
Tunable White Light for Elders (TWLITE): A Protocol Demonstrating Feasibility and Acceptability for Deployment, Remote Data Collection, and Analysis of a Home-Based Lighting Intervention in Older Adults

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Lighting Protocol
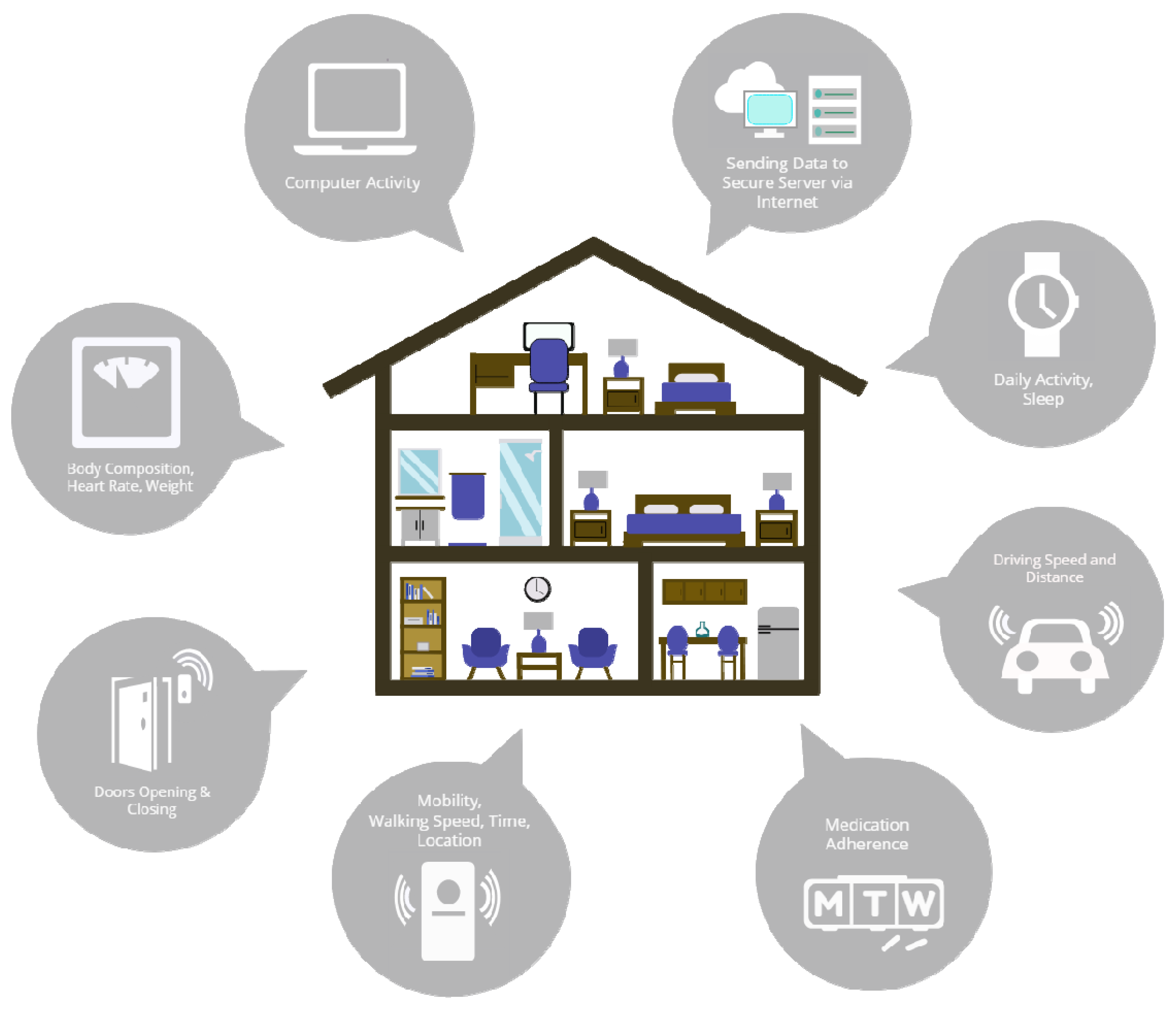
2.2. Passive Infrared Motion Sensors
2.3. Sleep
2.4. Actigraphy
3. Results
3.1. Demographics
3.2. Feasibility and Acceptability
3.3. Home Floorplans
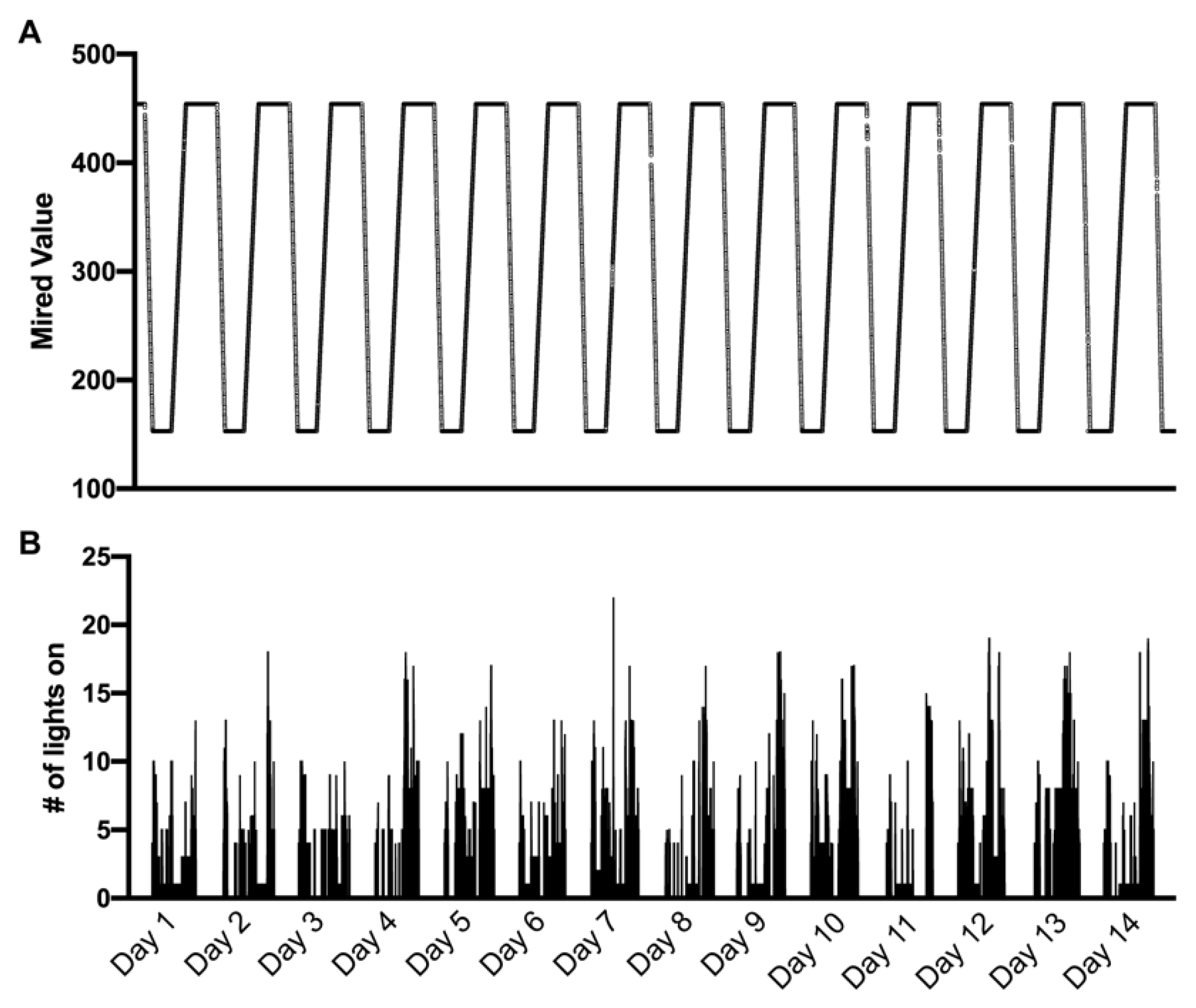
3.4. Mired Values and Light State
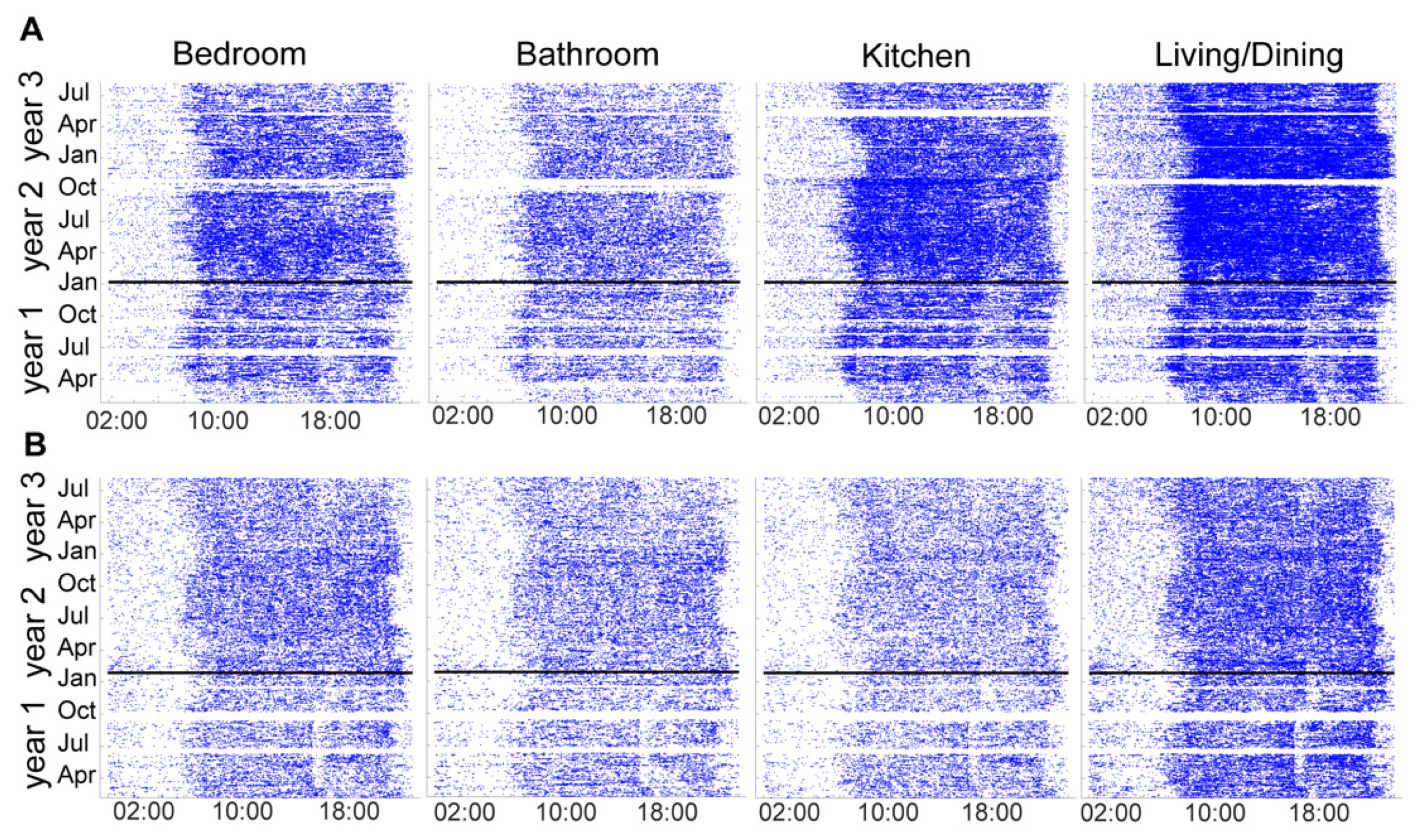
3.5. Passive Infrared Motion Sensors
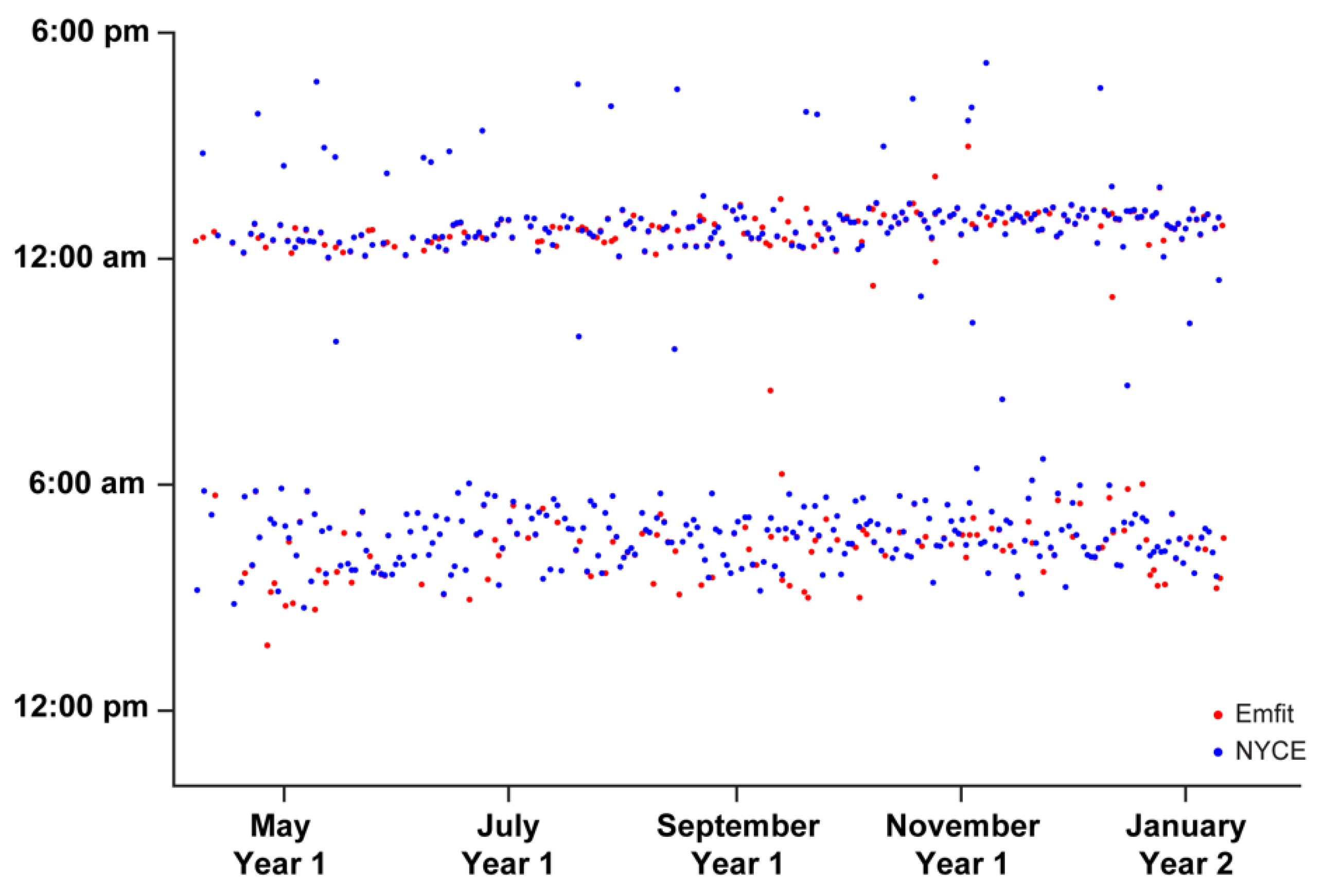
3.6. Sleep
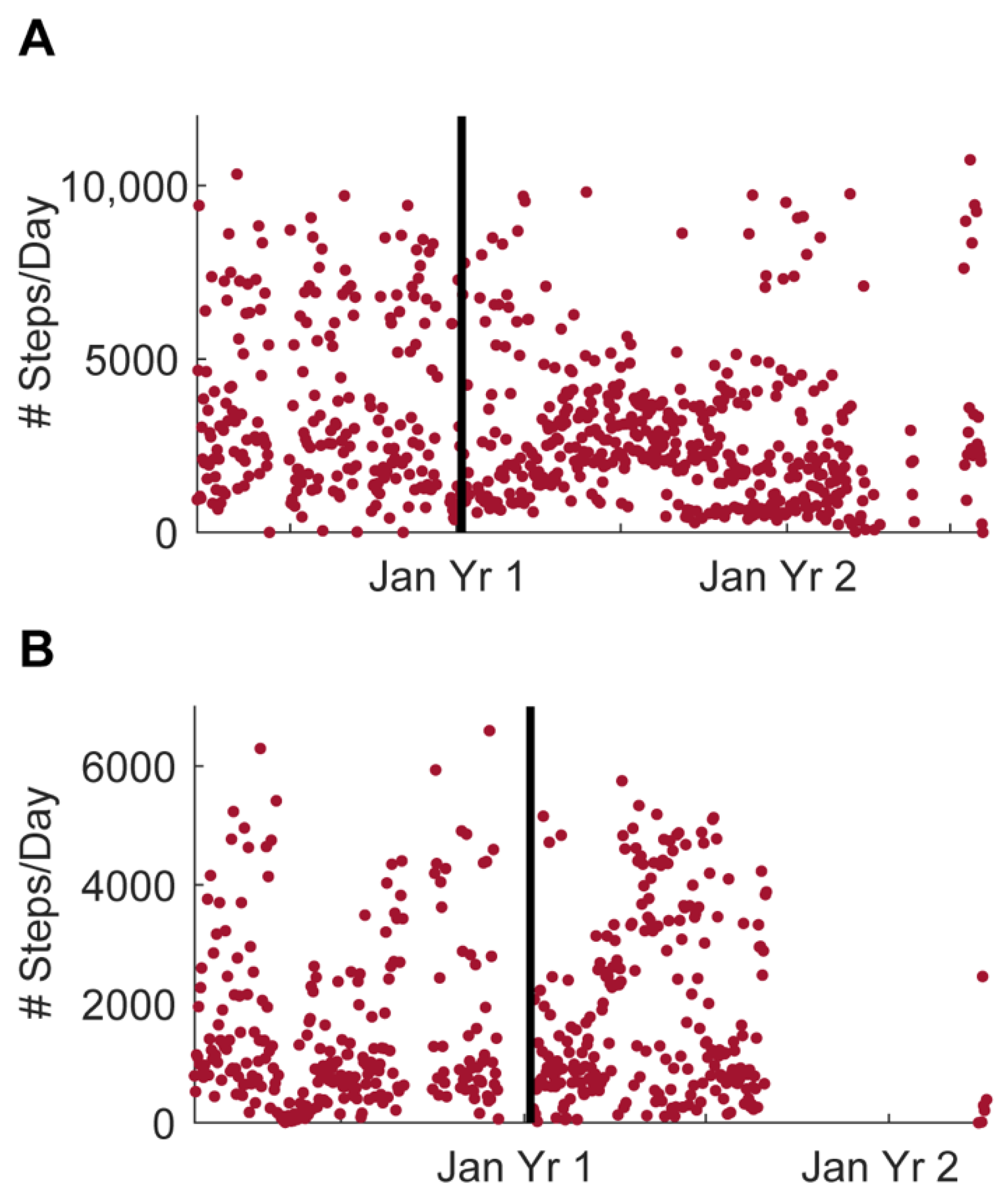
3.7. Physical Activity (Steps)
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Beaulieu-Bonneau, S.; Hudon, C. Sleep disturbances in older adults with mild cognitive impairment. Int. Psychogeriatr. 2009, 21, 654–666. [Google Scholar] [CrossRef] [PubMed]
- Bonanni, E.; Maestri, M.; Tognoni, G.; Fabbrini, M.; Nucciarone, B.; Manca, M.L.; Gori, S.; Iudice, A.; Murri, L. Daytime sleepiness in mild and moderate Alzheimer’s disease and its relationship with cognitive impairment. J. Sleep Res. 2005, 14, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Craig, D.; Hart, D.J.; Passmore, A.P. Genetically increased risk of sleep disruption in Alzheimer’s disease. SLEEP 2006, 29, 1003–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moran, M.; Lynch, C.A.; Walsh, C.; Coen, R.; Coakley, D.; Lawlor, B.A. Sleep disturbance in mild to moderate Alzheimer’s disease. Sleep Med. 2005, 6, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Bachman, D.; Rabins, P. “Sundowning” and other temporally associated agitation states in dementia patients. Annu. Rev. Med. 2006, 57, 499–511. [Google Scholar] [CrossRef] [Green Version]
- Guarnieri, B.; Adorni, F.; Musicco, M.; Appollonio, I.; Bonanni, E.; Caffarra, P.; Caltagirone, C.; Cerroni, G.; Concari, L.; Cosentino, F.I.; et al. Prevalence of sleep disturbances in mild cognitive impairment and dementing disorders: A multicenter Italian clinical cross-sectional study on 431 patients. Dement. Geriatr. Cogn. Disord. 2012, 33, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Ju, Y.E.; Lucey, B.P.; Holtzman, D.M. Sleep and Alzheimer disease pathology—A bidirectional relationship. Nat. Rev. Neurol. 2014, 10, 115–119. [Google Scholar] [CrossRef]
- Bombois, S.; Derambure, P.; Pasquier, F.; Monaca, C. Sleep disorders in aging and dementia. J. Nutr. Health Aging 2010, 14, 212–217. [Google Scholar] [CrossRef]
- Casement, M.D.; Broussard, J.L.; Mullington, J.M.; Press, D.Z. The contribution of sleep to improvements in working memory scanning speed: A study of prolonged sleep restriction. Biol. Psychol. 2006, 72, 208–212. [Google Scholar] [CrossRef] [Green Version]
- Graves, L.A.; Heller, E.A.; Pack, A.I.; Abel, T. Sleep deprivation selectively impairs memory consolidation for contextual fear conditioning. Learn. Mem. 2003, 10, 168–176. [Google Scholar] [CrossRef] [Green Version]
- Prince, T.M.; Wimmer, M.; Choi, J.; Havekes, R.; Aton, S.; Abel, T. Sleep deprivation during a specific 3-hour time window post-training impairs hippocampal synaptic plasticity and memory. Neurobiol. Learn. Mem. 2014, 109, 122–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holth, J.K.; Fritschi, S.K.; Wang, C.; Pedersen, N.P.; Cirrito, J.R.; Mahan, T.E.; Finn, M.B.; Manis, M.; Geerling, J.C.; Fuller, P.M.; et al. The sleep-wake cycle regulates brain interstitial fluid tau in mice and CSF tau in humans. Science 2019, 363, 880–884. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.E.; Lim, M.M.; Bateman, R.J.; Lee, J.J.; Smyth, L.P.; Cirrito, J.R.; Fujiki, N.; Nishino, S.; Holtzman, D.M. Amyloid-beta dynamics are regulated by orexin and the sleep-wake cycle. Science 2009, 326, 1005–1007. [Google Scholar] [CrossRef] [Green Version]
- Iliff, J.J.; Chen, M.J.; Plog, B.A.; Zeppenfeld, D.M.; Soltero, M.; Yang, L.; Singh, I.; Deane, R.; Nedergaard, M. Impairment of Glymphatic Pathway Function Promotes Tau Pathology after Traumatic Brain Injury. J. Neurosci. 2014, 34, 16180–16193. [Google Scholar] [CrossRef] [Green Version]
- Xie, L.; Kang, H.K.; Xu, Q.; Chen, M.J.; Liao, Y.; Thiyagarajan, M.; O’Donnell, J.; Christensen, D.J.; Nicholson, C.; Iliff, J.J.; et al. Sleep drives metabolite clearance from the adult brain. Science 2013, 342, 373–377. [Google Scholar] [CrossRef] [Green Version]
- Irish, L.A.; Kline, C.E.; Gunn, H.E.; Buysse, D.J.; Hall, M.H. The role of sleep hygiene in promoting public health: A review of empirical evidence. Sleep Med. Rev. 2015, 22, 23–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCrae, C.S.; Dzierzewski, J.M.; Kay, D. Treatment of Late-life Insomnia. Sleep Med. Clin. 2009, 4, 593–604. [Google Scholar] [CrossRef] [Green Version]
- Collier, J.; Durmus, D.; Davis, R. Lighting in Senior Care Centers: Comparing Tunable LED Systems to Conventional Lighting Systems in Four Senior Care Centers; Pacific Northwest National Lab. (PNNL): Richland, WA, USA, 2021. [Google Scholar] [CrossRef]
- De Lepeleire, J.; Bouwen, A.; De Coninck, L.; Buntinx, F. Insufficient lighting in nursing homes. J. Am. Med. Dir. Assoc. 2007, 8, 314–317. [Google Scholar] [CrossRef]
- Masri, S.; Sassone-Corsi, P. The circadian clock: A framework linking metabolism, epigenetics and neuronal function. Nat. Rev. Neurosci. 2013, 14, 69–75. [Google Scholar] [CrossRef] [Green Version]
- Lockley, S.W.; Gooley, J.J. Circadian Photoreception: Spotlight on the Brain. Curr. Biol. 2006, 16, 795–797. [Google Scholar] [CrossRef] [Green Version]
- Duffy, J.F.; Czeisler, C.A. Effect of Light on Human Circadian Physiology. Sleep Med. Clin. 2009, 4, 165–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, K.; Van Someren, E.J.W.; Shea, S.A.; Scheer, F.A.J.L. Reduction of scale invariance of activity fluctuations with aging and Alzheimer’s disease: Involvement of the circadian pacemaker. Proc. Natl. Acad. Sci. USA 2009, 106, 2490–2494. [Google Scholar] [CrossRef] [Green Version]
- Witting, W.; Mirmiran, M.; Bos, N.P.; Swaab, D.F. Effect of light intensity on diurnal sleep-wake distribution in young and old rats. Brain Res. Bull. 1993, 30, 157–162. [Google Scholar] [CrossRef] [Green Version]
- Van Someren, E.J.W.; Riemersma, R.F.; Swaab, D.F. Functional plasticity of the circadian timing system in old age: Light exposure. Prog. Brain Res. 2002, 138, 205–231. [Google Scholar] [CrossRef] [PubMed]
- Giménez, M.C.; Kanis, M.J.; Beersma, D.G.M.; van der Pol, B.A.E.; van Norren, D.; Gordijn, M.C.M. In vivo quantification of the retinal reflectance spectral composition in elderly subjects before and after cataract surgery: Implications for the non-visual effects of light. J. Biol. Rhythms. 2010, 25, 123–131. [Google Scholar] [CrossRef] [Green Version]
- Turner, P.L.; Van Someren, E.J.W.; Mainster, M.A. The role of environmental light in sleep and health: Effects of ocular aging and cataract surgery. Sleep Med. Rev. 2010, 14, 269–280. [Google Scholar] [CrossRef]
- Hu, K.; Riemersma-van der Lek, R.F.; Patxot, M.; Li, P.; Shea, S.A.; Scheer, F.A.J.L.; Van Someren, E.J.W. Progression of Dementia Assessed by Temporal Correlations of Physical Activity: Results From a 3.5-Year, Longitudinal Randomized Controlled Trial. Sci. Rep. 2016, 6, 27742. [Google Scholar] [CrossRef]
- Royer, M.; Ballentine, N.H.; Eslinger, P.J.; Houser, K.; Mistrick, R.; Behr, R.; Rakos, K. Light therapy for seniors in long term care. J. Am. Med. Dir. Assoc. 2012, 13, 100–102. [Google Scholar] [CrossRef]
- Hattar, S.; Liao, H.W.; Takao, M.; Berson, D.M.; Yau, K.W. Melanopsin-containing retinal ganglion cells: Architecture, projections, and intrinsic photosensitivity. Science 2002, 295, 1065–1070. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, S.; Morgan, P.L.; Schlangen, L.J.M.; Williams, P.; Skene, D.J.; Middleton, B. Blue-Enriched Lighting for Older People Living in Care Homes: Effect on Activity, Actigraphic Sleep, Mood and Alertness. Curr. Alzheimer Res. 2017, 14, 1053–1062. [Google Scholar] [CrossRef]
- Pilorz, V.; Tam, S.K.; Hughes, S.; Pothecary, C.A.; Jagannath, A.; Hankins, M.W.; Bannerman, D.M.; Lightman, S.L.; Vyazovskiy, V.V.; Nolan, P.M.; et al. Melanopsin Regulates Both Sleep-Promoting and Arousal-Promoting Responses to Light. PLoS Biol. 2016, 14, e1002482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raikes, A.C.; Killgore, W.D.S. Potential for the development of light therapies in mild traumatic brain injury. Concussion 2018, 3, CNC57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Maanen, A.; Meijer, A.M.; van der Heijden, K.B.; Oort, F.J. The effects of light therapy on sleep problems: A systematic review and meta-analysis. Sleep Med. Rev. 2016, 29, 52–62. [Google Scholar] [CrossRef]
- Figueiro, M.G. Light, sleep and circadian rhythms in older adults with Alzheimer’s disease and related dementias. Neurodegener. Dis. Manag. 2017, 7, 119–145. [Google Scholar] [CrossRef] [Green Version]
- Elliott, J.E.; McBride, A.A.; Balba, N.M.; Thomas, S.V.; Pattinson, C.L.; Morasco, B.J.; Wilkerson, A.; Gill, J.M.; Lim, M.M. Feasibility and preliminary efficacy for morning bright light therapy to improve sleep and plasma biomarkers in US Veterans with TBI. A prospective, open-label, single-arm trial. PLoS ONE 2022, 17, e0262955. [Google Scholar] [CrossRef] [PubMed]
- Baier, R.R.; McCreedy, E.; Uth, R.; Gifford, D.R.; Wetle, T. Nursing home leaders’ perceptions of a research partnership. Aging Clin. Exp. Res. 2021, 33, 3371–3377. [Google Scholar] [CrossRef]
- Sekiguchi, H.; Iritani, S.; Fujita, K. Bright light therapy for sleep disturbance in dementia is most effective for mild to moderate Alzheimer’s type dementia: A case series. Psychogeriatrics 2017, 17, 275–281. [Google Scholar] [CrossRef]
- Van Der Ploeg, E.S.; O’Connor, D.W. Methodological challenges in studies of bright light therapy to treat sleep disorders in nursing home residents with dementia. Psychiatry Clin. Neurosci. 2014, 68, 777–784. [Google Scholar] [CrossRef] [Green Version]
- Connolly, L.J.; Ponsford, J.L.; Rajaratnam, S.M.W.; Lockley, S.W. Development of a Home-Based Light Therapy for Fatigue Following Traumatic Brain Injury: Two Case Studies. Front. Neurol. 2021, 12, 651498. [Google Scholar] [CrossRef]
- Beattie, Z.; Miller, L.M.; Almirola, C.; Au-Yeung, W.-T.M.; Bernard, H.; Cosgrove, K.E.; Dodge, H.H.; Gamboa, C.J.; Golonka, O.; Gothard, S.; et al. The Collaborative Aging Research Using Technology Initiative: An Open, Sharable, Technology-Agnostic Platform for the Research Community. Digit. Biomark. 2020, 4, 100–118. [Google Scholar] [CrossRef]
- Wu, C.-Y.; Dodge, H.H.; Gothard, S.; Mattek, N.; Wright, K.; Barnes, L.L.; Silbert, L.C.; Lim, M.M.; Kaye, J.A.; Beattie, Z. Unobtrusive Sensing Technology Detects Ecologically Valid Spatiotemporal Patterns of Daily Routines Distinctive to Persons with Mild Cognitive Impairment. J. Gerontol. A Biol. Sci. Med. Sci. 2021. [Google Scholar] [CrossRef] [PubMed]
- Kaye, J.; Reynolds, C.; Bowman, M.; Sharma, N.; Riley, T.; Golonka, O.; Lee, J.; Quinn, C.; Beattie, Z.; Austin, J.; et al. Methodology for Establishing a Community-Wide Life Laboratory for Capturing Unobtrusive and Continuous Remote Activity and Health Data. J. Vis. Exp. 2018, 137, e56942. [Google Scholar] [CrossRef] [PubMed]
- Piantino, J.; Luther, M.; Reynolds, C.; Lim, M.M. Emfit Bed Sensor Activity Shows Strong Agreement with Wrist Actigraphy for the Assessment of Sleep in the Home Setting. Nat. Sci. Sleep 2021, 13, 1157–1166. [Google Scholar] [CrossRef]
- Kaye, J.; Beattie, Z.; Sharma, N.; Riley, T.; Silbert, L.; Barnes, L.; Czaja, S.; Dodge, H. Collaborative aging research using technology: New pathways forward. Innov. Aging 2019, 3, S832. [Google Scholar] [CrossRef]
- Thomas, N.W.D.; Lindauer, A.; Kaye, J. EVALUATE-AD and Tele-STAR: Novel Methodologies for Assessment of Caregiver Burden in a Telehealth Caregiver Intervention—A Case Study. Dement. Geriatr. Cogn. Disord. 2019, 47, 176–184. [Google Scholar] [CrossRef]
- Au-Yeung, W.-T.M.; Kaye, J.A.; Beattie, Z. Step Count Standardization: Validation of Step Counts from the Withings Activite using PiezoRxD and wGT3X-BT. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine & Biology Society, Montreal, QC, Canada, 20–24 July 2020; pp. 4608–4611. [Google Scholar] [CrossRef]
- Reynolds, C.; Lim, M.M.; Mattek, N.; Dodge, H.; Kaye, J.A. Disrupted infradian rhythms in mild cognitive impairment. Alzheimer’s Assoc. Int. Conf. 2017, 13, 368–639. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Successes |
|
|
|
| Challenges |
|
|
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elliott, J.E.; Tinsley, C.E.; Reynolds, C.; Olson, R.J.; Weymann, K.B.; Au-Yeung, W.-T.M.; Wilkerson, A.; Kaye, J.A.; Lim, M.M. Tunable White Light for Elders (TWLITE): A Protocol Demonstrating Feasibility and Acceptability for Deployment, Remote Data Collection, and Analysis of a Home-Based Lighting Intervention in Older Adults. Sensors 2022, 22, 5372. https://doi.org/10.3390/s22145372
Elliott JE, Tinsley CE, Reynolds C, Olson RJ, Weymann KB, Au-Yeung W-TM, Wilkerson A, Kaye JA, Lim MM. Tunable White Light for Elders (TWLITE): A Protocol Demonstrating Feasibility and Acceptability for Deployment, Remote Data Collection, and Analysis of a Home-Based Lighting Intervention in Older Adults. Sensors. 2022; 22(14):5372. https://doi.org/10.3390/s22145372
Chicago/Turabian StyleElliott, Jonathan E., Carolyn E. Tinsley, Christina Reynolds, Randall J. Olson, Kristianna B. Weymann, Wan-Tai M. Au-Yeung, Andrea Wilkerson, Jeffrey A. Kaye, and Miranda M. Lim. 2022. "Tunable White Light for Elders (TWLITE): A Protocol Demonstrating Feasibility and Acceptability for Deployment, Remote Data Collection, and Analysis of a Home-Based Lighting Intervention in Older Adults" Sensors 22, no. 14: 5372. https://doi.org/10.3390/s22145372