
A Hybrid Deep Transfer Learning of CNN-Based LR-PCA for Breast Lesion Diagnosis via Medical Breast Mammograms

 , ,
, ,  , ,
, ,  and
and
Abstract
:1. Introduction
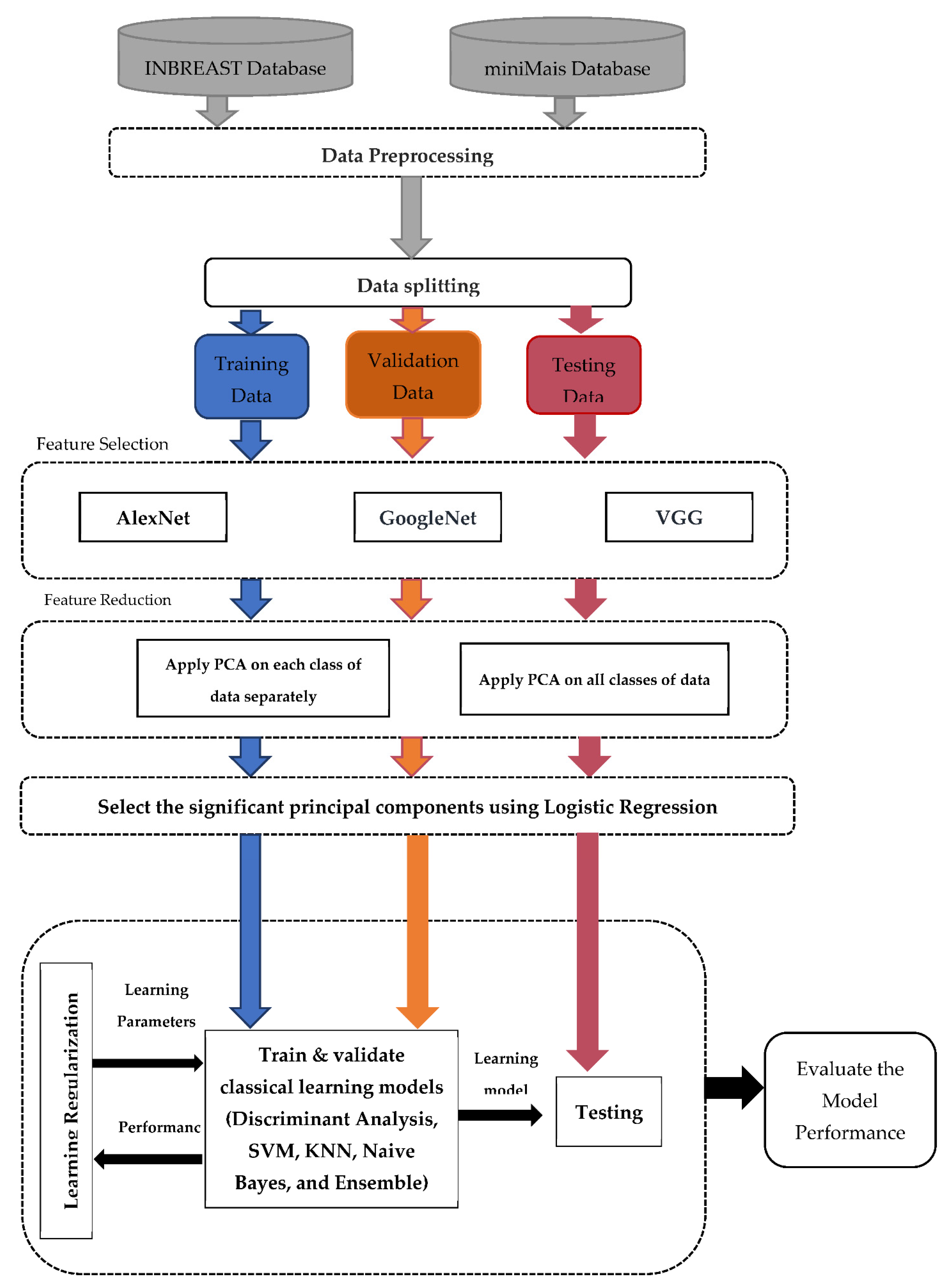
- A hybrid deep learning model of CNN-based LR-PCA has been designed for breast lesion classification purpose using the X-ray breast cancer images (i.e., mammograms).
- Generating more useful and powerful input information based on pseudo-colored images to enrich the input knowledge of deep learning models.
- A comprehensive study of transfer learning based on multiple convolutional networks has been conducted in order to extract the high-level deep features directly from the pre-trained backbone models.
- Resolving the multicollinearity problem that occurs among the derived high-level deep features from pre-trained by introducing a new method called LR-PCA. The optimized PCs are selected to perform the final classification purpose.
- A comprehensive evaluation process of the proposed CAD system is performed using two different public benchmark datasets: INbreast and mini-MAIS.
2. Related Work
3. Methodology
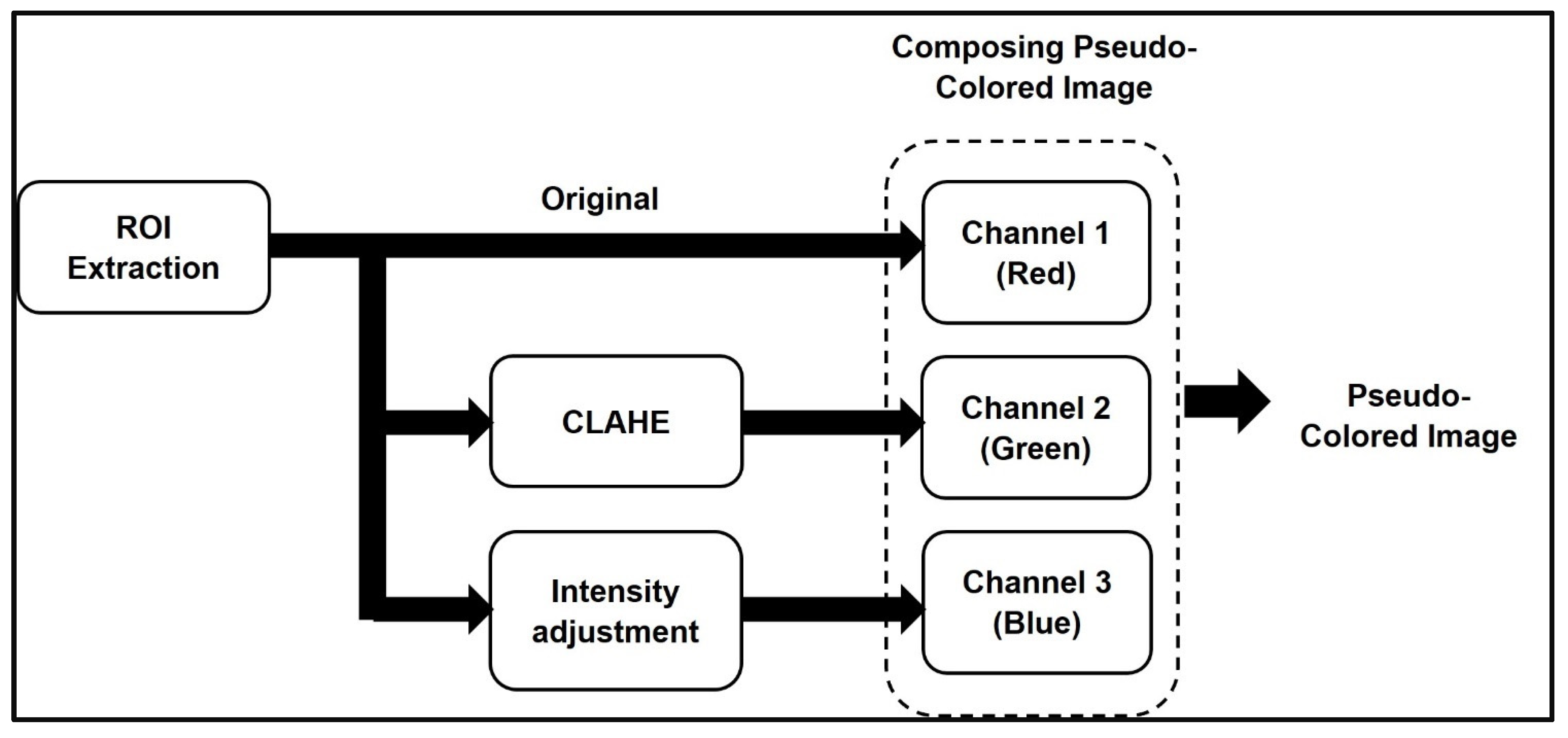
3.1. Data Preparation
- Channel 1 (Red) includes the original grayscale image.
- Channel 2 (Green) includes the enhanced image contrast of the grayscale image by transforming the values using contrast-limited adaptive histogram equalization (CLAHE) [65].
- Channel 3 (Blue) includes the processed image that maps the intensity values in the grayscale image to new values by saturating the bottom 1% and the top 1% of all pixel values. This operation increases the contrast of the output image.
3.2. Feature Selection Using Transfer Learning
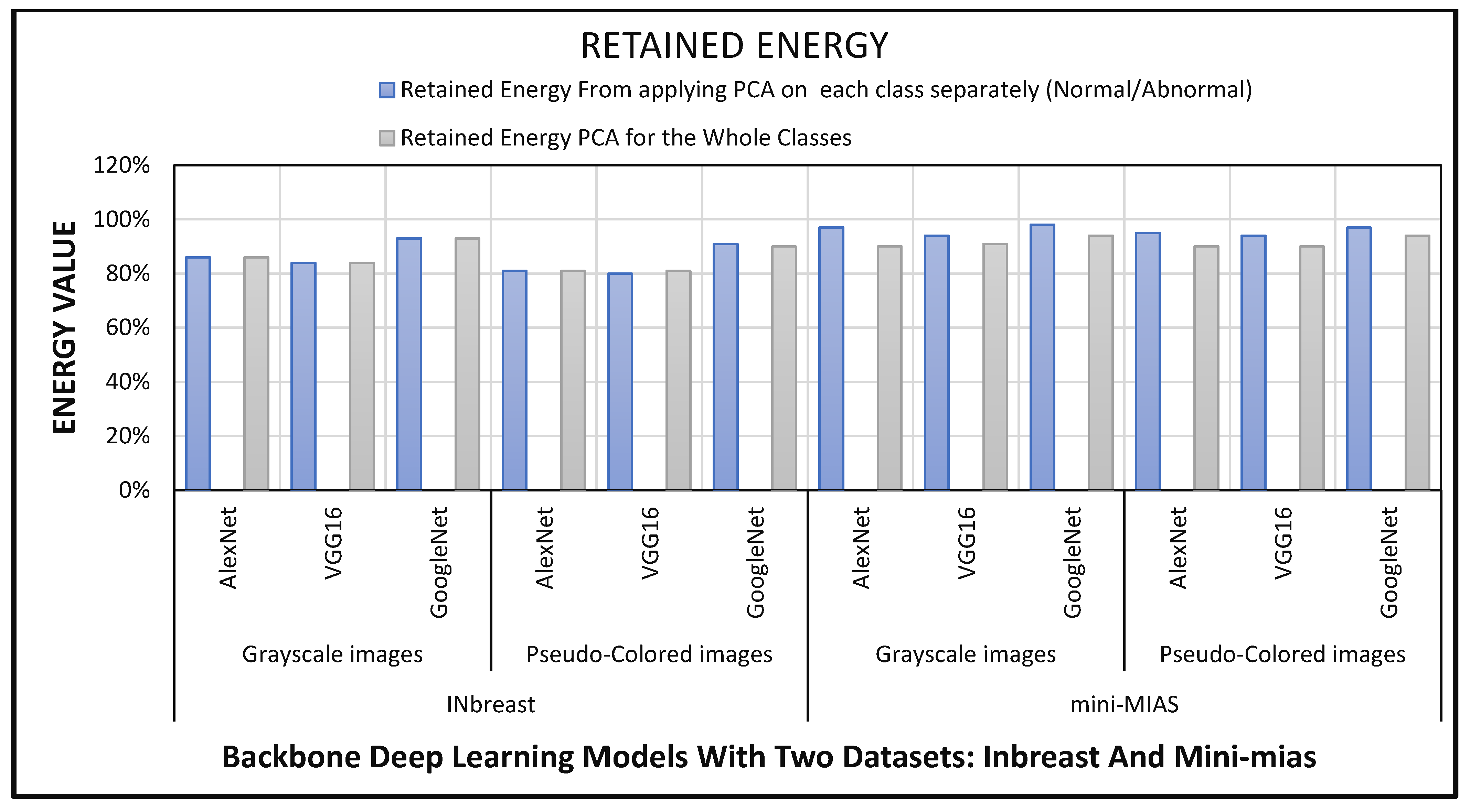
3.3. Dimensional Reduction Using LR-PCA
- Create a covariance matrix for your dataset.
- Determine the eigenvectors and eigenvalues of that matrix.
- Choose the desired number of dimensions and filter the eigenvectors to match, sorting them by their associated eigenvalue.
- Multiply the original space by the feature vector produced in the preceding step.
- Build a Multinomial Logistic Regression model for the retrieved features.
- Pick the principal components of the newly created LR model that have significant coefficients.
3.4. Classical ML Approaches for ROI Classification and Model Evaluation
4. Results and Discussion
5. Comparing the Performance and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Albeshan, S.M.; Alashban, Y.I. Incidence Trends of Breast Cancer in Saudi Arabia: A Joinpoint Regression Analysis (2004–2016). J. King Saud Univ. Sci. 2021, 33, 101578. [Google Scholar] [CrossRef]
- Sardanelli, F.; Fallenberg, E.M.; Clauser, P.; Trimboli, R.M.; Camps-Herrero, J.; Helbich, T.H.; Forrai, G. Mammography: An Update of the EUSOBI Recommendations on Information for Women. Insights Imaging 2017, 8, 11–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saadatmand, S.; Bretveld, R.; Siesling, S.; Tilanus-Linthorst, M.M.A. Influence of Tumour Stage at Breast Cancer Detection on Survival in Modern Times: Population Based Study in 173,797 Patients. BMJ 2015, 351, h4901. [Google Scholar] [CrossRef] [Green Version]
- Feig, S.A. Screening Mammography Benefit Controversies. Sorting the Evidence. Radiol. Clin. N. Am. 2014, 52, 455–480. [Google Scholar] [CrossRef]
- Dheeba, J.; Albert Singh, N.; Tamil Selvi, S. Computer-Aided Detection of Breast Cancer on Mammograms: A Swarm Intelligence Optimized Wavelet Neural Network Approach. J. Biomed. Inform. 2014, 49, 45–52. [Google Scholar] [CrossRef]
- Kolb, T.M.; Lichy, J.; Newhouse, J.H. Comparison of the Performance of Screening Mammography, Physical Examination, and Breast US and Evaluation of Factors That Influence Them: An Analysis of 27,825 Patient Evaluations. Radiology 2002, 225, 165–175. [Google Scholar] [CrossRef] [Green Version]
- Bozek, J.; Mustra, M.; Delac, K.; Grgic, M. A Survey of Image Processing Algorithms in Digital Mammography. Stud. Comput. Intell. 2009, 231, 631–657. [Google Scholar] [CrossRef]
- Cheng, H.D.; Shi, X.J.; Min, R.; Hu, L.M.; Cai, X.P.; Du, H.N. Approaches for Automated Detection and Classification of Masses in Mammograms. Pattern Recognit. 2006, 39, 646–668. [Google Scholar] [CrossRef]
- Anaya-Isaza, A.; Mera-Jiménez, L.; Zequera-Diaz, M. An Overview of Deep Learning in Medical Imaging. Inform. Med. Unlocked 2021, 26, 100723. [Google Scholar] [CrossRef]
- Khan, U.; Khan, S.; Rizwan, A.; Atteia, G.; Jamjoom, M.M.; Samee, N.A. Aggression Detection in Social Media from Textual Data Using Deep Learning Models. Appl. Sci. 2022, 12, 5083. [Google Scholar] [CrossRef]
- Samee, N.A.; Atteia, G.; Alkanhel, R.; Alhussan, A.A.; AlEisa, H.N. Hybrid Feature Reduction Using PCC-Stacked Autoencoders for Gold/Oil Prices Forecasting under COVID-19 Pandemic. Electronics 2022, 11, 991. [Google Scholar] [CrossRef]
- Abdel Samee, N.M. Classical and Deep Learning Paradigms for Detection and Validation of Key Genes of Risky Outcomes of HCV. Algorithms 2020, 13, 73. [Google Scholar] [CrossRef] [Green Version]
- Alhussan, A.A.; Gaafar, M.S.; Alharbi, M.; Marzouk, S.Y.; Alharbi, S.; ElRashidy, H.; Mabrouk, M.S.; AlEisa, H.N.; Samee, N.A. Prediction of the Judd–Ofelt Parameters of Dy3+-Doped Lead Borosilicate Using Artificial Neural Network. Electronics 2022, 11, 1045. [Google Scholar] [CrossRef]
- Alhussan, A.A.; AlEisa, H.N.; Atteia, G.; Solouma, N.H.; Seoud, R.A.A.A.A.; Ayoub, O.S.; Ghoneim, V.F.; Samee, N.A. ForkJoinPcc Algorithm for Computing the Pcc Matrix in Gene Co-Expression Networks. Electronics 2022, 11, 1174. [Google Scholar] [CrossRef]
- Alhussan, A.; Abdel Samee, N.; Ghoneim, V.; Kadah, Y. Evaluating Deep and Statistical Machine Learning Models in the Classification of Breast Cancer from Digital Mammograms. (IJACSA) Int. J. Adv. Comput. Sci. Appl. 2021, 12, 304–313. [Google Scholar] [CrossRef]
- BSI; AAMI. The Emergence of Artificial Intelligence and Machine Learning Algorithms in Healthcare: Recommendations to Support Governance and Regulation. Position Paper. Available online: https://www.bsigroup.com/globalassets/localfiles/en-gb/about-bsi/nsb/innovation/mhra-ai-paper-2019.pdf (accessed on 20 December 2021).
- Alolfe, M.A.; Youssef, A.M.; Kadah, Y.M.; Mohamed, A.S. Computer-Aided Diagnostic System Based on Wavelet Analysis for Microcalcification Detection in Digital Mammograms. In Proceedings of the 2008 Cairo International Biomedical Engineering Conference, Cairo, Egypt, 18–20 December 2008. [Google Scholar]
- Mousa, R.; Munib, Q.; Moussa, A. Breast Cancer Diagnosis System Based on Wavelet Analysis and Fuzzy-Neural. Expert Syst. Appl. 2005, 28, 713–723. [Google Scholar] [CrossRef]
- Winsberg, F.; Elkin, M.; Macy, J.; Bordaz, V.; Weymouth, W. Detection of Radiographic Abnormalities in Mammograms by Means of Optical Scanning and Computer Analysis. Radiology 1967, 89, 211–215. [Google Scholar] [CrossRef]
- Mohamed, W.A.; Alolfe, M.A.; Kadah, Y.M. Microcalcifications Enhancement in Digital Mammograms Using Fractal Modeling. In Proceedings of the 2008 Cairo International Biomedical Engineering Conference, Cairo, Egypt, 18–20 December 2008. [Google Scholar]
- Alolfe, M.A.; Mohamed, W.A.; Youssef, A.B.M.; Mohamed, A.S.; Kadah, Y.M. Computer Aided Diagnosis in Digital Mammography Using Combined Support Vector Machine and Linear Discriminant Analyasis Classification. In Proceedings of the International Conference on Image Processing, Cairo, Egypt, 7–10 November 2009; IEEE Computer Society: Washington, DC, USA, 2009; pp. 2609–2612. [Google Scholar]
- Jiang, J.; Yao, B.; Wason, A.M. A Genetic Algorithm Design for Microcalcification Detection and Classification in Digital Mammograms. Comput. Med. Imaging Graph. 2007, 31, 49–61. [Google Scholar] [CrossRef]
- Mohamed, W.A.; Kadah, Y.M. Computer Aided Diagnosis of Digital Mammograms. In Proceedings of the ICCES’07—2007 International Conference on Computer Engineering and Systems, Auckland, New Zealand, 11–14 July 2007; pp. 299–303. [Google Scholar]
- Alolfe, M.A.; Youssef, A.B.M.; Kadah, Y.M.; Mohamed, A.S. Development of a Computer-Aided Classification System for Cancer Detection from Digital Mammograms. In Proceedings of the National Radio Science Conference, Tanta, Egypt, 18–20 March 2008. [Google Scholar]
- Ayer, T.; Chen, Q.; Burnside, E.S. Artificial Neural Networks in Mammography Interpretation and Diagnostic Decision Making. Comput. Math. Methods Med. 2013, 2013, 832509. [Google Scholar] [CrossRef] [Green Version]
- Xu, W.; Li, H.; Xu, P. A New ANN-Based Detection Algorithm of the Masses in Digital Mammograms. In Proceedings of the IEEE ICIT 2007—2007 IEEE International Conference on Integration Technology, Burlingame, CA, USA, 4–6 June 2007; pp. 26–30. [Google Scholar]
- al Sharkawy, M.; Sharkas, M.; Ragab, D. Breast Cancer Detection Using Support Vector Machine Technique Applied on Extracted Electromagnetic Waves. Appl. Comput. Electromagn. Soc. J. 2012, 27, 292–301. [Google Scholar]
- Ragab, D.A.; Sharkas, M.; Attallah, O. Breast Cancer Diagnosis Using an Efficient CAD System Based on Multiple Classifiers. Diagnostics 2019, 9, 165. [Google Scholar] [CrossRef] [Green Version]
- Assiri, A.S.; Nazir, S.; Velastin, S.A. Breast Tumor Classification Using an Ensemble Machine Learning Method. J. Imaging 2020, 6, 39. [Google Scholar] [CrossRef]
- Liu, N.; Qi, E.S.; Xu, M.; Gao, B.; Liu, G.Q. A Novel Intelligent Classification Model for Breast Cancer Diagnosis. Inf. Processing Manag. 2019, 56, 609–623. [Google Scholar] [CrossRef]
- Kadah, Y.M.; Farag, A.A.; Zurada, J.M.; Badawi, A.M.; Youssef, A.B.M. Classification Algorithms for Quantitative Tissue Characterization of Diffuse Liver Disease from Ultrasound Images. IEEE Trans. Med. Imaging 1996, 15, 466–478. [Google Scholar] [CrossRef]
- Jiang, F.; Liu, H.; Yu, S.; Xie, Y. Breast Mass Lesion Classification in Mammograms by Transfer Learning. In Proceedings of the ACM International Conference Proceeding Series; Association for Computing Machinery: New York, NY, USA, 2017; pp. 59–62. [Google Scholar]
- Tan, Y.J.; Sim, K.S.; Ting, F.F. Breast Cancer Detection Using Convolutional Neural Networks for Mammogram Imaging System. In Proceedings of the 2017 International Conference on Robotics, Automation and Sciences, Melaka, Malaysia, 27–29 November 2017; Institute of Electrical and Electronics Engineers Inc.: New York, NY, USA, 2018; pp. 1–5. [Google Scholar]
- Hepsaǧ, P.U.; Özel, S.A.; Yazici, A. Using Deep Learning for Mammography Classification. In Proceedings of the 2nd International Conference on Computer Science and Engineering, Antalya, Turkey, 5–8 October 2017; Institute of Electrical and Electronics Engineers Inc.: New York, NY, USA, 2017; pp. 418–423. [Google Scholar]
- Zhang, X.; Zhang, Y.; Han, E.Y.; Jacobs, N.; Han, Q.; Wang, X.; Liu, J. Whole Mammogram Image Classification with Convolutional Neural Networks. In Proceedings of the 2017 IEEE International Conference on Bioinformatics and Biomedicine, Kansas City, MO, USA, 13–16 November 2017; Institute of Electrical and Electronics Engineers Inc.: New York, NY, USA, 2017; pp. 700–704. [Google Scholar]
- Wu, H.; Liu, Q.; Liu, X. A Review on Deep Learning Approaches to Image Classification and Object Segmentation. Comput. Mater. Contin. 2019, 60, 575–597. [Google Scholar] [CrossRef] [Green Version]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the Inception Architecture for Computer Vision. In Proceedings of the IEEE Computer Society Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; IEEE Computer Society: Washington, DC, USA, 2016; pp. 2818–2826. [Google Scholar]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. ImageNet Classification with Deep Convolutional Neural Networks. In Advances in Neural Information Processing Systems 25, Proceedings of the 26th Annual Conference on Neural Information Processing Systems 2012, Lake Tahoe, NV, USA, 3–6 December 2012; ACM Digital Library: New York, NY, USA, 2012. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very Deep Convolutional Networks for Large-Scale Image Recognition. In Proceedings of the 3rd International Conference on Learning Representations, ICLR 2015-Conference Track Proceedings, International Conference on Learning Representations, San Diego, CA, USA, 7–9 May 2015. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the IEEE Computer Society Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; IEEE Computer Society: Washington, DC, USA, 2016; pp. 770–778. [Google Scholar]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going Deeper with Convolutions. In Proceedings of the IEEE Computer Society Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; IEEE Computer Society: Washington, DC, USA, 2015; pp. 1–9. [Google Scholar]
- Yemini, M.; Zigel, Y.; Lederman, D. Detecting Masses in Mammograms Using Convolutional Neural Networks and Transfer Learning. In Proceedings of the 2018 IEEE International Conference on the Science of Electrical Engineering in Israel, Sydney, Australia, 15–17 June 2018; Institute of Electrical and Electronics Engineers Inc.: New York, NY, USA, 2019. [Google Scholar]
- Hasan, M.K.; Aleef, T.A.; Roy, S. Automatic Mass Classification in Breast Using Transfer Learning of Deep Convolutional Neural Network and Support Vector Machine. In Proceedings of the 2020 IEEE Region 10 Symposium, Dhaka, Bangladesh, 5–7 June 2020; Institute of Electrical and Electronics Engineers Inc.: New York, NY, USA, 2020; pp. 110–113. [Google Scholar]
- Abd-Elsalam, N.M.; Fawzi, S.A.; Kandil, A.H. Comparing Different Pre-Trained Models Based on Transfer Learning Technique in Classifying Mammogram Masses. In Proceedings of the 30th International Conference on Computer Theory and Applications, Virtual, 12–14 December 2020; Institute of Electrical and Electronics Engineers Inc.: New York, NY, USA, 2020; pp. 54–59. [Google Scholar]
- Falconi, L.G.; Perez, M.; Aguilar, W.G. Transfer Learning in Breast Mammogram Abnormalities Classification with Mobilenet and Nasnet. In Proceedings of the International Conference on Systems, Signals, and Image Processing, Osijek, Croatia, 5–7 June 2019; IEEE Computer Society: Washington, DC, USA, 2019; pp. 109–114. [Google Scholar]
- Falconi, L.; Perez, M.; Aguilar, W.; Conci, A. Transfer Learning and Fine Tuning in Mammogram Bi-Rads Classification. In Proceedings of the IEEE Symposium on Computer-Based Medical Systems, Rochester, MN, USA, 28–30 July 2020; Institute of Electrical and Electronics Engineers Inc.: New York, NY, USA, 2020; pp. 475–480. [Google Scholar]
- Samala, R.K.; Chan, H.P.; Hadjiiski, L.M.; Helvie, M.A.; Cha, K.H.; Richter, C.D. Multi-Task Transfer Learning Deep Convolutional Neural Network: Application to Computer-Aided Diagnosis of Breast Cancer on Mammograms. Phys. Med. Biol. 2017, 62, 8894–8908. [Google Scholar] [CrossRef]
- Weiss, K.; Khoshgoftaar, T.M.; Wang, D.D. A Survey of Transfer Learning. J. Big Data 2016, 3, 9. [Google Scholar] [CrossRef] [Green Version]
- Wimmer, M.; Sluiter, G.; Major, D.; Lenis, D.; Berg, A.; Neubauer, T.; Buhler, K. Multi-Task Fusion for Improving Mammography Screening Data Classification. IEEE Trans. Med. Imaging 2021, 41, 937–950. [Google Scholar] [CrossRef]
- Wang, Z.; Li, M.; Wang, H.; Jiang, H.; Yao, Y.; Zhang, H.; Xin, J. Breast Cancer Detection Using Extreme Learning Machine Based on Feature Fusion with CNN Deep Features. IEEE Access 2019, 7, 105146–105158. [Google Scholar] [CrossRef]
- Ragab, D.A.; Attallah, O.; Sharkas, M.; Ren, J.; Marshall, S. A Framework for Breast Cancer Classification Using Multi-DCNNs. Comput. Biol. Med. 2021, 131, 104245. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Yuan, Y. Dimension Reduction of Image Deep Feature Using PCA. J. Vis. Commun. Image Represent. 2019, 63, 102578. [Google Scholar] [CrossRef]
- Meyer, P.; Noblet, V.; Mazzara, C.; Lallement, A. Survey on Deep Learning for Radiotherapy. Comput. Biol. Med. 2018, 98, 126–146. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, A.; Haenlein, M. Siri, Siri, in My Hand: Who’s the Fairest in the Land? On the Interpretations, Illustrations, and Implications of Artificial Intelligence. Bus. Horiz. 2019, 62, 15–25. [Google Scholar] [CrossRef]
- Topol, E.J. High-Performance Medicine: The Convergence of Human and Artificial Intelligence. Nat. Med. 2019, 25, 44–56. [Google Scholar] [CrossRef]
- Liu, Z.; Jin, L.; Chen, J.; Fang, Q.; Ablameyko, S.; Yin, Z.; Xu, Y. A Survey on Applications of Deep Learning in Microscopy Image Analysis. Comput. Biol. Med. 2021, 134, 104523. [Google Scholar] [CrossRef]
- Castiglioni, I.; Rundo, L.; Codari, M.; di Leo, G.; Salvatore, C.; Interlenghi, M.; Gallivanone, F.; Cozzi, A.; D’Amico, N.C.; Sardanelli, F. AI Applications to Medical Images: From Machine Learning to Deep Learning. Phys. Med. 2021, 83, 9–24. [Google Scholar] [CrossRef] [PubMed]
- Alzubaidi, L.; Al-Shamma, O.; Fadhel, M.A.; Farhan, L.; Zhang, J.; Duan, Y. Optimizing the Performance of Breast Cancer Classification by Employing the Same Domain Transfer Learning from Hybrid Deep Convolutional Neural Network Model. Electronics 2020, 9, 445. [Google Scholar] [CrossRef] [Green Version]
- Suckling, J.; Parker, J.; Dance, D.; Astley, S.; Hutt, I.; Boggis, C.; Ricketts, I.; Stamatakis, E.; Cerneaz, N.; Kok, S.; et al. The Mammographic Image Analysis Society Digital Mammogram Database. Excerpta Med. Int. Congr. Ser. 1994, 1069, 375–378. [Google Scholar]
- Moreira, I.C.; Amaral, I.; Domingues, I.; Cardoso, A.; Cardoso, M.J.; Cardoso, J.S. INbreast: Toward a Full-Field Digital Mammographic Database. Acad. Radiol. 2012, 19, 236–248. [Google Scholar] [CrossRef] [Green Version]
- Feature Selection in Computer Aided Diagnostic System for Microcalcification Detection in Digital Mammograms|IEEE Conference Publication|IEEE Xplore. Available online: https://ieeexplore.ieee.org/document/5233466 (accessed on 18 June 2022).
- Al-antari, M.A.; Al-masni, M.A.; Park, S.U.; Park, J.H.; Metwally, M.K.; Kadah, Y.M.; Han, S.M.; Kim, T.S. An Automatic Computer-Aided Diagnosis System for Breast Cancer in Digital Mammograms via Deep Belief Network. J. Med. Biol. Eng. 2018, 38, 443–456. [Google Scholar] [CrossRef]
- Al-antari, M.A.; Han, S.M.; Kim, T.S. Evaluation of Deep Learning Detection and Classification towards Computer-Aided Diagnosis of Breast Lesions in Digital X-Ray Mammograms. Comput. Methods Programs Biomed. 2020, 196, 105584. [Google Scholar] [CrossRef]
- Yadav, G.; Maheshwari, S.; Agarwal, A. Contrast Limited Adaptive Histogram Equalization Based Enhancement for Real Time Video System. In Proceedings of the 2014 International Conference on Advances in Computing, Communications and Informatics, Delhi, India, 24–27 September 2014; Institute of Electrical and Electronics Engineers Inc.: New York, NY, USA, 2014; pp. 2392–2397. [Google Scholar]
- Fujita, H. AI-Based Computer-Aided Diagnosis (AI-CAD): The Latest Review to Read First. Radiol. Phys. Technol. 2020, 13, 6–19. [Google Scholar] [CrossRef] [PubMed]
- Hssayeni, M.D.; Saxena, S.; Ptucha, R.; Savakis, A. Distracted Driver Detection: Deep Learning vs. Handcrafted Features. In Proceedings of the IS and T International Symposium on Electronic Imaging Science and Technology, Society for Imaging Science and Technology, Burlingame, CA, USA, 29 January–2 February 2017; Volume 29, pp. 20–26. [Google Scholar]
- Abdelhafiz, D.; Yang, C.; Ammar, R.; Nabavi, S. Deep Convolutional Neural Networks for Mammography: Advances, Challenges and Applications. BMC Bioinform. 2019, 20, 281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, J.Y.-L.; Leow, S.M.H.; Bea, K.T.; Cheng, W.K.; Phoong, S.W.; Hong, Z.-W.; Chen, Y.-L. Mitigating the Multicollinearity Problem and Its Machine Learning Approach: A Review. Mathematics 2022, 10, 1283. [Google Scholar] [CrossRef]
- Wang, X.; Paliwal, K.K. Feature Extraction and Dimensionality Reduction Algorithms and Their Applications in Vowel Recognition. Pattern Recognit. 2003, 36, 2429–2439. [Google Scholar] [CrossRef]
- Atteia, G.; Abdel Samee, N.; Zohair Hassan, H. DFTSA-Net: Deep Feature Transfer-Based Stacked Autoencoder Network for DME Diagnosis. Entropy 2021, 23, 1251. [Google Scholar] [CrossRef]
- Liu, X.; Mei, M.; Liu, J.; Hu, W. Microcalcification Detection in Full-Field Digital Mammograms with PFCM Clustering and Weighted SVM-Based Method. Eurasip J. Adv. Signal Process. 2015, 2015, 73. [Google Scholar] [CrossRef] [Green Version]
- Mina, L.M.; Mat Isa, N.A. Breast Abnormality Detection in Mammograms Using Artificial Neural Network. In Proceedings of the I4CT 2015—2015 2nd International Conference on Computer, Communications, and Control Technology, Art Proceeding, Kuching, Malaysia, 21–23 April 2015; Institute of Electrical and Electronics Engineers Inc.: New York, NY, USA, 2015; pp. 258–263. [Google Scholar]
- Xie, W.; Li, Y.; Ma, Y. Breast Mass Classification in Digital Mammography Based on Extreme Learning Machine. Neurocomputing 2016, 173, 930–941. [Google Scholar] [CrossRef]
- Jian, W.; Sun, X.; Luo, S. Computer-Aided Diagnosis of Breast Microcalcifications Based on Dual-Tree Complex Wavelet Transform. Biomed. Eng. Online 2012, 11, 96. [Google Scholar] [CrossRef] [Green Version]
- Vijayarajeswari, R.; Parthasarathy, P.; Vivekanandan, S.; Basha, A.A. Classification of Mammogram for Early Detection of Breast Cancer Using SVM Classifier and Hough Transform. Meas. J. Int. Meas. Confed. 2019, 146, 800–805. [Google Scholar] [CrossRef]
- Phadke, A.C.; Rege, P.P. Fusion of Local and Global Features for Classification of Abnormality in Mammograms. Sadhana-Acad. Proc. Eng. Sci. 2016, 41, 385–395. [Google Scholar] [CrossRef] [Green Version]
- Oliver, A.; Freixenet, J.; Zwiggelaar, R. Automatic Classification of Breast Density. In Proceedings of the International Conference on Image Processing, Genoa, Italy, 11–14 September 2005; Volume 2, pp. 1258–1261. [Google Scholar]
- Xu, J.; Li, C.; Zhou, Y.; Mou, L.; Zheng, H.; Wang, S. Classifying Mammographic Breast Density by Residual Learning. arXiv 2018, arXiv:1809.10241 2018. [Google Scholar]
- Nasir Khan, H.; Shahid, A.R.; Raza, B.; Dar, A.H.; Alquhayz, H. Multi-View Feature Fusion Based Four Views Model for Mammogram Classification Using Convolutional Neural Network. IEEE Access 2019, 7, 165724–165733. [Google Scholar] [CrossRef]
- Zhang, H.; Wu, R.; Yuan, T.; Jiang, Z.; Huang, S.; Wu, J.; Hua, J.; Niu, Z.; Ji, D. DE-Ada*: A Novel Model for Breast Mass Classification Using Cross-Modal Pathological Semantic Mining and Organic Integration of Multi-Feature Fusions. Inf. Sci. 2020, 539, 461–486. [Google Scholar] [CrossRef]
- Al-masni, M.A.; Al-antari, M.A.; Park, J.M.; Gi, G.; Kim, T.Y.; Rivera, P.; Valarezo, E.; Choi, M.T.; Han, S.M.; Kim, T.S. Simultaneous Detection and Classification of Breast Masses in Digital Mammograms via a Deep Learning YOLO-Based CAD System. Comput. Methods Programs Biomed. 2018, 157, 85–94. [Google Scholar] [CrossRef]
- Song, R.; Li, T.; Wang, Y. Mammographic Classification Based on XGBoost and DCNN with Multi Features. IEEE Access 2020, 8, 75011–75021. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model Predictors | SE | t Statistics | p-Value |
|---|---|---|---|
| PC1 | 1.1638 | 7.8235 | 5.14 × 10−15 |
| PC2 | 0.0008 | 14.7641 | 0 |
| PC3 | 0.0013 | −11.1861 | 4.77 × 10−29 |
| PC4 | 0.0014 | −13.4629 | 2.59 × 10−41 |
| PC5 | 0.0019 | −12.9322 | 2.96 × 10−38 |
| PC6 | 0.0015 | −2.1592 | 0.030837 |
| PC7 | 0.0022 | 13.8375 | 1.51 × 10−43 |
| PC8 | 0.0019 | −0.0055 | 0.995623 |
| PC9 | 0.0023 | −9.0287 | 1.74 × 10−19 |
| PC10 | 0.0026 | 1.2018 | 0.22944 |
| PC11 | 0.0026 | −2.1862 | 0.028801 |
| PC12 | 0.0027 | 1.6188 | 0.1055 |
| PC13 | 0.0032 | −7.2077 | 5.69 × 10−13 |
| PC14 | 0.0033 | −8.3964 | 4.61 × 10−17 |
| PC15 | 0.0034 | −0.7858 | 0.431973 |
| PC16 | 0.0035 | 1.8389 | 0.065923 |
| PC17 | 0.0037 | 0.0854 | 0.931964 |
| PC18 | 0.0036 | 5.9441 | 2.78 × 10−9 |
| PC19 | 0.0035 | 1.8050 | 0.07108 |
| PC20 | 0.0036 | −6.9300 | 4.21 × 10−12 |
| PC21 | 0.0040 | 4.9057 | 9.31 × 10−7 |
| PC22 | 0.0040 | −4.4528 | 8.47 × 10−6 |
| PC23 | 0.0043 | 11.6463 | 2.40 × 10−31 |
| PC24 | 0.0045 | −4.8968 | 9.74 × 10−7 |
| PC25 | 0.0048 | −9.4881 | 2.35 × 10−21 |
| PC26 | 0.0047 | 0.7119 | 0.476501 |
| PC27 | 0.0047 | −0.6445 | 0.519277 |
| PC28 | 0.0050 | −2.6172 | 0.008865 |
| PC29 | 0.0053 | 0.9396 | 0.347413 |
| PC30 | 0.0054 | −6.5354 | 6.34 × 10−11 |
| PC31 | 0.0050 | −1.4328 | 0.151915 |
| PC32 | 0.0054 | −0.5211 | 0.602287 |
| PC33 | 0.0052 | 2.2693 | 0.023249 |
| PC34 | 0.0057 | −0.6697 | 0.503072 |
| PC35 | 0.0058 | −0.1642 | 0.869595 |
| PC36 | 0.0056 | 6.0392 | 1.55 × 10−9 |
| PC37 | 0.0059 | −1.5046 | 0.132437 |
| PC38 | 0.0061 | −2.5012 | 0.012377 |
| PC39 | 0.0060 | 0.5841 | 0.559178 |
| PC40 | 0.0062 | 2.9399 | 0.003284 |
| PC41 | 0.0065 | 3.0751 | 0.002104 |
| PC42 | 0.0065 | −6.5521 | 5.67 × 10−11 |
| PC43 | 0.0065 | −3.3909 | 0.000697 |
| PC44 | 0.0068 | −0.2496 | 0.802873 |
| PC45 | 0.0063 | 3.0721 | 0.002125 |
| PC46 | 0.0065 | −1.5325 | 0.125403 |
| PC47 | 0.0064 | −1.5169 | 0.1293 |
| PC48 | 0.0067 | −2.3565 | 0.01845 |
| PC49 | 0.0069 | 1.7933 | 0.072918 |
| PC50 | 0.0071 | −3.3454 | 0.000822 |
| Dataset | LR-PCA | Feature Extractor | Classification Model | Acc. | SE | SP | PRE | FNR | FPR | AUC | MCC | F1-Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Grayscale images | Across all classes | AlexNet | Ensemble (subspace KNN) | 97.20 | 96.75 | 97.67 | 97.65 | 3.25 | 2.33 | 100 | 94.43 | 97.20 |
| VGG16 | Ensemble (subspace KNN) | 95.90 | 94.12 | 97.77 | 97.68 | 5.88 | 2.23 | 99.0 | 91.95 | 95.87 | ||
| GoogleNet | Ensemble (subspace KNN) | 93.90 | 92.29 | 95.54 | 95.39 | 7.71 | 4.46 | 98.0 | 87.88 | 93.81 | ||
| Pseudo-Colored images | AlexNet | Ensemble (subspace KNN) | 98.00 | 96.96 | 98.88 | 98.86 | 3.04 | 1.12 | 95.22 | 95.86 | 97.90 | |
| VGG16 | Ensemble (subspace KNN) | 97.90 | 96.65 | 99.09 | 99.06 | 3.35 | 0.91 | 100 | 95.77 | 97.84 | ||
| GoogleNet | Ensemble (subspace KNN) | 95.10 | 92.90 | 97.06 | 96.93 | 7.10 | 2.94 | 99.0 | 90.04 | 94.87 | ||
| Grayscale images | For each class separately | AlexNet | Ensemble (subspace KNN) | 97.20 | 96.65 | 97.67 | 97.64 | 3.35 | 2.33 | 100 | 94.33 | 97.15 |
| VGG16 | Ensemble (subspace KNN) | 95.90 | 95.13 | 96.65 | 96.60 | 4.87 | 3.35 | 99.0 | 91.80 | 95.86 | ||
| GoogleNet | Ensemble (subspace KNN) | 94.60 | 92.90 | 97.06 | 96.93 | 7.10 | 2.94 | 99.0 | 90.04 | 94.87 | ||
| Pseudo-Colored images | AlexNet | Ensemble (subspace KNN) | 98.60 | 98.28 | 98.99 | 98.98 | 1.72 | 1.01 | 100 | 97.26 | 98.63 | |
| VGG16 | Ensemble (subspace KNN) | 98.10 | 97.87 | 98.28 | 98.27 | 2.13 | 1.72 | 99.0 | 96.15 | 98.07 | ||
| GoogleNet | Ensemble (subspace KNN) | 94.50 | 92.60 | 96.45 | 96.31 | 7.40 | 3.55 | 98.0 | 89.11 | 94.42 | ||
| Grayscale images | Not applied | AlexNet | KNN | 96.00 | 94.61 | 97.67 | 97.59 | 5.39 | 2.33 | 96.0 | 92.33 | 96.07 |
| VGG16 | KNN | 95.80 | 94.53 | 97.16 | 97.09 | 5.47 | 2.84 | 99.0 | 91.72 | 95.79 | ||
| GoogleNet | KNN | 93.40 | 92.01 | 95.02 | 94.89 | 7.99 | 4.98 | 98.0 | 87.06 | 93.43 | ||
| Pseudo-Colored | AlexNet | KNN | 96.80 | 95.13 | 98.48 | 98.43 | 4.87 | 1.52 | 96.0 | 93.66 | 96.75 | |
| VGG16 | KNN | 96.40 | 95.13 | 97.67 | 97.61 | 4.87 | 2.33 | 96.0 | 92.83 | 96.35 | ||
| GoogleNet | KNN | 93.90 | 92.49 | 95.23 | 95.10 | 7.51 | 4.77 | 94.0 | 87.76 | 93.78 |
| Dataset | LR-PCA | Feature Extractor | Classification Model | Acc. | SE | SP | PRE | FNR | FPR | AUC | MCC | F1-Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Grayscale images | Across all classes | AlexNet | Ensemble (subspace KNN) | 97.50 | 99.42 | 96.38 | 96.41 | 0.58 | 3.62 | 100 | 95.81 | 97.89 |
| VGG16 | Ensemble (subspace KNN) | 97.30 | 97.49 | 97.30 | 97.30 | 2.51 | 2.70 | 100 | 94.79 | 97.40 | ||
| GoogleNet | Ensemble (subspace KNN) | 97.50 | 97.47 | 95.98 | 95.98 | 2.53 | 4.02 | 100 | 93.45 | 96.72 | ||
| Pseudo-Colored images | AlexNet | Ensemble (subspace KNN) | 98.60 | 99.41 | 97.49 | 97.54 | 0.39 | 2.51 | 100 | 97.13 | 98.57 | |
| VGG16 | Ensemble (subspace KNN) | 98.20 | 98.26 | 98.07 | 98.07 | 1.74 | 1.93 | 100 | 96.33 | 98.17 | ||
| GoogleNet | Ensemble (subspace KNN) | 97.50 | 97.88 | 97.10 | 97.13 | 2.12 | 2.90 | 100 | 94.98 | 97.50 | ||
| Grayscale images | For each class separately | AlexNet | Ensemble (subspace KNN) | 98.10 | 98.65 | 97.49 | 97.51 | 1.35 | 2.51 | 100 | 96.14 | 98.08 |
| VGG16 | Ensemble (subspace KNN) | 97.00 | 98.07 | 96.53 | 96.58 | 1.93 | 3.47 | 100 | 94.61 | 97.32 | ||
| GoogleNet | Ensemble (subspace KNN) | 96.30 | 96.35 | 96.71 | 96.72 | 3.65 | 3.29 | 99.0 | 93.05 | 96.53 | ||
| Pseudo-Colored images | AlexNet | Ensemble (subspace KNN) | 98.80 | 99.62 | 98.26 | 98.28 | 0.58 | 1.74 | 100 | 97.69 | 98.85 | |
| VGG16 | Ensemble (subspace KNN) | 97.70 | 98.46 | 96.91 | 96.96 | 1.54 | 3.09 | 99.0 | 95.38 | 97.70 | ||
| GoogleNet | Ensemble (subspace KNN) | 97.30 | 97.30 | 97.30 | 97.30 | 2.70 | 2.70 | 0.99 | 94.59 | 97.30 | ||
| Grayscale images | Not applied | AlexNet | KNN | 97.00 | 98.65 | 96.91 | 96.97 | 1.35 | 3.09 | 96.0 | 95.57 | 97.80 |
| VGG16 | KNN | 97.80 | 97.88 | 97.68 | 97.69 | 2.12 | 2.32 | 100 | 95.56 | 97.78 | ||
| GoogleNet | KNN | 97.80 | 97.68 | 97.88 | 97.87 | 2.32 | 2.12 | 98.0 | 95.56 | 97.78 | ||
| Pseudo-Colored | AlexNet | KNN | 97.20 | 97.90 | 96.93 | 96.97 | 2.10 | 3.07 | 95.0 | 94.83 | 97.43 | |
| VGG16 | KNN | 97.60 | 97.87 | 97.88 | 97.87 | 2.13 | 2.12 | 100 | 0.9575 | 0.9787 | ||
| GoogleNet | KNN | 97.90 | 97.67 | 97.50 | 97.49 | 2.33 | 2.50 | 99.0 | 0.9517 | 0.9758 |
| Reference | Feature Extraction Approach | Classifier | Dataset | SE (%) | Acc. (%) |
|---|---|---|---|---|---|
| Oliver et al. [78] | Utilizing Fuzzy C Means for lesion segmentation and a number of textural and morphological features are used | SVM | MIAS | 87.33 | 91.51 |
| Phadke et al. [77] | Breast cancer classification based on the fusion of local and global morphological and textural features | SVM | MIAS | 92.71 | 83.1 |
| Jian et al. [75] | Utilizing the wavelet transform in order to retrieve the textural features of ROIs | Classification of ROIs using SVM | MIAS | 96.3 | 97.7 |
| Vijayarajeswari et al. [76] | Breast lesions were classified using SVM after applying the Hough transform for feature extraction. | SVM | MIAS | - | 94.0 |
| Xie et al. [74] | Classification of breast lesions using metaheuristic-based classifier | PSO-SVM | MIAS | 92.0 | 89.0 |
| Mina et al. [73] | Classification of breast cancer using ANN and wavelet decomposition for feature extraction | ANN | MIAS | 68.0 | - |
| Liu et al. [72] | Detection of microcalcification in digital mammograms | SVM | INbreast | 92.0 | - |
| Xu et al. [79] | Deep CNN for feature extraction and classification of breast lesions | CNN | INbreast | - | 96.8 |
| Al-antari et al. [63,82] | End-to-end CAD system for the segmentation and classification of breast masses | YOLO classifier | INbreast | 95.64 | 89.91 |
| Ragab et al. [29] | Deep features fusion of AlexNet, GoogleNet, ResNet-18, ResNet-50, and ResNet-10. | SVM | CBIS-DDSM MIAS | 98.0 99.0 | 97.90 97.40 |
| Alhussan et al. [16] | AlexNet | AlexNet | MIAS | 98.26 | 98.26 |
| GoogLeNet | GoogLeNet | 98.26 | 98.26 | ||
| VGG-16 | VGG-16 | 98.70 | 98.28 | ||
| Zhang et al. [81] | Features were extracted by Gist, SIFT, HOG, LBP, VGG, ResNet, and DenseNet and fused together. | SVM, XGBoost, Naïve Bayes, k-NN, DT, AdaBoosting | CBIS-DDSM INbreast | 98.61 57.2 | 90.91 87.93 |
| Song et al. [83] | GoogleNet Inception-v2 | XGBoost | DDSM | 99.74 | 92.8 |
| Khan et al. [80] | Fusion of deep features extracted by VGG-16, VGG-19, GoogleNet, and ResNet-50. | Transfer Learning | CBIS-DDSM MIAS | 98.07 | 96.6 |
| Proposed CAD system | Features are selected using LR-PCA from pseudo images. | Hybrid Transfer Learning of CNN-based LR-PCA | MIAS INbreast | 99.62 98.28 | 98.80 98.62 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samee, N.A.; Alhussan, A.A.; Ghoneim, V.F.; Atteia, G.; Alkanhel, R.; Al-antari, M.A.; Kadah, Y.M. A Hybrid Deep Transfer Learning of CNN-Based LR-PCA for Breast Lesion Diagnosis via Medical Breast Mammograms. Sensors 2022, 22, 4938. https://doi.org/10.3390/s22134938
Samee NA, Alhussan AA, Ghoneim VF, Atteia G, Alkanhel R, Al-antari MA, Kadah YM. A Hybrid Deep Transfer Learning of CNN-Based LR-PCA for Breast Lesion Diagnosis via Medical Breast Mammograms. Sensors. 2022; 22(13):4938. https://doi.org/10.3390/s22134938
Chicago/Turabian StyleSamee, Nagwan Abdel, Amel A. Alhussan, Vidan Fathi Ghoneim, Ghada Atteia, Reem Alkanhel, Mugahed A. Al-antari, and Yasser M. Kadah. 2022. "A Hybrid Deep Transfer Learning of CNN-Based LR-PCA for Breast Lesion Diagnosis via Medical Breast Mammograms" Sensors 22, no. 13: 4938. https://doi.org/10.3390/s22134938