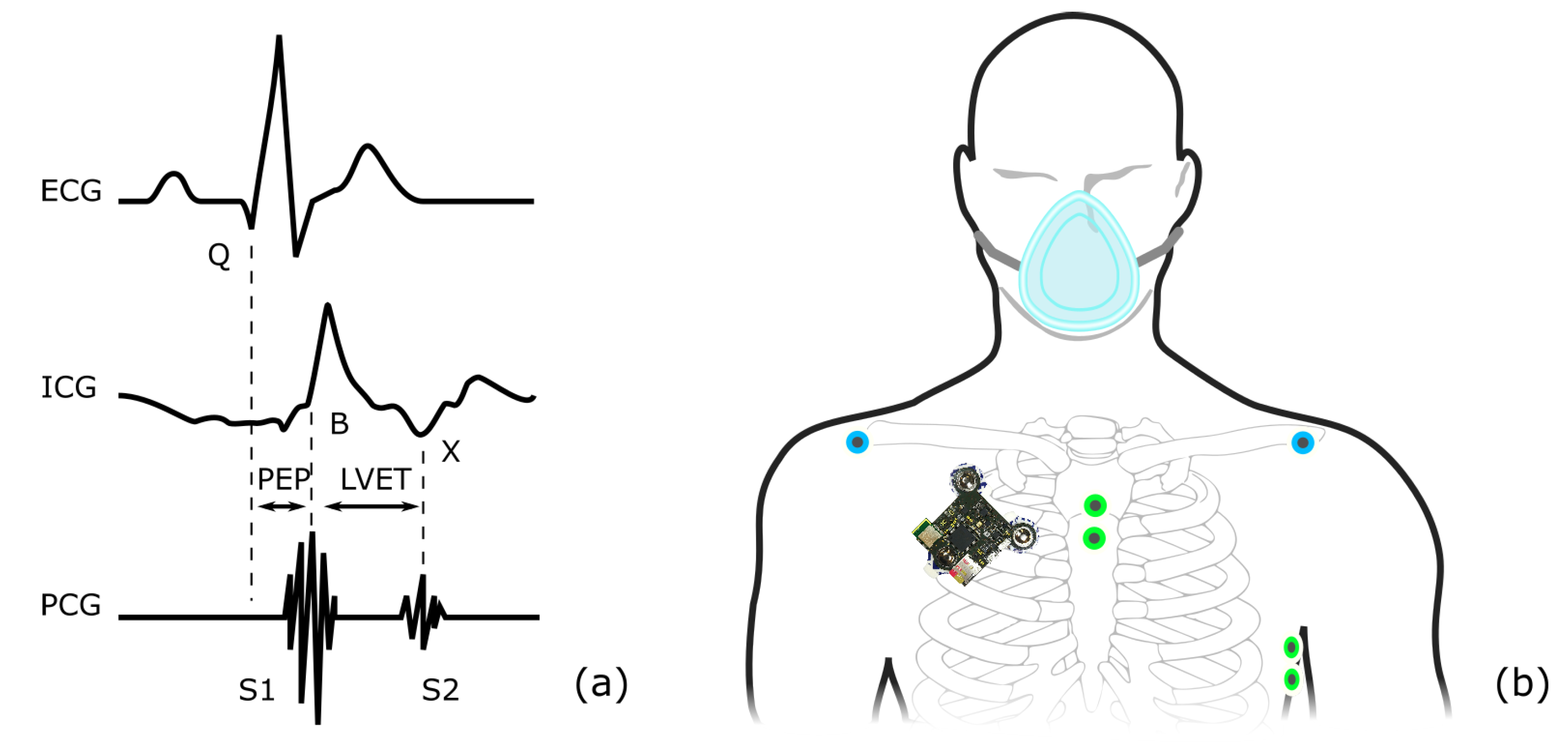
Combining ECG and PCG signals, systolic time intervals (STI) can be derived. STIs are known to relate closely to ventricular failure, the rate of ventricular pressure rise, preload, and other indices [
27]. Especially the pre-ejection period (PEP) and the left ventricular ejection time (LVET) have been found to be closely related to these measures. STIs provide insights into the temporal structure of the mechanical heart activity and can therefore contribute additional vital information about the cardiovascular system. Several approaches to assessing STIs are available, including echocardiography, impedance cardiography (ICG), photoplethysmography, seismocardiography (SCG), and PCG. Considering echocardiography as the reference, the PCG approach outperforms other methods when PEP and LVET are to be estimated [
28], and PCG and SCG deliver comparable results estimating total systolic time and the electromechanical delay [
29]. Therefore, several approaches of estimating STI from ECG and PCG have been reported [
30,
31]. Despite the work available on PEP estimation using the PCG, there seem to be diverging opinions about whether or not PCG can be used for PEP estimation in principle [
29,
32].
Assessing the function of the respiratory system is usually bound to obtrusive sensors. Especially in the context of sleep testing, flow sensors such as face masks or nasal cannula pressure sensors and effort sensors such as respiratory inductance plethysmography chest and abdominal belts are still recommended [
33]. While the development of an unobtrusive home sleep test system took important steps forward, the expert opinion remains that further research regarding the minimum number of parameters and methods of signal acquisitions is required [
34]. A promising technique for unobtrusive respiratory signal estimation is ECG-derived respiration (EDR), which is commonly used in conjunction with other signal modalities such as photoplethysmography (PPG) [
35]. An obvious advantage of EDR in the case of an available ECG is that no additional sensor is needed to estimate respiratory parameters. It is widely accepted that the ECG is modulated in three main aspects by the respiration: baseline wandering, heart rate, and QRS morphology. EDR methods aim to use one or more of these measures to estimate respiratory parameters. The extraction of the heart rate is less sensitive to ECG position and electrode distances due to the electrically strong QRS complex. The usability of morphological features, however, more strongly depends on the lead location. Especially in the context of small sensor systems placed at non-standard positions, this becomes important [
36].
Besides ECG and PPG based methods, several additional concepts of estimating respiratory parameters have emerged. Other approaches used to estimate respiratory signals include respiratory sounds, breathing air temperature, humidity and components [
37], the oscillometric cuff pressure, Korotkoff sounds, as well as the seismocardiogram (SCG) [
38]. For the latter, it has been shown that the morphology of the vibrational cardiac waveforms varies with the respiratory volume [
39,
40], and methods of extracting respiratory phases [
41,
42], effort [
43] and breathing states such as normal, breathless, long, and labored [
44] have been proposed. However, the interindividual morphological variations, as well as dependencies on numerous parameters including subject position, are still challenging [
45]. SCG and PCG are closely related [
46], with differences mostly defined by their frequency ranges [
47]. However, the application of PCG signals for respiratory signal estimation seems not to have been proposed yet. The authors assume that one reason is the unavailability of appropriate long-term monitoring stethoscope systems.
1.2. Scope of the Presented Work
With strong evidence that continuous, long-term cardiovascular and respiratory monitoring can improve clinical outcome [
48], optimize therapy success evaluation [
49], and be an effective strategy to assess sleep apnea [
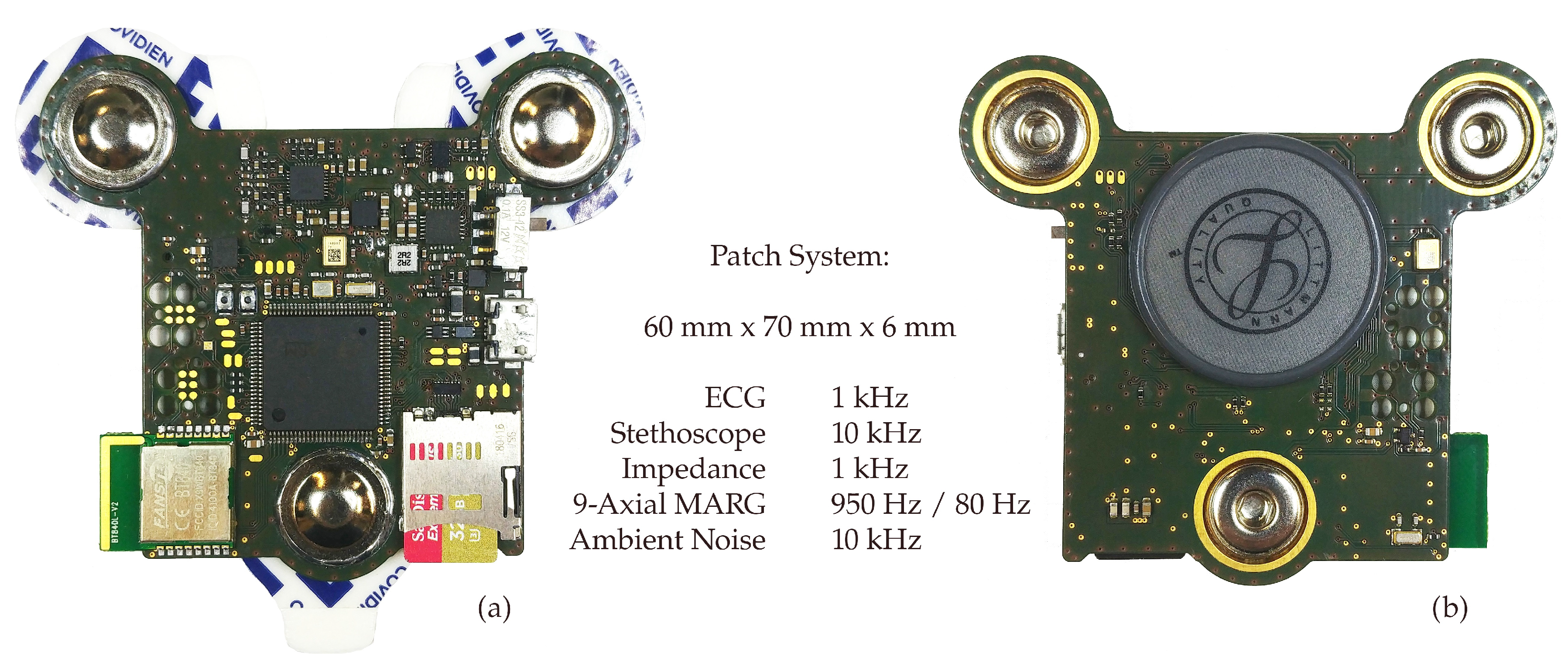
50], it is time to introduce a paradigm shift. Unimodal acquisition systems, such as wearable ECGs, can provide vital information. The real strength of wearable monitoring, however, lies beyond: in multimodality matched with unobtrusiveness. We recently presented a wearable, multimodal digital stethoscope patch, shown in
Figure 1. The system incorporates single-lead ECG and impedance pneumography at an electrode distance of 55 mm, 9-axial magnetic, angular rate and gravity (MARG) sensors, a digital stethoscope and ambient sound recording in a 60 mm × 70 mm × 6 mm device [
51]. In its current implementation, the system employs a thin 450 mAh lithium-polymer battery and realized runtimes exceeding 10 h even though not being optimized for low energy consumption yet.
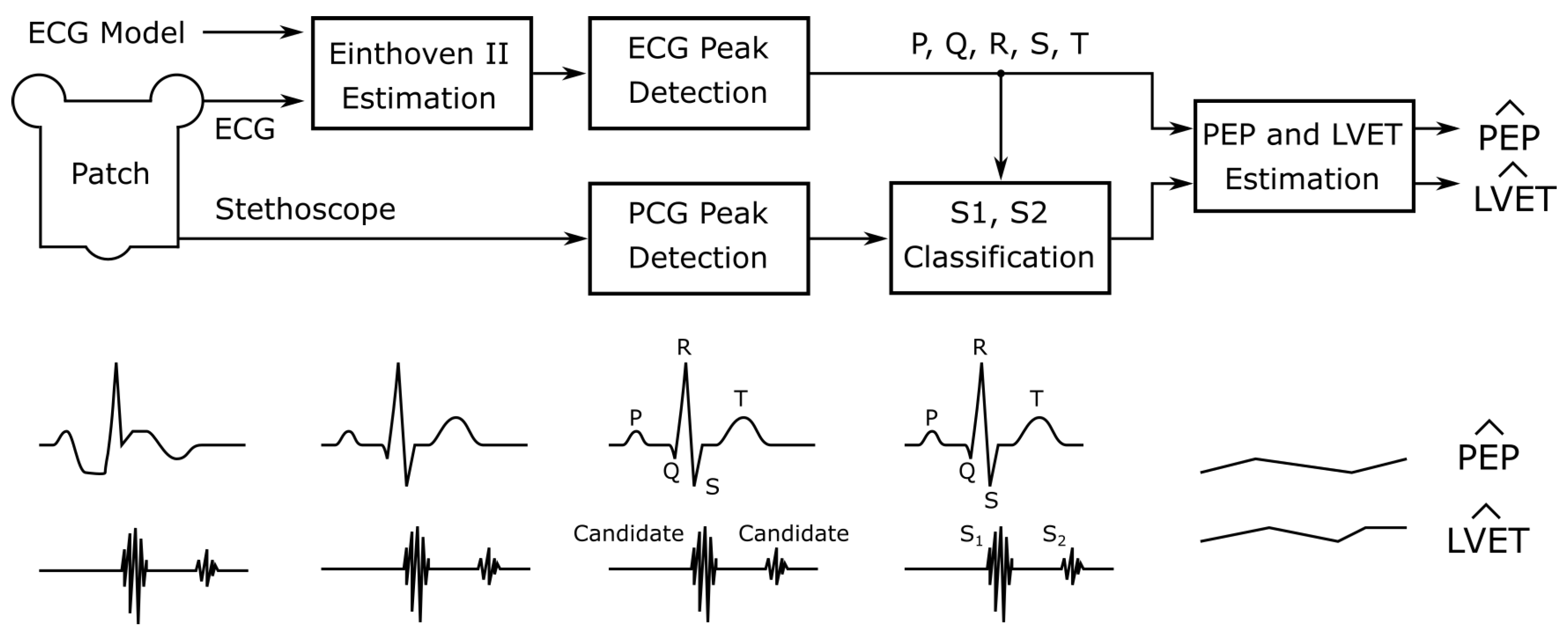
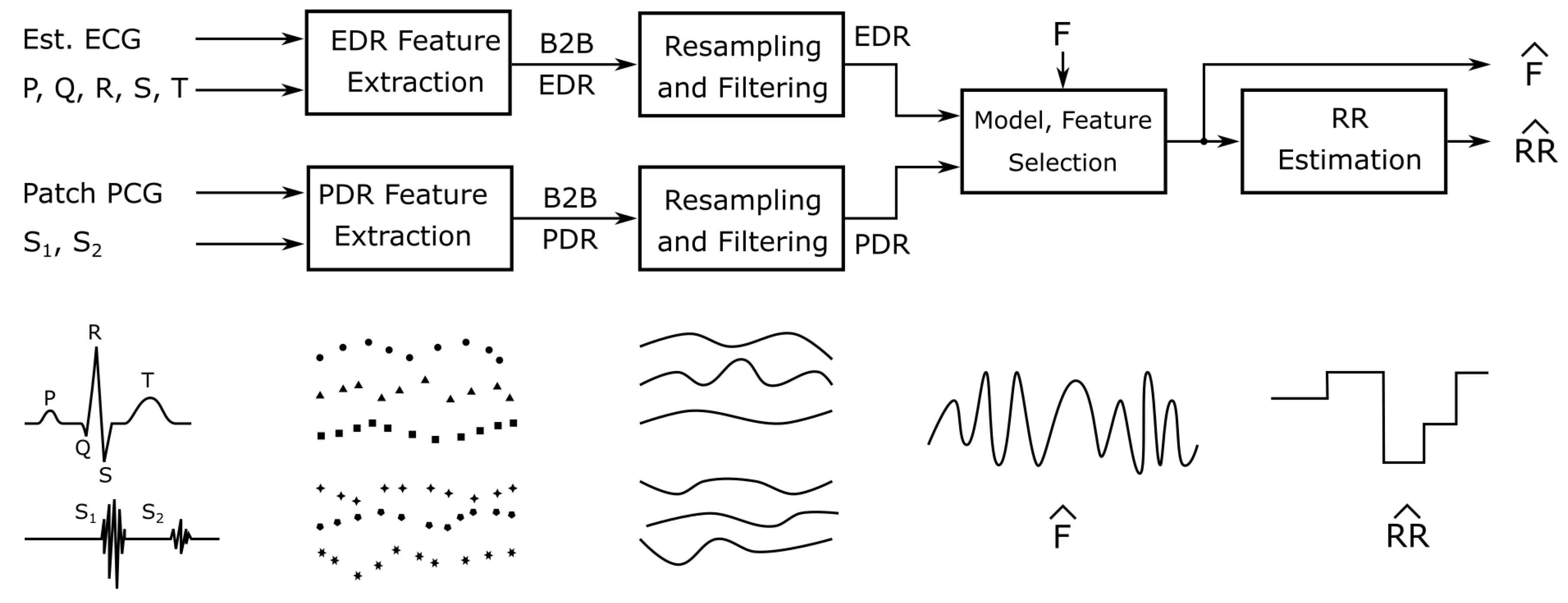
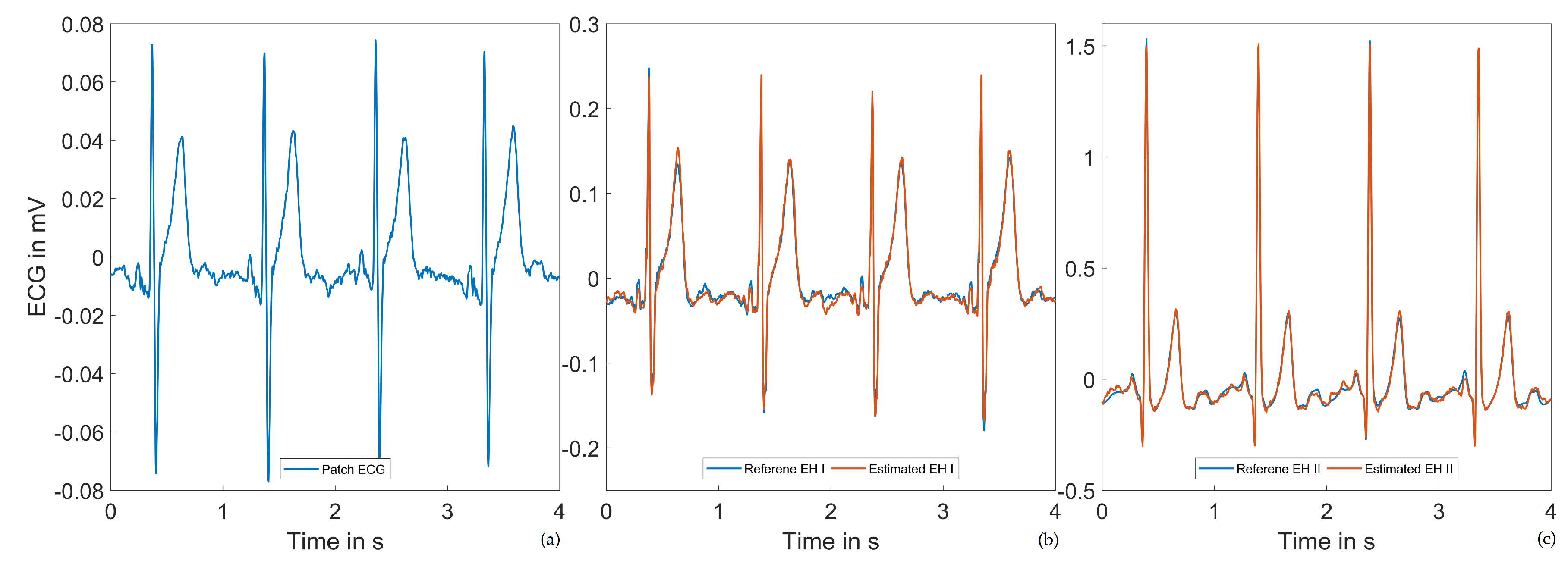
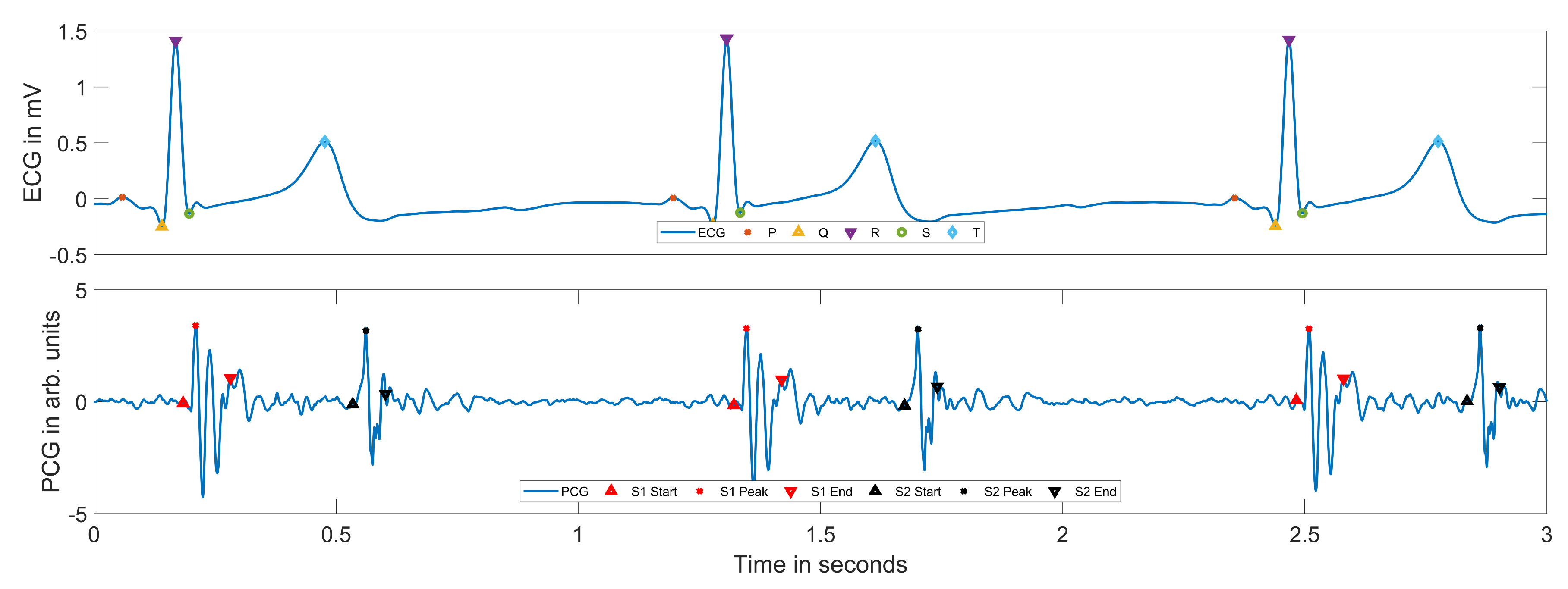
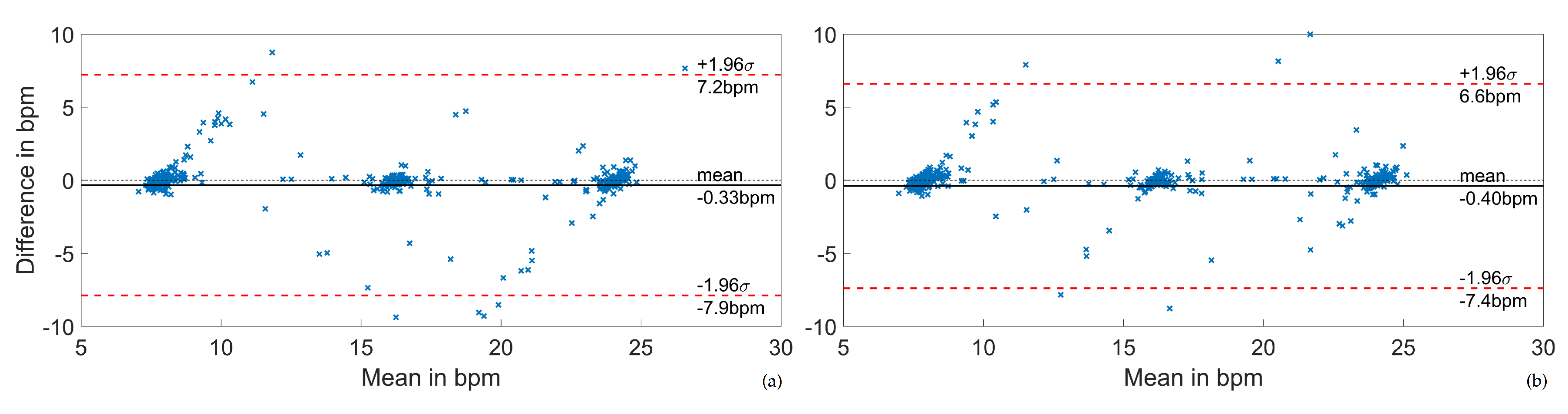
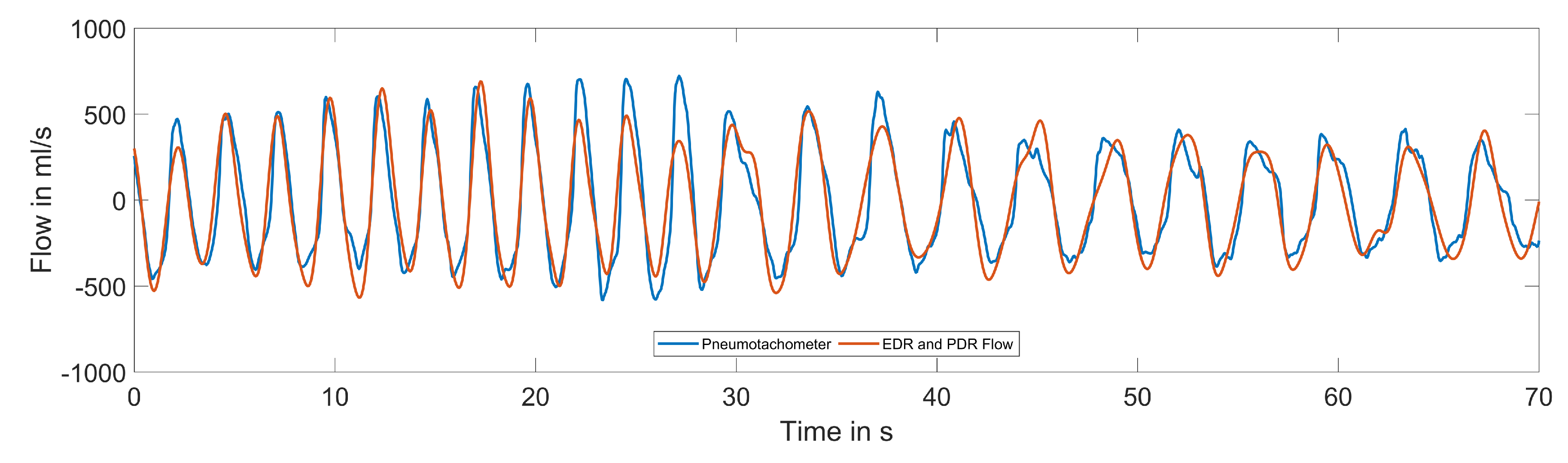
In this work, we present three distinct cardiovascular and respiratory monitoring applications using the ECG and digital stethoscope subsystems of our novel, multimodal wearable. We start by evaluating the performance of estimating standard Einthoven leads from the single, 55 mm short-distance lead implemented in the patch. Using the derived standard ECG leads, we classify the ECG fiducial points and the PCG S1 and S2 peaks in the stethoscope signal. This information is used to estimate PEP and LVET. Finally, respiratory signals and rates are estimated using ECG-derived respiration techniques combined with a novel phonocardiogram-derived respiration (PDR) approach.
Figure 2 gives a simplified overview of the processing steps. We evaluate our approaches using two commercially available reference systems (SOMNOmedics SOMNO HD
TM and Osypka ICON-Core
TM) acquiring reference ECG signals, PEP, LVET, and respiratory flow in a study including 10 healthy subjects with 33 min measurements each in different body positions. We aim to accelerate the development of truly multimodal, wearable biosignal acquisition and processing towards holistic long-term monitoring concepts.

 ,
, 















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}