
Effect of a Passive Exosuit on Sit-to-Stand Performance in Geriatric Patients Measured by Body-Worn Sensors—A Pilot Study
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Design
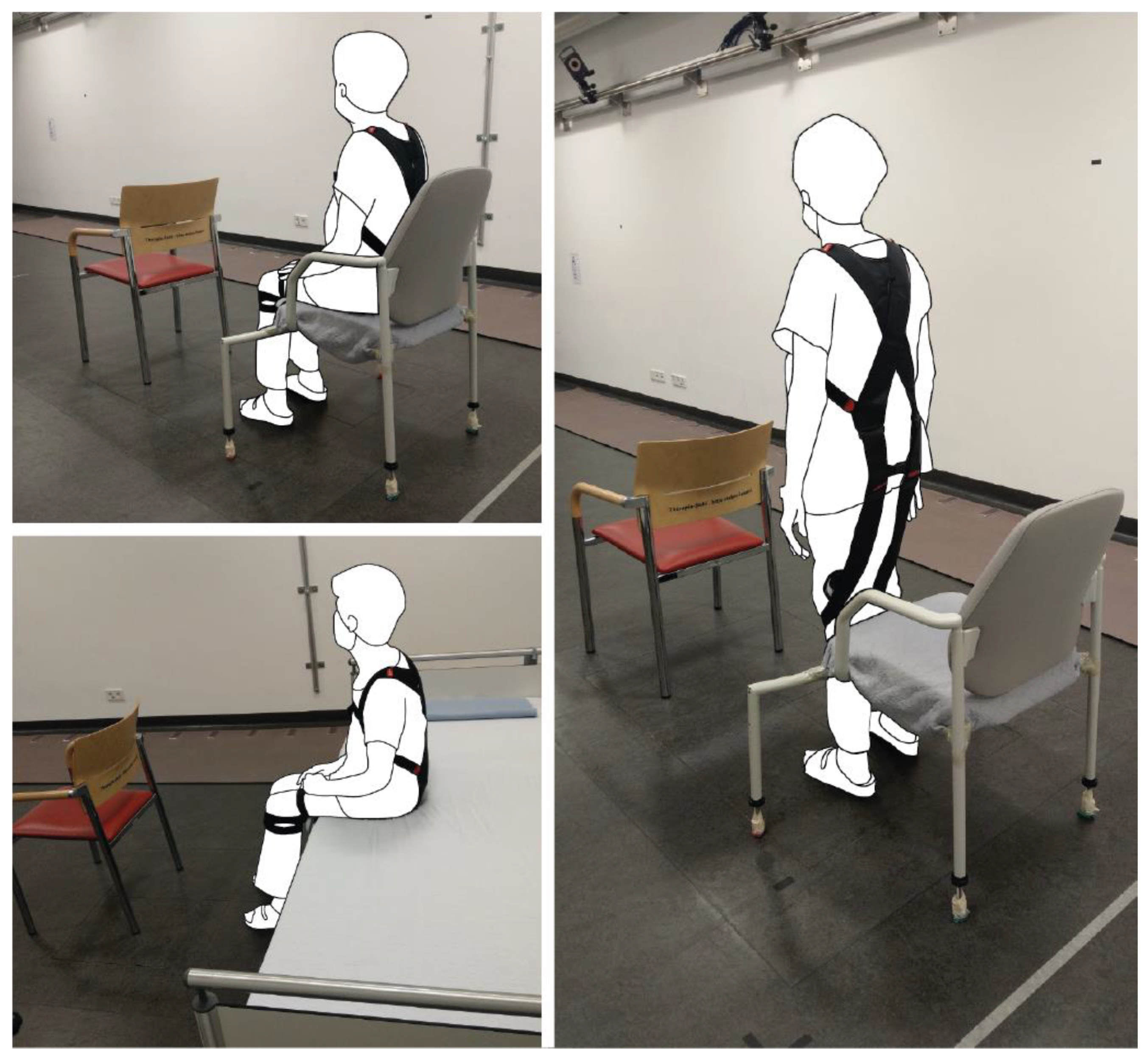
2.2. Protocol and Outcome Parameters
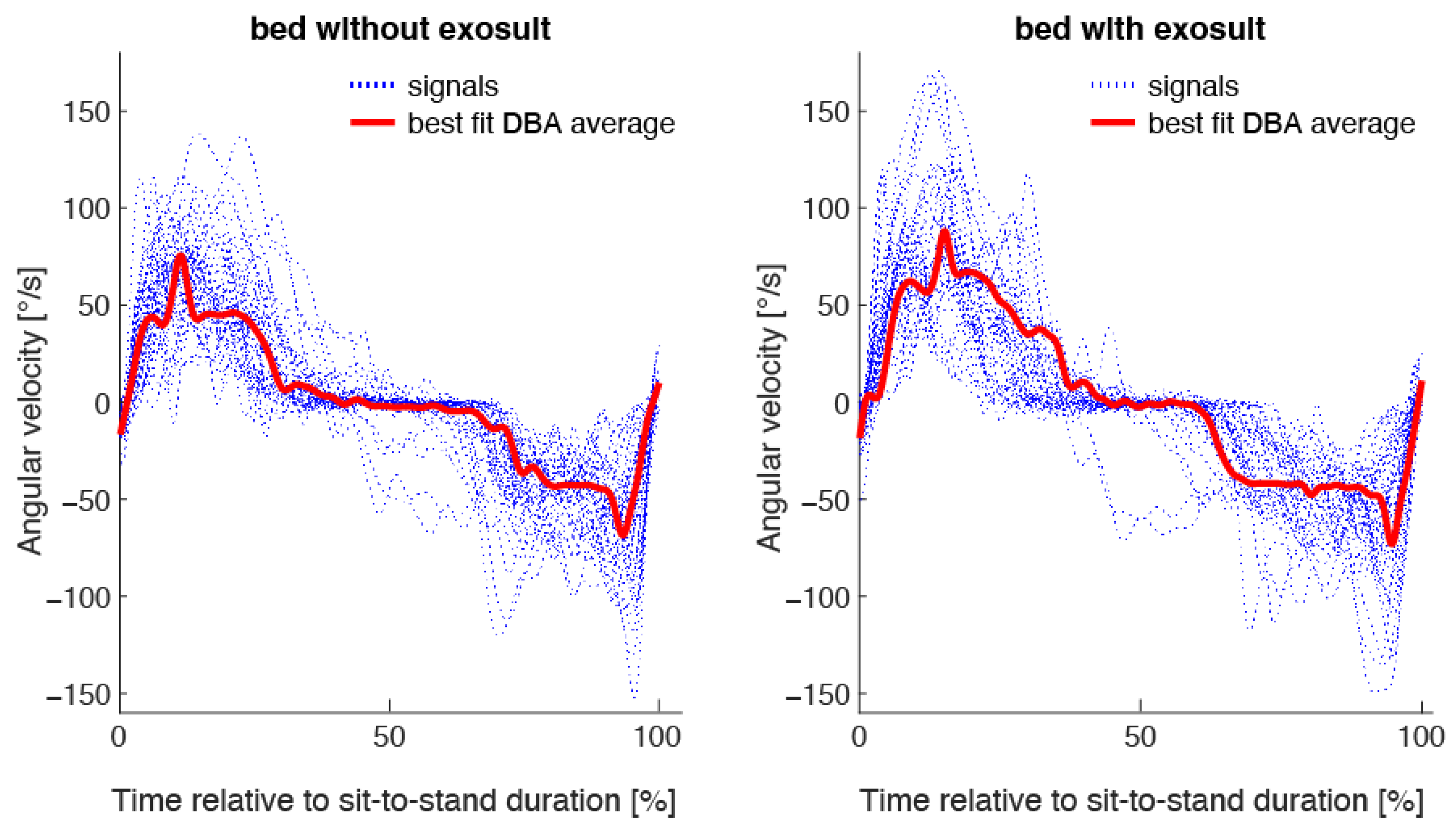
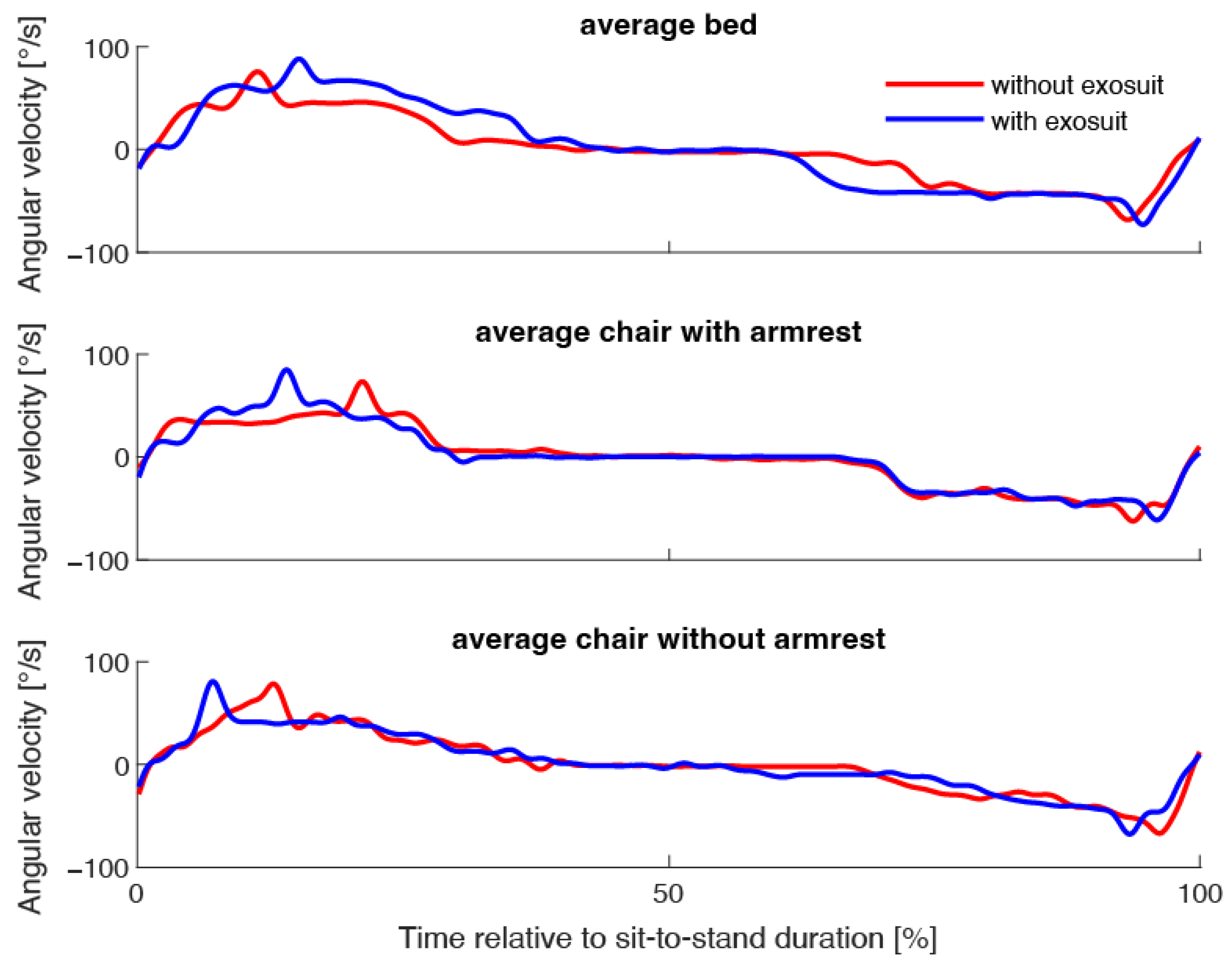
2.3. Outcome Measure
2.4. Descriptive Measures
2.5. Statistics
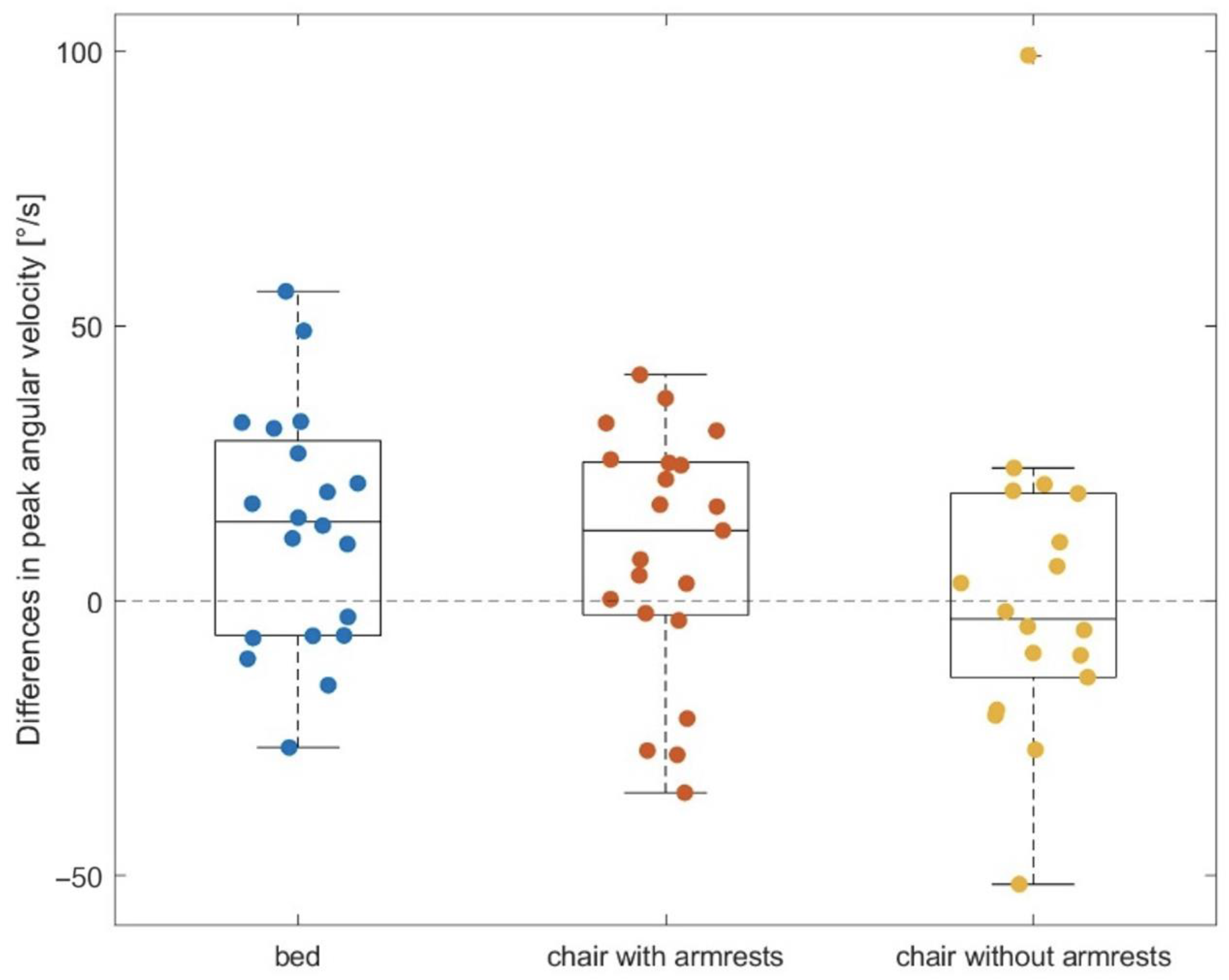
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chamberlain, M.A.; Munton, J. Designing chairs for the disabled arthritic. Br. J. Rheumatol. 1984, 23, 304–308. [Google Scholar] [CrossRef] [PubMed]
- Alcazar, J.; Alegre, L.M.; Van Roie, E.; Magalhães, J.P.; Nielsen, B.R.; González-Gross, M.; Júdice, P.B.; Casajús, J.A.; Delecluse, C.; Sardinha, L.B.; et al. Relative sit-to-stand power: Aging trajectories, functionally relevant cut-off points, and normative data in a large European cohort. J. Cachexia Sarcopenia Muscle 2021, 12, 921–932. [Google Scholar] [CrossRef] [PubMed]
- Rapp, K.; Becker, C.; Cameron, I.D.; König, H.-H.; Büchele, G. Epidemiology of Falls in Residential Aged Care: Analysis of More Than 70,000 Falls From Residents of Bavarian Nursing Homes. J. Am. Med. Dir. Assoc. 2012, 13, 187.e1–187.e6. [Google Scholar] [CrossRef] [PubMed]
- Ejupi, A.; Brodie, M.; Gschwind, Y.J.; Lord, S.R.; Zagler, W.L.; Delbaere, K. Kinect-Based Five-Times-Sit-to-Stand Test for Clinical and In-Home Assessment of Fall Risk in Older People. Gerontology 2015, 62, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Bao, W.; Sun, Y.; Zhang, T.; Zou, L.; Wu, X.; Wang, D.; Chen, Z. Exercise Programs for Muscle Mass, Muscle Strength and Physical Performance in Older Adults with Sarcopenia: A Systematic Review and Meta-Analysis. Aging Dis. 2020, 11, 863–873. [Google Scholar] [CrossRef]
- de Labra, C.; Guimaraes-Pinheiro, C.; Maseda, A.; Lorenzo, T.; Millán-Calenti, J.C. Effects of physical exercise interventions in frail older adults: A systematic review of randomized controlled trials. BMC Geriatr. 2015, 15, 154. [Google Scholar] [CrossRef] [Green Version]
- Becker, C.; Kron, M.; Lindemann, U.; Sturm, E.; Eichner, B.; Walter-Jung, B.; Nikolaus, T. Effectiveness of a Multifaceted Intervention on Falls in Nursing Home Residents. J. Am. Geriatr. Soc. 2003, 51, 306–313. [Google Scholar] [CrossRef] [Green Version]
- Sherrington, C.; Tiedemann, A.; Fairhall, N.J.; Hopewell, S.; Michaleff, Z.A.; Howard, K.; Clemson, L.; Lamb, S.E. Exercise for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2019, 1, CD012424. [Google Scholar] [CrossRef]
- Janssen, W.G.; Bussmann, H.B.; Stam, H.J. Determinants of the sit-to-stand movement: A review. Phys. Ther. 2002, 82, 866–879. [Google Scholar] [CrossRef]
- Rodríguez-Fernández, A.; Lobo-Prat, J.; Font-Llagunes, J.M. Systematic review on wearable lower-limb exoskeletons for gait training in neuromuscular impairments. J. Neuroeng. Rehabil. 2021, 18, 22. [Google Scholar] [CrossRef]
- Quinlivan, B.T.; Lee, S.; Malcolm, P.; Rossi, D.M.; Grimmer, M.; Siviy, C.; Karavas, N.; Wagner, D.; Asbeck, A.; Galiana, I.; et al. Assistance magnitude versus metabolic cost reductions for a tethered multiarticular soft exosuit. Sci. Robot. 2017, 2, eaah4416. [Google Scholar] [CrossRef] [PubMed]
- Zanotto, D.; Akiyama, Y.; Stegall, P.; Agrawal, S.K. Knee Joint Misalignment in Exoskeletons for the Lower Extremities: Effects on User’s Gait. IEEE Trans. Robot. 2015, 31, 978–987. [Google Scholar] [CrossRef]
- Lee, H.; Kim, S.H.; Park, H.-S. A Fully Soft and Passive Assistive Device to Lower the Metabolic Cost of Sit-to-Stand. Front. Bioeng. Biotechnol. 2020, 8, 966. [Google Scholar] [CrossRef] [PubMed]
- Daub, U.; Budaker, B.; Schneider, U. Assistive technologies for workers in the automotive industry. In Internationales Stuttgarter Symposium; Bargende, M., Reuss, H.C., Wiedemann, J., Eds.; Springer Fachmedien: Wiesbaden, Germany, 2015; pp. 899–908. [Google Scholar]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A Short Physical Performance Battery Assessing Lower Extremity Function: Association With Self-Reported Disability and Prediction of Mortality and Nursing Home Admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- Schenkman, M.; Riley, P.; Pieper, C. Sit to stand from progressively lower seat heights—Alterations in angular velocity. Clin. Biomech. Bristol Avon. 1996, 11, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.M.; Hester, G.M.; Ha, P.L.; Olmos, A.A.; Stratton, M.T.; VanDusseldorp, T.A.; Feito, Y.; Dalton, B.E. Sit-to-Stand Kinetics and Correlates of Performance in Young and Older Males. Arch. Gerontol. Geriatr. 2020, 91, 104215. [Google Scholar] [CrossRef]
- Zijlstra, W.; Aminian, K. Mobility assessment in older people: New possibilities and challenges. Eur. J. Ageing 2007, 4, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Klenk, J.; Ba, A.; Sczuka, K.S.; Daub, U.; Lindemann, U. Assessment of Thigh Angular Velocity by an Activity Monitor to Describe Sit-to-Stand Performance. Sensors 2022, 22, 1405. [Google Scholar] [CrossRef] [PubMed]
- Pickford, C.G.; Findlow, A.H.; Kerr, A.; Banger, M.; Clarke-Cornwell, A.M.; Hollands, K.L.; Quinn, T.; Granat, M.H. Quantifying sit-to-stand and stand-to-sit transitions in free-living environments using the activPAL thigh-worn activity monitor. Gait Posture 2019, 73, 140–146. [Google Scholar] [CrossRef]
- Brooke, J. SUS: A “quick and dirty” usability scale. In Usability Evaluation in Industry; Jordan, P.W., Thomas, B., Weerdmeester, B.A., McClelland, A.L., Eds.; Taylor & Francs: London, UK, 1996; pp. 189–194. [Google Scholar]
- Groll, D.L.; To, T.; Bombardier, C.; Wright, J.G. The development of a comorbidity index with physical function as the outcome. J. Clin. Epidemiol. 2005, 58, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Katzman, R.; Brown, T.; Fuld, P.; Peck, A.; Schechter, R.; Schimmel, H. Validation of a short Orientation-Memory-Concentration Test of cognitive impairment. Am. J. Psychiatry 1983, 140, 734–739. [Google Scholar]
- Lindemann, U. Spatiotemporal gait analysis of older persons in clinical practice and research: Which parameters are relevant? Z Gerontol. Geriatr. 2020, 53, 171–178. [Google Scholar] [CrossRef]
- Petitjean, F.; Ketterlin, A.; Gançarski, P. A global averaging method for dynamic time warping, with applications to clustering. Pattern Recognit. 2011, 44, 678–693. [Google Scholar] [CrossRef]
- Sakoe, H.; Chiba, S. Dynamic programming algorithm optimization for spoken word recognition. IEEE Trans. Acoust. Speech Signal Process. 1978, 26, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Shokoohi-Yekta, M.; Hu, B.; Jin, H.; Wang, J.; Keogh, E. Generalizing DTW to the multi-dimensional case requires an adaptive approach. Data Min. Knowl. Discov. 2017, 31, 1–31. [Google Scholar] [CrossRef] [Green Version]
- Sczuka, K.; Schneider, M.; Bourke, A.; Mellone, S.; Kerse, N.; Helbostad, J.; Becker, C.; Klenk, J. Template-Based Recognition of Human Locomotion in IMU Sensor Data Using Dynamic Time Warping. Sensors 2021, 21, 2601. [Google Scholar] [CrossRef]
- Hirschfeld, H.; Thorsteinsdottir, M.; Olsson, E. Coordinated ground forces exerted by buttocks and feet are adequately programmed for weight transfer during sit-to-stand. J. Neurophysiol. 1999, 82, 3021–3029. [Google Scholar] [CrossRef] [PubMed]
- Yandell, M.B.; Ziemnicki, D.M.; McDonald, K.A.; Zelik, K.E. Characterizing the comfort limits of forces applied to the shoulders, thigh and shank to inform exosuit design. PLoS ONE 2020, 15, e0228536. [Google Scholar] [CrossRef]
- Guillén-Climent, S.; Garzo, A.; Muñoz-Alcaraz, M.N.; Casado-Adam, P.; Arcas-Ruiz-Ruano, J.; Mejías-Ruiz, M.; Mayordomo-Riera, F.J. A usability study in patients with stroke using MERLIN, a robotic system based on serious games for upper limb rehabilitation in the home setting. J. Neuroeng. Rehabil. 2021, 18, 41. [Google Scholar] [CrossRef]
- Ito, K.; Uehara, S.; Yuasa, A.; Kim, C.M.; Kitamura, S.; Ushizawa, K.; Tanabe, S.; Otaka, Y. Electromyography-controlled gamified exercise system for the distal upper extremity: A usability assessment in subacute post-stroke patients. Disabil. Rehabil. Assist. Technol. 2021, 6, 1–6. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Median (1.–3.Q) | Minimum–Maximum | |
|---|---|---|
| Age (years) | 82 (79–84) | 64–92 |
| Body weight (kg) | 71.0 (60.0–87.0) | 40.5–104.0 |
| Body height (m) | 1.66 (1.62–1.76) | 1.45–1.90 |
| Comorbidity index (0–18) | 3 (3–4) | 2–6 |
| Cognition (0–25) | 4 (2–6.5) | 0–12 |
| Habitual gait speed (m/s) | 0.70 (0.51–0.79) | 0.41–1.17 |
| Maximum handgrip strength (kg) | 20.0 (17.8–29.6) | 14.4–51.0 |
| Peak Angular Velocity (°/s) While Standing Up from … | Median (1.–3.Q) | Min–Max | p |
|---|---|---|---|
| bed with push off without exosuit * | 79.7 (74.6–98.2) | 56.0–140.2 | 0.014 |
| bed with push off with exosuit * | 92.6 (84.3–116.2) | 50.6–164.6 | |
| chair using armrests without exosuit | 77.8 (59.3–100.7) | 31.5–160.6 | 0.089 |
| chair using armrests with exosuit | 92.9 (78.3–113.0) | 29.3–163.2 | |
| chair without using armrests without exosuit ** | 86.8 (68.8–114.3) | 35.4–147.4 | 0.966 |
| chair without using armrests with exosuit ** | 83.7 (73.4–112.4) | 33.5–204.8 |
| Differences in Peak Angular Velocity with and without Exosuit Support When … | Gait Speed | Hand Grip Strength |
|---|---|---|
| standing up from bed with pushing off | r = 0.33 | r = 0.07 |
| standing up from chair using armrests | r = 0.02 | r = 0.31 |
| standing up from chair without using armrests | r = −0.13 | r = −0.38 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lindemann, U.; Krespach, J.; Daub, U.; Schneider, M.; Sczuka, K.S.; Klenk, J. Effect of a Passive Exosuit on Sit-to-Stand Performance in Geriatric Patients Measured by Body-Worn Sensors—A Pilot Study. Sensors 2023, 23, 1032. https://doi.org/10.3390/s23021032
Lindemann U, Krespach J, Daub U, Schneider M, Sczuka KS, Klenk J. Effect of a Passive Exosuit on Sit-to-Stand Performance in Geriatric Patients Measured by Body-Worn Sensors—A Pilot Study. Sensors. 2023; 23(2):1032. https://doi.org/10.3390/s23021032
Chicago/Turabian StyleLindemann, Ulrich, Jana Krespach, Urban Daub, Marc Schneider, Kim S. Sczuka, and Jochen Klenk. 2023. "Effect of a Passive Exosuit on Sit-to-Stand Performance in Geriatric Patients Measured by Body-Worn Sensors—A Pilot Study" Sensors 23, no. 2: 1032. https://doi.org/10.3390/s23021032