
Electromyographic Activity of the Pelvic Floor Muscles and Internal Oblique Muscles in Women during Running with Traditional and Minimalist Shoes: A Cross-Over Clinical Trial

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Sample Size Calculation
2.4. Instrumentation
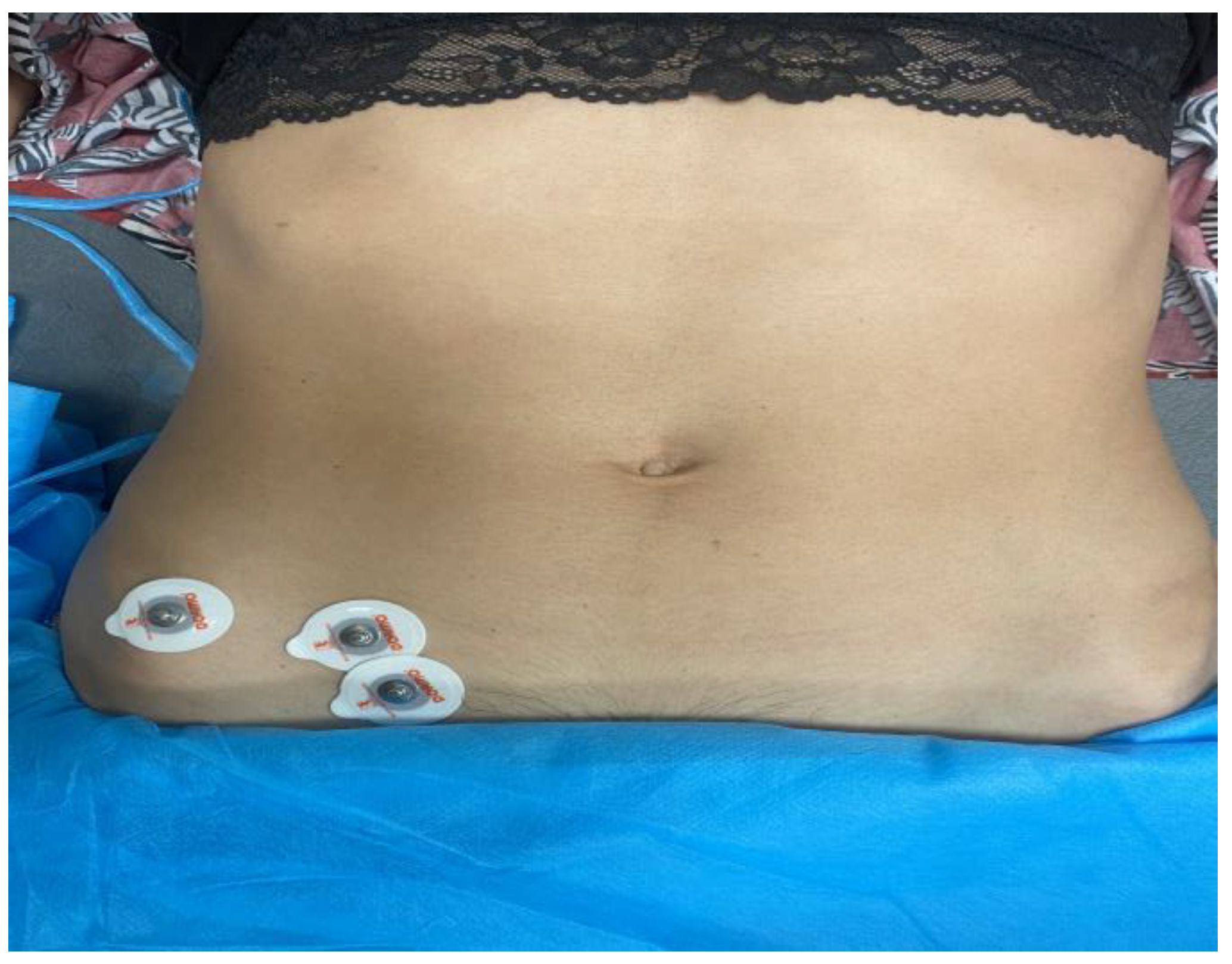
2.5. Procedures
2.6. Data Reduction
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chisholm, L.; Delpe, S.; Priest, T.; Reynolds, W.S. Physical Activity and Stress Incontinence in Women. Curr. Bl. Dysfunct. Rep. 2019, 14, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Rogers, R.G.; Pauls, R.N.; Thakar, R.; Morin, M.; Kuhn, A.; Petri, E.; Fatton, B.; Whitmore, K.; Kinsberg, S.; Lee, J. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for the assessment of sexual health of women with pelvic floor dysfunction. Neurourol. Urodyn. 2018, 37, 1220–1240. [Google Scholar] [CrossRef] [PubMed]
- Rubilotta, E.; Balzarro, M.; D’amico, A.; Cerruto, M.A.; Bassi, S.; Bovo, C.; Iacovelli, V.; Bianchi, D.; Artibani, W.; Agrò, E.F. Pure stress urinary incontinence: Analysis of prevalence, estimation of costs, and financial impact. BMC Urol. 2019, 19, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagovska, M.; Svihra, J.; Bukova, A.; Horbacz, A.; Svihrova, V. The impact of physical activity measured by the International Physical Activity questionnaire on the prevalence of stress urinary incontinence in young women. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 228, 308–312. [Google Scholar] [CrossRef]
- Leitner, M.; Moser, H.; Eichelberger, P.; Kuhn, A.; Radlinger, L. Evaluation of pelvic floor muscle activity during running in continent and incontinent women: An exploratory study. Neurourol. Urodyn. 2017, 36, 1570–1576. [Google Scholar] [CrossRef]
- Neumann, P.; Gill, V. Pelvic Floor and Abdominal Muscle Interaction: EMG Activity and Intra-abdominal Pressure. Int. Urogynecol. J. 2002, 13, 125–132. [Google Scholar] [CrossRef]
- Goldish, G.D.; Quast, J.E.; Blow, J.J.; Kuskowski, M.A. Postural effects on intra-abdominal pressure during Valsalva maneuver. Arch. Phys. Med. Rehabil. 1994, 75, 324–327. [Google Scholar] [CrossRef]
- Tajiri, K.; Huo, M.; Maruyama, H. Effects of Co-contraction of Both Transverse Abdominal Muscle and Pelvic Floor Muscle Exercises for Stress Urinary Incontinence: A Randomized Controlled Trial. J. Phys. Ther. Sci. 2014, 26, 1161–1163. [Google Scholar] [CrossRef] [Green Version]
- Hollander, K.; Liebl, D.; Meining, S.; Mattes, K.; Willwacher, S.; Zech, A. Adaptation of Running Biomechanics to Repeated Barefoot Running: A Randomized Controlled Study. Am. J. Sports Med. 2019, 47, 1975–1983. [Google Scholar] [CrossRef]
- Lieberman, D.E.; Castillo, E.R.; Otárola-Castillo, E.; Sang, M.K.; Sigei, T.K.; Ojiambo, R.; Okutoyi, P.; Pitsiladis, Y. Variation in Foot Strike Patterns among Habitually Barefoot and Shod Runners in Kenya. PLoS ONE 2015, 10, e0131354. [Google Scholar] [CrossRef]
- Davis, I.S.; Rice, H.M.; Wearing, S.C. Why forefoot striking in minimal shoes might positively change the course of running injuries. J. Sport Health Sci. 2017, 6, 154–161. [Google Scholar] [CrossRef] [Green Version]
- Perkins, K.P.; Hanney, W.J.; Rothschild, C.E. The Risks and Benefits of Running Barefoot or in Minimalist Shoes. Sports Health A Multidiscip. Approach 2014, 6, 475–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillinov, S.M.; Laux, S.; Kuivila, T.; Hass, D.; Joy, S.M. Effect of Minimalist Footwear on Running Efficiency: A Randomized Crossover Trial. Sports Health A Multidiscip. Approach 2015, 7, 256–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azevedo, A.P.D.S.; Mezêncio, B.; Amadio, A.C.; Serrão, J.C. 16 Weeks of Progressive Barefoot Running Training Changes Impact Force and Muscle Activation in Habitual Shod Runners. PLoS ONE 2016, 11, e0167234. [Google Scholar] [CrossRef] [Green Version]
- Esculier, J.-F.; Dubois, B.; Dionne, C.E.; Leblond, J.; Roy, J.-S. A consensus definition and rating scale for minimalist shoes. J. Foot Ankle Res. 2015, 8, 42. [Google Scholar] [CrossRef] [Green Version]
- Campitelli, N.A.; Spencer, S.A.; Bernhard, K.; Heard, K.; Kidon, A. Effect of Vibram FiveFingers Minimalist Shoes on the Abductor Hallucis Muscle. J. Am. Podiatr. Med. Assoc. 2016, 106, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Robbins, S.E.; Hanna, A.M. Running-related injury prevention through barefoot adaptations. Med. Sci. Sports Exerc. 1987, 19, 148–156. [Google Scholar] [CrossRef]
- Yang, Y.; Zhang, X.; Luo, Z.; Wang, X.; Ye, D.; Fu, W. Alterations in Running Biomechanics after 12 Week Gait Retraining with Minimalist Shoes. Int. J. Environ. Res. Public Heal. 2020, 17, 818. [Google Scholar] [CrossRef] [Green Version]
- Bonacci, J.; Vicenzino, B.; Spratford, W.; Collins, P. Take your shoes off to reduce patellofemoral joint stress during running. Br. J. Sports Med. 2014, 48, 425–428. [Google Scholar] [CrossRef]
- Grier, T.; Canham-Chervak, M.; Bushman, T.; Anderson, M.; North, W.; Jones, B.H. Minimalist Running Shoes and Injury Risk Among United States Army Soldiers. Am. J. Sports Med. 2016, 44, 1439–1446. [Google Scholar] [CrossRef]
- Goldstick, O.; Constantini, N. Urinary incontinence in physically active women and female athletes. Br. J. Sports Med. 2014, 48, 296–298. [Google Scholar] [CrossRef]
- Nygaard, I.; Shaw, J.; Egger, M.J. Exploring the association between lifetime physical activity and pelvic floor disorders: Study and design challenges. Contemp. Clin. Trials 2012, 33, 819–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carls, C. The prevalence of stress urinary incontinence in high school and college-age female athletes in the midwest: Implica-tions for education and prevention. Urol. Nurs. 2007, 27, 21. [Google Scholar] [PubMed]
- Almeida, M.B.A.; Barra, A.A.; Saltiel, F.; Silva-Filho, A.L.; Fonseca, A.M.R.M.; Figueiredo, E.M. Urinary incontinence and other pelvic floor dysfunctions in female athletes in Brazil: A cross-sectional study. Scand. J. Med. Sci. Sports 2016, 26, 1109–1116. [Google Scholar] [CrossRef] [PubMed]
- Nygaard, I.E.; Glowacki, C.; Saltzman, C.L. Relationship between foot flexibility and urinary incontinence in nulliparous varsity athletes. Obstet. Gynecol. 1996, 87, 1049–1051. [Google Scholar] [CrossRef] [PubMed]
- García-Arrabe, M.; García-Fernández, P.; Ruiz-Ruiz, B.; del Prado-Álvarez, R.; Romero-Morales, C.; Díaz-Arribas, M.J. Effects of minimalist shoes on pelvic floor activity in nulliparous women during running at different velocities: A randomized cross-over clinical trial. Sci. Rep. 2022, 12, 21218. [Google Scholar] [CrossRef]
- Brinkman, H.; Yanchek, A.; Thorton, E. Barefoot Training: Effect on Lateral Pelvic Drop and EMG Activity of Gluteus Medius and TFL. Ph.D. Thesis, University of North Dakota, Grand Forks, ND, USA, 2018. [Google Scholar]
- Yang, C.; Xiao, S.; Yang, Y.; Zhang, X.; Wang, J.; Fu, W. Patellofemoral Joint Loads during Running Immediately Changed by Shoes with Different Minimalist Indices: A Cross-sectional Study. Appl. Sci. 2019, 9, 4176. [Google Scholar] [CrossRef] [Green Version]
- Wakeling, J.M.; Pascual, S.A.; Nigg, B.M. Altering muscle activity in the lower extremities by running with different shoes. Med. Sci. Sports Exerc. 2002, 34, 1529–1532. [Google Scholar] [CrossRef]
- Vigotsky, A.D.; Halperin, I.; Lehman, G.J.; Trajano, G.; Vieira, T.M.; Vigotsky, A.D.; Halperin, I.; Lehman, G.J.; Trajano, G.; Vieira, T.M. Interpreting Signal Amplitudes in Surface Electromyography Studies in Sport and Rehabilitation Sciences. Front. Physiol. 2018, 8, 985. [Google Scholar] [CrossRef] [Green Version]
- Schlink, B.R.; Nordin, A.D.; Ferris, D.P. Human myoelectric spatial patterns differ among lower limb muscles and locomotion speeds. Physiol. Rep. 2020, 8, e14652. [Google Scholar] [CrossRef]
- Nordander, C.; Willner, J.; Hansson, G.-A.; Larsson, B.; Unge, J.; Granquist, L.; Skerfving, S. Influence of the subcutaneous fat layer, as measured by ultrasound, skinfold calipers and BMI, on the EMG amplitude. Eur. J. Appl. Physiol. 2003, 89, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Luginbuehl, H.; Naeff, R.; Zahnd, A.; Baeyens, J.-P.; Kuhn, A.; Radlinger, L. Pelvic floor muscle electromyography during different running speeds: An exploratory and reliability study. Arch. Gynecol. Obstet. 2016, 293, 117–124. [Google Scholar] [CrossRef]
- Snijders, C.J.; Ribbers, M.T.; de Bakker, H.V.; Stoeckart, R.; Stam, H.J. EMG recordings of abdominal and back muscles in various standing postures: Validation of a biomechanical model on sacroiliac joint stability. J. Electromyogr. Kinesiol. 1998, 8, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Leitner, M.; Moser, H.; Eichelberger, P.; Kuhn, A.; Baeyens, J.-P.; Radlinger, L. Evaluation of pelvic floor kinematics in continent and incontinent women during running: An exploratory study. Neurourol. Urodyn. 2018, 37, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Luginbuehl, H.; Greter, C.; Gruenenfelder, D.; Baeyens, J.-P.; Kuhn, A.; Radlinger, L. Intra-session test–retest reliability of pelvic floor muscle electromyography during running. Int. Urogynecol. J. 2013, 24, 1515–1522. [Google Scholar] [CrossRef] [Green Version]
- Oakford, R.; Moses, L.E. Tables of Random Permutations. In Applied Statistics; Stanford University Press: Redwood City, CA, USA, 1963; Volume 12, p. 196. [Google Scholar]
- Hopkins, W.; Marshall, S.; Batterham, A.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3. [Google Scholar] [CrossRef] [Green Version]
- Lucas-Cuevas, A.G.; Quesada, J.I.P.; Giménez, J.V.; Aparicio, I.; Jimenez-Perez, I.; Pérez-Soriano, P. Initiating running barefoot: Effects on muscle activation and impact accelerations in habitually rearfoot shod runners. Eur. J. Sport Sci. 2016, 16, 1145–1152. [Google Scholar] [CrossRef]
- Cooper, D.M.; Leissring, S.K.; Kernozek, T.W. Plantar loading and foot-strike pattern changes with speed during barefoot running in those with a natural rearfoot strike pattern while shod. Foot 2015, 25, 89–96. [Google Scholar] [CrossRef]
- Perl, D.P.; Daoud, A.I.; Lieberman, D.E. Effects of Footwear and Strike Type on Running Economy. Med. Sci. Sports Exerc. 2012, 44, 1335–1343. [Google Scholar] [CrossRef] [Green Version]
- Jacome, C.; Oliveira, D.; Marques, A.; Sá Couto, P. Prevalence and impact of urinary incontinence among female athletes. Int. J. Gynecol. Obs. 2011, 114, 60–63. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Variable Geometry EMG Sensor | Fixed Geometry EMG Sensor |
|---|---|---|
| Weight | 5 g | 5 g |
| Measurements | 8 × 37 × 21 mm | 7 × 27 × 19 mm |
| Distance between electrodes | Variable | 12 mm |
| Electrode composition | Single use | Ag or Ag-AgCl |
| Differential amplification | 990 v/v ± 0.2% | 990 v/v ± 0.2% |
| Common mode rejection coefficient | >113 dB | >113 dB |
| Input impedance | >1.1 GΩ | >1.1 GΩ |
| Output impedance | <100 Ω | <100 Ω |
| Lower cutoff frequency | 20 Hz | 20 Hz |
| Upper cutoff frequency | 20.3 kHz | 20.3 kHz |
| Equivalent input noise | <22 nV/Hz | <22 nV/Hz |
| Supply voltage | Of ± 2 V ± 6 V | Of ± 2 V ± 6 V |
| Absorbed current | ±865 µA | ±865 µA |
| Mean ± SD | Range (min–max) | |
|---|---|---|
| Age | 27.1 ± 5.3 | 20–36 |
| Weight | 64.9 ± 1.4 | 58–80 |
| Height | 168 ± 5.1 | 165–180 |
| BMI | 22.8 ± 2.5 | 20.0–28.3 |
| EMG Variables | Minimalist Shoes n = 10 | Traditional Shoes n = 10 | Mean Difference (95%CI) | p-Value (ES) | |
|---|---|---|---|---|---|
| IO | work average (µV) | 14.6 ± 6.9 | 15.6 ± 8.2 | −1.0 (−6.0;8.0) | 0.21 (0.10) |
| % of MVC | 16.7 ± 10.8 | 21.2 ± 10.1 | −4.4 (0.03;8.9) | 0.04 (0.77) | |
| PFM | work average (µV) | 31.7 ± 10.4 | 31.9 ± 9.8 | −0.2 (−3.9;4.4) | 0.33 (0.04) |
| % of MVC | 36.3 ± 4.8 | 34.7 ± 4.5 | 1.6 (−6.0;8.0) | 0.23 (0.50) |
| Muscles | Variables | Height | p | Weight | p | Age | p | |
|---|---|---|---|---|---|---|---|---|
| IO | Traditional Shoes | work average (µV) | 0.08 | 0.81 | −0.8 | 0.8 | −0.64 * | 0.046 |
| % of MVC | 0.62 | 0.07 | −0.2 | 0.52 | −0.25 | 0.84 | ||
| Minimalist Shoes | work average (µV) | 0.61 | 0.06 | 0.12 | 0.73 | −0.04 | 0.24 | |
| % of MVC | 0.49 | 0.17 | −0.05 | 0.88 | −0.41 | 0.27 | ||
| PFMs | Traditional Shoes | work average (µV) | −0.23 | 0.51 | 0.18 | 0.61 | 0.28 | 0.43 |
| % of MVC | −0.34 | 0.36 | −0.48 | 0.18 | 0.01 | 0.9 | ||
| Minimalist Shoes | work average (µV) | −0.19 | 0.59 | −0.03 | 0.92 | 0.53 | 0.11 | |
| % of MVC | −0.38 | 0.3 | 0.07 | 0.84 | 0.08 | 0.98 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Arrabé, M.; García-Fernandez, P.; Díaz-Arribas, M.J.; López-Marcos, J.J.; González-de-la-Flor, Á.; Estrada-Barranco, C.; Roy, J.-S. Electromyographic Activity of the Pelvic Floor Muscles and Internal Oblique Muscles in Women during Running with Traditional and Minimalist Shoes: A Cross-Over Clinical Trial. Sensors 2023, 23, 6496. https://doi.org/10.3390/s23146496
García-Arrabé M, García-Fernandez P, Díaz-Arribas MJ, López-Marcos JJ, González-de-la-Flor Á, Estrada-Barranco C, Roy J-S. Electromyographic Activity of the Pelvic Floor Muscles and Internal Oblique Muscles in Women during Running with Traditional and Minimalist Shoes: A Cross-Over Clinical Trial. Sensors. 2023; 23(14):6496. https://doi.org/10.3390/s23146496
Chicago/Turabian StyleGarcía-Arrabé, María, Pablo García-Fernandez, María José Díaz-Arribas, Jose Javier López-Marcos, Ángel González-de-la-Flor, Cecilia Estrada-Barranco, and Jean-Sébastien Roy. 2023. "Electromyographic Activity of the Pelvic Floor Muscles and Internal Oblique Muscles in Women during Running with Traditional and Minimalist Shoes: A Cross-Over Clinical Trial" Sensors 23, no. 14: 6496. https://doi.org/10.3390/s23146496