
Cleaning in Times of Pandemic: Perceptions of COVID-19 Risks among Workers in Facility Services
by
 ,
,
Isabel Dias
1,*, 
Alexandra Lopes
2 ,
,
José Azevedo
3,
Ana Sofia Maia
3 and
João Santos Baptista
4,* 1
Institute of Sociology of the University of Porto, Faculty of Arts and Humanities, University of Porto, 4150-564 Porto, Portugal
2
Centre for English, Translation and Anglo-American Studies (CETAPS), Faculty of Arts and Humanities, University of Porto, 4150-564 Porto, Portugal
3
Faculty of Arts and Humanities, University of Porto, 4150-564 Porto, Portugal
4
Associated Laboratory for Energy, Transports and Aeronautics (PROA/LAETA), Faculty of Engineering, University of Porto, 4200-465 Porto, Portugal
*
Authors to whom correspondence should be addressed.
Soc. Sci. 2022, 11(7), 276; https://doi.org/10.3390/socsci11070276
Submission received: 30 April 2022
/
Revised: 18 June 2022
/
Accepted: 21 June 2022
/
Published: 27 June 2022
(This article belongs to the Topic Research and Innovation Practices: Cooperation and Collaborations in Scientific and Entrepreneurial Contexts)
Abstract
:Cleaning services are a transversal activity that guarantees the proper functioning and conditions of safety, hygiene, and health across all economic sectors. The COVID-19 pandemic increased the need for clean, sanitary spaces, particularly in health services and other areas with a large number of people. The workers in these services were often placed on the frontline without any specific training or information. Their low average schooling aggravated this situation. Therefore, exploring these workers’ perceptions about the COVID-19 pandemic and its potential influence on their mental health was the primary goal of our research. Structured interviews were conducted based on questionnaires in a sample of 436 women. Their characterisation focused on three aspects related to the pandemic. First, to prevent infecting others (85.5%) and that people close to them could die (86.0%) were the dominant concerns; second, the feeling of permanent vigilance was mentioned (56.2%); and third, the fear of not getting medical care (60.7%). Thus, the workers felt there was a need for more dissemination of individual protection measures, as well as more training, better general working conditions, and access to psychological counselling.
Keywords:
cleaners; cleaning services; confinement; mental health; health conditions; coronavirus; SARS-COV-21. Introduction
Regardless of the industrial or service sector, whether public or private, all have some kind of cleaning activities in common. They guarantee basic hygiene and the quality of living and working conditions.
As an independent, specialised service, the cleaning sector began to grow at the end of the Second World War. However, the sector experienced significant expansion in the mid-1960s due to the abundant supply of labour and its low initial investment (Scandella 2010). Currently, according to the European Cleaning and Installation Services Industry (EFCI) Federation (EFCI 2020), the sector employs more than 4.2 million people in more than 297,000 companies in Europe (NACE code 81.2: “cleaning activities”). In Portugal, according to the INE (INE 2021), in 2020, this sector of activity housed 9393 companies, having experienced rapid growth; employed 90,103 workers; and had a turnover of more than 1.3 thousand million EUR. In Europe, the sector is dominated by companies with nine or fewer employees (EFCI 2020; INE 2021). However, this growth was accompanied by structural changes in the cleaning industry, such as increased competition, the disappearance of permanent jobs, privatisation, and segmentation, leading to different impacts on employers and workers in this sector (Ollus 2016).
The International Labor Organization (ILO) classifies these workers among the most vulnerable groups (ILO-Lisbon 2020). The COVID-19 pandemic aggravated this situation, increasing the cleaning workers’ direct exposure to harmful agents (Sun et al. 2020). The awareness of their exposure to risks and the danger to their close relatives significantly added to their level of stress (Pfefferbaum and North 2020). This situation was further aggravated by the social disqualification of this activity (Rodrigues et al. 2013).
Given the cleaning sector’s fast pace and excess workload, workers do not have time for adequate training (Suleiman and Svendsen 2015). In addition to low levels of schooling, this partly explains why there are so many work accidents and work-related illnesses in this sector (Parra-Tapia et al. 2019). Therefore, how little we know about the reality of cleaning workers is surprising, as well as the lack of academic interest in this professional category, which is largely neglected in scientific research (Luz et al. 2017).
In this sector, relations between workers and employers are more precarious than in most others. Outsourcing aggravates the precariousness of the cleaning companies concerning the enterprises for which they provide services. This means that the workers do not work on their employer’s premises, further legitimising precarious forms of employment (Bondy 2018). At the same time, there has been increased pressure on working conditions, heightening the profession’s socially disqualified image (Brugière 2017). A service that is provided before or after “regular” working hours, usually under subcontracting schemes, removes the “cleaning” factor from companies and makes hygiene and cleaning even more invisible (De Gasparo et al. 2018). Thus, if work is invisible, its value also becomes invisible from an economic point of view (Hughes 1997; Lhuilier 2005; De Gasparo et al. 2018).
In addition to chemical risks (Nan et al. 2021; Ruokolainen et al. 2022), these workers face other risks that cannot be ignored, particularly ergonomic risks (Naik and Khan 2020; Gonçalves and de Oliveira Sato 2020), health risks (Taş et al. 2021; Furuya et al. 2022), and psychosocial risks (Soo-Jeong et al. 2021; Unge et al. 2007).
Given the global context described above, this study aimed to assess the impacts of COVID-19 among female cleaning service workers, both in terms of their perceptions about the pandemic and the potential implications for their mental health. The goal was to contribute to the emerging literature on the impacts of COVID-19 by focusing on a specific professional group that was critical for the implementation of infection containment protocols (e.g., disinfection and sanitation). However, they did not benefit from the public visibility and appreciation that other professional groups experienced, namely, healthcare workers. The study used scales other researchers have already validated to measure these effects. The research focused on the perceptions of female cleaning service workers to identify the factors that heightened their worries and anxiety. The article also discusses the driving forces behind increased anxiety regarding COVID-19.
In summary, the article discusses the factors leading to increased anxiety about COVID-19, showing a link between cleaning workers’ performance during the pandemic and increased anxiety levels and worsening mental health. Several recommendations are also proposed to decrease the levels of anxiety experienced by female cleaners during the pandemic, improve their mental health levels, and increase safety at work.
2. Literature Review
The facility services industry, in particular, cleaning services, was one of the economic sectors in high demand during the pandemic to cope with the sanitary requirements. Due to its labour-intensive characteristics, it employs a large number of workers, mainly women.
The facility services sector increasingly provides a diverse range of services. However, its main activities are largely associated with cleaning activities inside buildings, building maintenance, gardening, sanitation, and pest control.
In terms of its main characteristics, the service is performed at the client’s premises; the allocated workforce has an employment contract associated with a workplace and not with an enterprise (Bondy 2018; Eurofund 2014). The workplace may be occasional, in which workers belong to different service teams, or it may be habitual, resulting in a fixed workplace at the customer’s premises (Larsen et al. 2019). The complexity of the cleaning service provided varies, ranging from domestic households to hospital surgical blocks (EFCI 2020; Marconato et al. 2017).
However, there is no professional recognition of this sector’s workers or their tasks’ importance (Brugière 2017). The majority earn minimum wage, and the working hours are generally outside the company’s business hours, which implies working at night and/or early morning, as well as maintaining services, even at minimal levels, on festive dates and holidays (Eurofund 2014; Larsen et al. 2019).
Labour dynamics and worker well-being have long raised the interest of the social sciences and other disciplinary areas, particularly occupational and public health. Facility services, more specifically, cleaning activities, are often addressed in studies dedicated to occupational diseases, i.e., diseases caused by work-related factors. These diseases are generally contracted when workers are exposed to chemical, physical, and biological agents above the legal limits without the appropriate protection (Castro et al. 2019; Gonçalves and de Oliveira Sato 2020; Taş et al. 2021).
Other risks arise from, for example, repetitive physical movements, extreme body postures, exposure to mechanical elements, intense work rhythms, physical violence, and moral harassment in the workplace (Castro et al. 2019), which also lead to occupational diseases and worsen the existing social vulnerabilities among cleaning workers (Marconato et al. 2017).
Despite a growing trend in studies focused on occupational diseases and surveys that measure the functional and psychosocial aspects of work (e.g., the Copenhagen Psychological Questionnaire—COPSOQ-II) (Gonçalves and de Oliveira Sato 2020), research on the cleaning sector raises other issues: the repercussions of outsourcing on working conditions, labour exploitation, and the workers’ risk exposure (Toffolutti et al. 2021). For example, studies show that outsourcing cleaning services in hospitals lead to low hiring, poorer working conditions, and lower availability of hygiene materials, which may increase the risk of contamination (Toffolutti et al. 2017). It also has the aggravating factor of exposing workers to living with pain, suffering, and death, even if they do not engage directly with patients. This contact with death is more frequent during pandemics (Marconato et al. 2017). In another sector, the agri-food industry, some authors even speak of corporate crime because poor regulatory oversight fosters the overuse of subcontractors as a form of outsourcing labour and social responsibilities (Davies and Ollus 2019; De Gasparo et al. 2018).
Our literature review also shows that gender inequalities deeply mark the cleaning sector, reflecting the darkest dimensions of the social processes of disqualification and the precariousness of female labour. The sector emphasises how the domestic skills traditionally required of women are extended to the world of work, reproducing the segregation of social gender roles (Lefrançois et al. 2017; Young 2010; Holley and Rainnie 2012; Campbell and Price 2016).
Although a minority, men also work in this sector, sometimes in leadership positions, reflecting the rationale of male domination, and sometimes in cleaning activities that require strength and physical dexterity, thus reproducing biological determinism. In general, compared to men, women are more affected by precariousness, i.e., by greater insecurity and instability of employment, underemployment, lower wages, less social protection, and greater difficulties in reconciling work and family life, circumstances to which cleaning workers are particularly vulnerable. Consequently, substantial gender inequalities persist in this economic sector (Young 2010; McBride and Lucio 2021; Ollus 2016; Lefrançois et al. 2017). The workforce mainly involves lower-class women, ethnic minorities, migrants, low levels of schooling, part-time work, temporary work, and short-term contracts (Ollus 2016).
Recently, intersectional thinking has also gained prominence in labour and organisational studies. This approach was first used to analyse positions and experiences within the professional hierarchy and then to focus on the structural manifestations of workplace inequalities (Browne and Misra 2003). As a concept, intersectionality denotes the juxtaposition or meeting point of two or more social categories and axes or systems of power, domination or oppression (Crenshaw 2018). This framework offers theoretical explanations for how heterogeneous members of specific groups (such as cleaning women) may experience the workplace differently depending on their ethnicity, class, or other social locations (Browne and Misra 2003).
In the aftermath of the COVID-19 pandemic, little is known about how the workers in such a critical sector dealt with the extra demands associated with the pandemic and the risks they faced. Cleaning workers have remained practically invisible in the public debate about responding to the COVID-19 crisis. However, it is reasonable to assume that exposure to environments where people circulate and the risk of transmission is perceived as high would leave some marks on how workers feel about their job and their general well-being, especially their mental well-being. That was the starting hypothesis for the research presented in this paper (Roig et al. 2022; Casquilho-Martins and Belchior-Rocha 2022).
The different perspectives gathered in this research led us to question the impact of COVID-19 among female cleaning service workers, mainly at the level of their mental health. The research was based on an analytical framework that placed the socioeconomic determinants of health risks and job insecurity at the centre, along with overlapping inequalities identified in the intersectionality perspective.
3. Materials and Methods
3.1. Research and Design Methods
A quantitative methodological approach was used in this study. All data were collected by administering a questionnaire with face-to-face interviews. The final sample consisted of 436 women who performed cleaning activities in critical sectors in response to the pandemic.
The questionnaires were applied from 3 November 2020 to 17 May 2021 in different socio-professional contexts, namely:
- The two largest hospitals in the city of Porto;
- One university (fourteen faculties);
- Two large shopping centres;
- Three public services (e.g., courts, and criminal police facilities);
- Public transport companies (metro and bus).
This research focused on the different perceptions experienced by workers in their daily activities during the pandemic. The questionnaire included questions on working conditions, safety and hygiene at work, as well as on standard demographics (age, schooling, household size and composition, and income). Questions on perceptions about COVID-19 were also included, based on other previously validated, internationally referenced questionnaires, such as the Copenhagen Psychosocial Questionnaire (COPSOQ II—long version), translated into Portuguese (Rosário et al. 2017), the General Nordic Questionnaire (Wännström et al. 2009), and the COVID-19 Pandemic Mental Health Questionnaire (CoPaQ) (Rek et al. 2021; Conway et al. 2020). Some scales from the Perceived Coronavirus Threat Questionnaire were also used, which measure the impacts of COVID-19 on different levels and experiences with the infection (Coronavirus Experience Questionnaire) (Conway et al. 2020).
The questionnaire was administered face-to-face. This methodological option was fundamental to guarantee the sample size (436) and the quality of the results, such as very residual rates of nonresponse to the items included in the questionnaire. The presence of an interviewer who asked the questions and recorded the answers ensured this high response rate because the participants were able to clarify doubts or difficulties directly with the interviewer.
The interviewers remained in the field until the saturation point was reached, ending the data collection process when it became impossible to identify workers who had not already participated in the study, in a total of 72 days.
3.2. Sample and Procedures
The lack of a survey database with information on the universe of potentially eligible workers made it impossible to carry out random sampling. Hence, a non-random sampling design was chosen, which focused on selecting survey sites; that is, the places where the universe of workers carries out its work. The chosen locations ensured the typological diversity defined in the original research design (health facilities, higher education establishments, large commercial areas, public institutions, and public transport management companies). In the selected locations, all workers on duty on the day and time of the survey were invited to participate in the study. The participation rate was around 90%.
The study, informed consent form, and questionnaire were approved by the Ethics Committee of the Faculty of Arts and Humanities of the University of Porto and authorised by all the involved institutions.
In conducting the survey, the fact that cleaning service workers were not familiar with the questionnaire methodology was considered. In general, they have low levels of schooling and may fear the future use of the information obtained in more sensitive questions such as those concerning working conditions or health risks.
The team of interviewers was trained specifically for this purpose. In addition to the questionnaire, each interviewer had an observation checklist to record relevant information in line with the study’s goals. The questionnaire application period ran from 3 November 2020 to 17 May 2021.
3.3. Variables Definition, Measurements, and Data Analysis
In this section, we present the questions, scales, and variables used in the questionnaire survey to measure the main research hypothesis tested in this study, followed by data analysis.
Health conditions were assessed using the COVID-19 Pandemic Mental Health Questionnaire (CoPaQ) (Rek et al. 2021), a self-assessment measure of the personal and social consequences of the COVID-19 pandemic.
More specifically, the participants were first asked about their current health conditions, symptoms, diagnostic and serological tests, close contact with infected people and quarantine compliance, and, subsequently, about the prevalence of personal diseases and those of their household members. For each item presented, they had to indicate “yes” or “no”.
With regard to the frequency of self-protection practices, concerns about the pandemic, feelings provoked by the pandemic, and burden factors aggravated by the pandemic, the scales were again constructed using the COVID-19 Pandemic Mental Health Questionnaire (CoPaQ) (Rek et al. 2021), and responses were provided on a Likert-type scale.
This study required the reorganisation of variables to answer the research questions, particularly the hypothesis presented in this article, namely, to analyse the relationship between cleaning services during the pandemic and increased anxiety levels among cleaning workers.
In the case of health conditions, relationship profiles with COVID-19 were identified from the questions regarding diagnostic and serological testing, close contact with infected persons, and quarantine compliance. Concerning perceptions about the pandemic, dimensions of concerns, feelings, and impacts were constructed using factor analysis.
Data on the working conditions of the female cleaning workers in our sample were assessed based on their current employment status (full-time, part-time, or other situation); whether the respondent had always worked in the cleaning services sector (if yes, since what age; if no, what was the last sector of activity); which employer the respondent worked for (temporary work company or service provider); the type of contract (provision of services, fixed-term or open-ended employment contract, or other situation); how long the respondent had been working at the company and in that location; the number of working days per week; whether they worked on weekends and holidays (if yes, what period of the day); the number of working hours per week; the type of schedule (shift or fixed).
Additionally, working conditions were measured from the following questions: whether cleaning workers started to work longer hours after the start of the pandemic (if yes, every week or only some weeks; if not, whether or not the employer requested them); the type of activities they accomplished at the workplace; the type of wage (fixed or variable); the method of calculating the wage (monthly, weekly, daily, or hourly); the occurrence of accidents at work since the start of the pandemic (if so, the number of working days lost, the areas of the body where injuries were sustained, and the reasons for the accident); the occurrence of pandemic-related accidents/injuries; and the subjective assessment of exposure to the risk of contracting COVID-19 at work compared with most other occupations.
Sociodemographic data were collected through the following variables: age; height; weight; marital status; whether they had children; number of children; number of children at school; who took the children to school; number of children living together; number of household members; members aged over 65 living together; level of schooling completed; means of transport to work. In the design of the questionnaire, these questions were placed at the end of the survey, as they were considered more likely to provoke greater reservations in the participants’ answers.
The height and weight variables were recoded into a new variable—the Body Mass Index (BMI). BMI is a fundamental measure to determine the relationship between weight and height and is calculated according to the following formula: BMI = weight/(height x height), where the weight must be in kilos and the height in metres, and the result is measured in kg/m. After the result was obtained, it was classified according to the categories defined by the WHO: <18.5 = underweight; 18.5–24.9 = normal weight; 25–29.9 = pre-obese; 30–34.9 = obesity class I; 35–39.9 = obesity class II; > 40 = obesity class III.1
The marital status variable was grouped as follows: single/never married; married; cohabiting; separated/divorced; widowed. Subsequently, it was regrouped since it was relevant to distinguish the workers living in conjugality from those who do not confirm any experience of conjugality.
The SPSS software (Statistical Package for Social Sciences) version 26 was used to organise the data and produce results. The data were analysed using descriptive techniques (e.g., means, percentage).
A principal components analysis (PCA) was conducted with varimax rotation to assess the structure of items and refine the item pool by deleting poor-fitting items. Items were considered for deletion one at a time during PCA based on component loadings (not loading higher than 0.30 on any component or loadings above 0.30 on more than one component) and on commonalities (<0.30). The number of components to extract was determined using the Keyser–Meyer–Olkin criterion. The internal consistency of the different subscales with more than two items was determined by calculating Cronbach’s alpha (α) (Wännström et al. 2009; Eisinga et al. 2013). This analysis was carried out not to test whether the psychometric properties of the scales would hold in the sampled population compared to results discussed in the literature, but rather, to identify the latent structures in the data collected in preparation for the computation of the final scores.
Associations between the variables (original and derived subscales) were tested using bivariate Pearson’s correlation coefficients and unpaired two-sample and k-sample nonparametric tests (Mann–Whitney U and Kruskal–Wallis) when appropriate.
4. Results
4.1. General Characterisation of the Sample
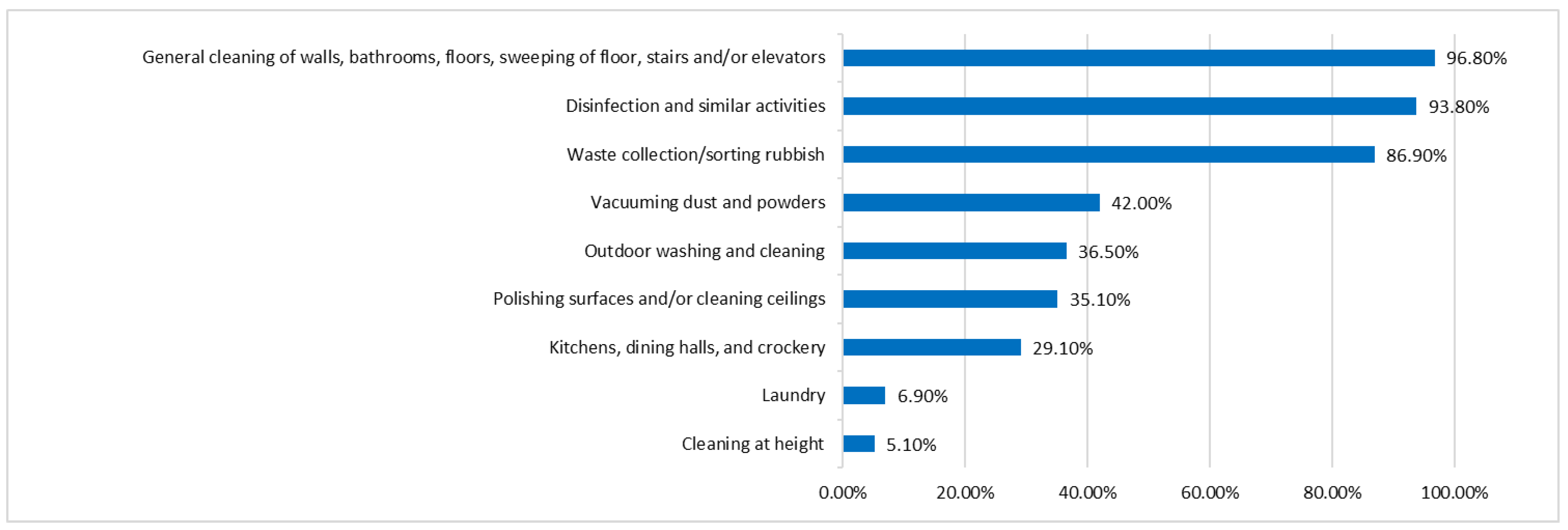
The sample characterisation was carried out on three levels: (1) general family context, in particular, household size; (2) work contexts, namely, time at the company and the workplace; and (3) which activities are developed (Figure 1).
The sample of 436 women surveyed had a varied age profile, although the age group from 51 to 60 stood out, accounting for 42.7% of the sample. This group was followed by women aged between 41 and 50 (28.4%) and between 31 and 40 (14.7%). The younger (under 30) and older (over 61) age groups had lower weights, 5.7% and 8.5%, respectively. About half of the sample lived with a partner (42.7% married, 9.6% in de facto relationships). The rest were single (21.1%), separated/divorced (19.7%) or widowed (6.9%). As expected for the professional group, the respondents’ education levels were generally low, as 86.2% had nine years or less of schooling. In fact, about one in three respondents had no more than four years of schooling. Regarding the family context, the overwhelming majority of respondents declared they were mothers (88%), 70% of whom lived with their children. Out of all our respondents, 33.7% had at least one child attending the education system, taken to school mainly by their other children (22.3%) or by their spouses/partners (23.8%). However, the most frequent solution was school transport, which 49.2% of the participants used.
Most households in the study sample were composed of two or three members (64.2%), whereas single-parent households accounted for 26.6%, and 15.6% of the sample lived with at least one person over 65 years old, an age group at increased risk due to COVID-19.
4.2. Work Conditions
Regarding the type of work, 40.5% worked part-time, and the vast majority, 87.3%, had worked for the same company for less than five years. It is common in this sector for companies to obtain service contracts under public tenders. These changes rarely imply substantive changes in the type of work and where the work is performed. However, formally, they mean changes in the contractual relationships of the workers.
About one-third of the respondents had always worked in the cleaning sector. Practically half (47.7%) started working before age 18, and 79.7% before age 21.
Regarding the number of working days, the average was five days per week (56.2%). However, almost half of the sample worked 6 or 7 days (43.1%). More than half of the workers (54.0%) worked weekends and holidays. The average workload was close to 40 h (59.6%) in a fixed work regime in the morning and afternoon. The most frequent form of remuneration was fixed (81.9%), and wages were mostly calculated on a monthly basis (70.1%). The most common activities were general cleaning, disinfection, and waste collection. (Figure 1).
Concerning changes in the volume of work resulting from the pandemic crisis, most workers said they did not experience changes in working hours (77%). However, about one in five workers had been asked to work longer hours.
Since the beginning of the pandemic, 3.9% of workers have suffered one or more accidents at work. The wrists and hands (50%), followed by the legs (37.5%), were the most affected areas of the body. The number of days lost due to accidents ranged from 0 to 150. Some respondents (3.4%) reported having suffered a problem related to the pandemic outside the professional context that led to their taking medication. This occurrence resulted from post-COVID-19 consequences (e.g., pain, muscle strains, breathing difficulties, fatigue) or a worsening of their mental health. Overall, 50% of the workers consider their work riskier than most professions when contracting COVID-19.
4.3. Health Conditions
Cleaning services are an indispensable professional sector to contain the evolution of pandemics and diseases. However, this sector is also particularly affected by precariousness and instability. Therefore, it was important to understand how the conditions for exercising this professional activity increased the risk of exposure and infection by SARS-CoV-2. Thus, the workers were asked about their health, contacts with infected people, and compliance with quarantine.
During the study, 91.8% of the workers surveyed performed at least one serological COVID-19 test, which suggested concern about the disease. Out of all workers, 5.5% tested positive, 29.4% had family members or friends who had been infected, and 2.5% lost someone close to COVID-19. It should also be noted that 27.4% had direct contact with someone infected, among which 17.1% were quarantined. The data collection occurred during the first pandemic wave before the virus suffered several mutations that increased its transmission ability. This may be one of the reasons why lower rates were recorded than those observed later with other variants of SARS-CoV-2.
It is also important to note that 37.6% of workers had at least one risk factor regarding more severe infections of COVID-19. About one in four respondents had been diagnosed with cardiovascular disease, one in seven had a chronic respiratory disease, and one in twelve was diabetic (Table 1). As for the risk of infection from third parties, 64.5% of the respondents lived with someone with at least one pre-existing disease that constituted a risk factor.
4.4. Perceptions about the Pandemic
The workers’ perceptions of the pandemic, its context, and their ability to protect themselves may have an important moderating role in their behaviour and an important role in their mental health. Table 2 summarises the data obtained in the fieldwork and the statistical analysis necessary for the final results.
Several subscales were calculated regarding the impacts of the pandemic on mental health and well-being in the target population. Fears arising from the risk that the workers themselves or those close to them could contract COVID-19 were considered. Workers were asked to rate their level of concern against a set of seven items using a four-point scale: It worries me a lot; it worries me a little; I don’t care at all; I never think about it (Table 3). The analysis resulted in constructing two subscales for anxiety regarding infection by SARS-CoV-2: COVID-contamination anxiety and COVID-health consequences anxiety. One item was eliminated due to its poor fit (“I have no means of control over the COVID-19 pandemic”).
The study also intended to analyse the prevalence of stress symptoms associated with the pandemic. Respondents were asked to rate how often they felt a set of 13 feelings on a three-point scale: “It never happened to me”, “I feel this sometimes”, and “I feel this many times” (Table 4). The analysis resulted in the construction of 3 subscales: COVID-19 social distancing stress; COVID-19 posttraumatic stress; COVID-19 internal stress. Two items were eliminated due to their poor fit (“I have avoided internal reminders of the experience of the COVID-19 pandemic (e.g., thoughts, feelings, or physical sensations)”, and “I have been feeling jumpy or easily startled”).
In order to identify the so-called disruptive factors of the context/environment that can influence the way workers to manage the pandemic, three subscales were also calculated: COVID-19 parental workload; COVID-19 health resources; COVID-19 socioeconomic resources. Respondents were asked to what extent 11 aspects of daily life were disrupted in their lives using a four-point scale: It disturbs me a lot; it disturbs me a little; it does not disturb me; I never think about it (Table 5).
Four items were eliminated due to their poor fit (“living in small accommodation”, “concerns for my own personal safety”, “concerns for the integrity of family and friends”, and “fears of what the future will bring, or that I will not be able to cope with everything”).
For the subscales with Cronbach’s alpha equal to or greater than 0.7, the respective indices were calculated using a simple summing process that maintained the original metric of the variables to facilitate the reading of the numerical results. In subscales with only two items or when Cronbach’s alpha was less than 0.7, the analysis of the original variables was chosen (Table 6).
4.5. Variation Factors in Anxiety Levels about COVID-19
The next stage involved analysing the correlations between the subscales built and between these and the sociodemographic and labour factors.
Table 7 shows the correlations between the subscales and between the subscales and items in the case of subscales with two items.
Table 8 shows the association analysis results between sociodemographic and labour indicators and the values on the subscales and items. The tested associations were found to be mostly nonsignificant. However, significant associations were identified between the measures (or lack thereof) taken by the companies and the dimensions of pandemic perception by female workers. The results follow the expected direction in a positive reading of the effects of the formation and dissemination of information.
5. Discussion
5.1. General Characterisation of the Sample, and Work and Health Conditions
The sample presented ages between 18 and 70 years old, in which the largest age group were the 51 to 60 years old, accounting for 42.7%. This fact reveals the presence of a female workforce older than the Portuguese population average. As for the households, 64.2% were composed of two or three members, in line with the values of the Portuguese population.
Another important factor detected was that a high percentage of female workers worked part-time (40.5%), which constituted a potential factor of labour instability. Consequently, this sector shows a high turnover of workers in companies. A high number, 87.3%, had remained less than five years in the same company, and 49.7% had remained less than five years in the same workplace.
In the dimension “start to work”, the vast majority of the female workers had started to work in the sector at a young age, between 18 and 21 years old (79.7%), with a fixed salary (81.9 %) paid out monthly (70.1%). This fact, associated with low qualifications, can provide a perception of stability and motivate permanence in the sector.
Furthermore, accidents and comorbidities can be a factor of instability. Due to the pandemic, this scenario was worsened if associated with a salary reduction due to lower working hours.
5.2. Perceptions about the Pandemic
The pandemic brought more extensive health, economic, and social repercussions to the sector, deepening its severe fragility and deregulation. This fact created a favourable context for the emergence of psychological vulnerability factors, with implications on the workers’ attitudes and behaviours (Pfefferbaum and North 2020).
Thus, the possibility that close relatives and friends could die from COVID-19 was at the top of the pandemic concerns. This was followed by the possibility of infecting others, namely, in the family context, and those close people could be infected with COVID-19. Only then did the possibility of contracting a severe infection and dying from the disease appear. The fear of being infected appeared only in sixth place (Table 3). Coming in the seventh and last place was the feeling of not having the means to control the pandemic. However, the most consistent responses pointed to the fear of being infected and suffering severe health consequences (Table 3).
Regarding the latent perceptions about the pandemic (Table 3), a first dimension underlined the feeling of lack of control over the situation with the potential consequences of transmission to close relatives, highlighting the perception of the risk of COVID-19.
The second dimension, which included the points “in case of infection by COVID-19, the consequences for my health will be severe”, “I will die of COVID-19”, and “people close to me will die of COVID-19”, highlighted the perception of the potential consequences of COVID-19.
The analysis of the feelings provoked by the pandemic also provided relevant insights. According to the results presented in Table 4, the feeling of alertness was the most common among the respondents, with more than half feeling this way often since the beginning of the pandemic. Disturbing dreams related to the COVID-19 pandemic were the least observed phenomenon among the respondents, even though they comprised 20% of the sample. About two-thirds confessed to making some effort not to think about the pandemic. More than a quarter shared a recurring feeling of exhaustion or sadness. Practically half of the respondents felt fragile and considered, at times, that they could no longer bear their situation. Some of the feelings listed may have been underrepresented, as a considerable number of respondents claimed they had taken antidepressant or anxiety medications to better cope with the effects of the pandemic.
All 13 items described in Table 4 showed loads > 0.5 in at least one of the two components identified. However, retaining only 46.7% of the original information means it is impossible to identify different types of impacts from the pandemic. The effects of the pandemic appear to be too complex to be segmented in this way. However, a positive result was obtained because it is possible to create an index of the pandemic’s effects on mental health.
Regarding the overload factors aggravated by the pandemic (Table 5), concerns in a domestic context proved to be the ones that least disturbed the respondents, either in terms of the size of their household or discussions with close family members. The possibility of not getting medical care was the most disturbing scenario, followed by the possibility of having to quarantine, fear about the future, and concern for the safety of those closest to them, which prevailed over personal safety. Interestingly, when it came to financial concerns, the sample was particularly polarised between the extremes of the scale. They represented an issue that was either very disturbing or not disturbing at all. Closed schools and the need to monitor children’s lessons and homework were the most represented factors in the “I never think about it” and “it doesn’t bother me” options since they mainly concerned workers who had children or lived with minors.
The results show that investing in information and dissemination can protect workers’ emotional well-being. The fact that training did not have such a direct effect raises questions about the adequacy of the provided training.
6. Conclusions and Recommendations
This study shows a number of pre-existing difficulties in the cleaning services sector. It is a labour-intensive sector that is socially underrated and predominantly female. In addition to these general characteristics, the workers have a sociodemographic profile that exacerbates the precarious conditions and risks to which the workers are exposed, even more in times of pandemics. The pandemic has worsened working conditions, feelings of insecurity, and the perception of health risks for those who do the work that no one wants to do. Cleaning is intrinsically a low-skilled and poorly paid form of employment. Thus, the sector’s needs go far beyond the direct consequences of the pandemic. Hence, a structured intervention in the sector is urgent.
In short, given the results obtained, the following measures are considered essential:
- Intervention with workers using easily understandable, (in)formative digital resources that encourage the adoption of individual protection measures.
- Development of training/information/awareness programmes aimed at management and clients to meet the sociodemographic specificities of this professional group and their working conditions.
- Reinforcement of quality assurance processes/permanent adequacy of working conditions, considering the specific needs of the workplace;
- Ergonomic adequacy of workplaces and work equipment, as well as PPE, according to the tasks and workers’ anthropometric characteristics, avoiding the use of standardised equipment;
- Increase in the quality of training provided to female workers;
- Strengthening the psychological counselling service in companies’ occupational health programmes due to the negative impacts of COVID-19 on the mental health of this professional group.
Although it was possible to establish several important recommendations, the present study also has limitations that prevent us from drawing more comprehensive conclusions. Even though the sample encompassed practically all the workers of the participating organisations, and the methodology applied seems to have been the most appropriate, there is a need to take the research further. It is essential to extend the approach to other regions as well as to male workers. We were able to detect the existence of informal work, which is processed in even more precarious conditions, but which we were unable to address in this study.
Thus, in terms of future research, bearing in mind goal number five of the 2030 Agenda for Sustainable Development and under the motto “no one is left behind”, there is an urgent need to improve the working conditions of the women who work in cleaning services in the services facility sector. Risk management and prevention measures have to be identified, and labour and social policies are devised to suit their working conditions better. Organisational and regulatory measures are required to reduce work accidents and precariousness in the sector, as well as recommendations for occupational safety and health at work. Furthermore, the companies and regulatory entities require information and training materials to prevent and reduce these women’s risk factors and precarious employment contracts. Finally, participatory change has to be operated in the cleaning sector regarding the way it relates to women workers and how it awards social and economic value to their work in general.
Author Contributions
Conceptualisation, I.D. and J.S.B.; methodology, I.D., A.L. and J.S.B.; software, A.L.; validation, A.L., I.D. and J.S.B.; formal analysis, A.L.; investigation, A.S.M. and J.A.; resources, I.D.; data curation, A.L. writing—original draft preparation, I.D. and J.S.B.; writing—review and editing, I.D., A.L., J.A. and J.S.B.; visualisation, I.D. and J.S.B.; supervision, I.D.; project administration, I.D.; funding acquisition, I.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Portuguese Foundation for Science and Technology within Project UIDB/00727/2020.
Institutional Review Board Statement
This work was approved by the Ethics Committee of the Faculty of Arts and Humanities—University of Porto on 14 October 2020.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable. All data were presented in the article.
Acknowledgments
The research team expresses deep gratitude to all the participants in this project. Acknowledgements are also extended to the participating facility services companies, and also to the institutions and other clients of these services who collaborated in the study, and all those involved in the fieldwork. It also extends its gratitude to the Portuguese Foundation for Science and Technology as a funding entity, to the University of Porto (U.Porto) and the participating research centres, the Institute of Sociology of the University of Porto (ISUP), the Centre for English, Translation, and Anglo-American Studies (CETAPS) and the Associated Laboratory for Energy, Transports, and Aeronautics (PROA/LAETA) for all their support.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study, in the collection, analysis, or interpretation of the data, in the writing of the manuscript, or in the decision to publish the results.
| 1 | https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 3 January 2022). |
References
- Bondy, Assaf S. 2018. The (dis) advantages of sector-level bargaining: Outsourcing of cleaning work and the segmentation of the Israeli industrial relations system. Journal of Industrial Relations 60: 691–710. [Google Scholar] [CrossRef]
- Browne, Irene, and Joya Misra. 2003. The intersection of gender and race in the labor market. Annual Review of Sociology 29: 487–513. [Google Scholar] [CrossRef]
- Brugière, Fabien. 2017. La Sous-Traitance en Piste. Paris: Eres, Available online: https://www.editions-eres.com/ouvrage/4063/la-sous-traitance-en-piste (accessed on 3 January 2021).
- Campbell, Iain, and Robin Price. 2016. Precarious work and precarious workers: Towards an improved conceptualisation. The Economic and Labour Relations Review 27: 314–32. [Google Scholar] [CrossRef]
- Casquilho-Martins, Inês, and Helena Belchior-Rocha. 2022. Responses to COVID-19 Social and Economic Impacts: A Comparative Analysis in Southern European Countries. Social Sciences 11: 36. [Google Scholar] [CrossRef]
- Castro, Sabrina Alessandra, Laurindo Moacir Sassi, Cassius Carvalho Torres-Pereira, and Juliana Lucena Schussel. 2019. Occupations associated with head and neck cancer in a city in Southern Brazil, 1998 to 2012. Revista Brasileira de Medicina do Trabalho 17: 1. [Google Scholar]
- Conway III, Lucian Gideon, Shailee R. Woodard, and Alivia Zubrod. 2020. Social Psychological Measurements of COVID-19: Coronavirus Perceived Threat, Government Response, Impacts, and Experiences Questionnaires. PsyArXiv. April 7. Available online: https://eprovide.mapi-trust.org/instruments/coronavirus-experiences-questionnaire (accessed on 30 May 2022).
- Crenshaw, Kimberlé. 2018. Demarginalizing the Intersection of Race and Sex: A Black Feminist Critique of Antidiscrimination Doctrine, Feminist Theory, and Antiracist Politics [1989]. London: Routledge, pp. 57–80. Available online: http://chicagounbound.uchicago.edu/uclf/vol1989/iss1/8 (accessed on 16 January 2022).
- Davies, Jon, and Natalia Ollus. 2019. Labour exploitation as corporate crime and harm: Outsourcing responsibility in food production and cleaning services supply chains. Crime, Law and Social Change 72: 87–106. [Google Scholar] [CrossRef]
- De Gasparo, Sandro, Pierre-Yves Le Dilosquer, François Hubault, and Laerte Idal Sznelwar. 2018. When Creativity Meets Value Creation. A Case Study on Daytime Cleaning. In Congress of the International Ergonomics Association. Cham: Springer, pp. 991–96. [Google Scholar] [CrossRef]
- EFCI—European Cleaning and Facility Services Industry. 2020. About Us. Available online: https://www.efci.eu/about-us/ (accessed on 16 January 2022).
- Eisinga, Rob, Manfred te Grotenhuis, and Ben Pelzer. 2013. The reliability of a two-item scale: Pearson, Cronbach, or Spearman-Brown? International Journal of Public Health 58: 637–42. [Google Scholar] [CrossRef] [PubMed]
- Eurofund. 2014. Industrial Cleaning: Working Conditions and Job Quality; Dublin: Eurofund. Available online: https://www.eurofound.europa.eu/publications/information-sheet/2014/working-conditions/industrial-cleaning-working-conditions-and-job-quality (accessed on 30 May 2022).
- Furuya, Yuko, Kota Fukai, Shoko Nakazawa, Noriko Kojimahara, Keika Hoshi, Akihiro Toyota, and Masayuki Tatemichi. 2022. Occupational physical activity differentially affects the risk for developing later-onset Crohn’s disease and ulcerative colitis among middle-aged and older populations. Scandinavian Journal of Gastroenterology 57: 206–13. [Google Scholar] [CrossRef]
- Gonçalves, Josiane Sotrate, and Tatiana de Oliveira Sato. 2020. Factors associated with musculoskeletal symptoms and heart rate variability among cleaners—Cross-sectional study. BMC Public Health 20: 774. [Google Scholar] [CrossRef]
- Holley, Sasha, and Alistair Rainnie. 2012. Who cleans up? The declining earnings position of cleaners in Australia. The Economic and Labour Review 23: 143–60. [Google Scholar] [CrossRef]
- Hughes, Everett-C. 1997. Le Regard Sociologique. Revue Française de Sociologie. Available online: https://www.persee.fr/doc/rfsoc_0035-2969_1997_num_38_4_4670 (accessed on 1 February 2022).
- ILO-Lisbon. 2020. Preparar o Regresso ao Trabalho em Segurança. Obtido de Organização internacional do Trabalho. Available online: https://www.ilo.org/lisbon/sala-de-imprensa/WCMS_742989/lang--pt/index.htm (accessed on 23 March 2021).
- INE—Instituto Nacional de Estatísticas. 2021. SÍNTESE ESTATÍSTICA SETORIAL—CAE 81—Actividades relacionadas com edifícios, plantação e manutenção de jardins. Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&cad=rja&uact=8&ved=2ahUKEwjW8NLyyrb1AhWKmBQKHSCmBeIQFnoECAwQAQ&url=https%3A%2F%2Fwww.gee.gov.pt%2Fen%2Fdocs%2Fdoc-o-gee-2%2Festatisticas-setoriais%2Fn-actividades-administrativas-e-dos-servicos-de-apoio%2F81-actividades-relacionadas-com-edificios-plantacao-e-manutencao-de-jardin%2F2426-813-actividades-de-plantacao-e-manutencao-de-jardins%2Ffile&usg=AOvVaw1AfGdONjqvqru4-wxjXLtn (accessed on 23 January 2021).
- Larsen, Trine P., Mikkel Mailand, and Thorsten Schulten. 2019. Good intentions meet harsh realities: Social dialogue and precarious work in industrial cleaning. Economic and Industrial Democracy. [Google Scholar] [CrossRef]
- Lefrançois, Melanie, Johanne Saint-Charles, and Jessica Riel. 2017. Work/Family Balancing and 24/7 Work Schedules: Network Analysis of Strategies in a Transport Company Cleaning Service: Concilier travail-famille et horaires 24/7: Analyse réseau des stratégies au sein du service de nettoyage d’une compagnie de transport. New Solutions: A Journal Of Environmental And Occupational Health Policy 27: 319–41. [Google Scholar] [CrossRef] [PubMed]
- Lhuilier, Dominique. 2005. Le sale boulot. Travailler 14: 73–98. Available online: https://www.cairn.info/revue-travailler-2005-2-page-73.htm (accessed on 30 May 2022). [CrossRef]
- Luz, Emanuelli Mancio Ferreira da, Tânia Solange Bosi de Souza Magnago, Patrícia Bitencourt Toscani Greco, Juliana Dal Ongaro, Tais Carpes Lanes, and Jadir Camargo Lemos. 2017. Prevalence and factors associated with musculoskeletal pain in hospital cleaning workers. Texto e Contexto Enfermagem 26: e00870016. Available online: https://pesquisa.bvsalud.org/portal/resource/pt/biblio-962892?src=similardocs (accessed on 30 May 2022). [CrossRef] [Green Version]
- Marconato, Cintia da Silva, Ana Carolina de Souza Magnago, Tânia Solange Bosi de Souza Magnago, Graziele de Lima Dalmolin, Rafaela Andolhe, and Juliana Petri Tavares. 2017. Prevalence and factors associated with minor psychiatric disorders in hospital housekeeping workers. Revista da Escola de Enfermagem da USP 51: 1–8. [Google Scholar] [CrossRef] [Green Version]
- McBride, Jo, and Miguel Martinez Lucio. 2021. Beyond work intensification: The contradictions and ironies of the changing nature of ‘unskilled’ work in a context of austerity and organisational change. Capital & Class 45: 145–64. [Google Scholar] [CrossRef]
- Naik, Gouri, and Mohammed Rajik Khan. 2020. Prevalence of MSDs and Postural Risk Assessment in Floor Mopping Activity Through Subjective and Objective Measures. Safety and Health at Work 11: 80–87. [Google Scholar] [CrossRef]
- Nan, Lin, Marie-Anne Rosemberg, Wei Li, Emily Meza-Wilson, Christopher Godwin, and Stuart Batterman. 2021. Occupational exposure and health risks of volatile organic compounds of hotel housekeepers: Field measurements of exposure and health risks. Indoor Air 31: 26–39. [Google Scholar] [CrossRef]
- Ollus, Natalia. 2016. Forced flexibility and exploitation: Experiences of migrant workers in the cleaning industry. Nordic Journal of Working Life Studies 6: 25–45. [Google Scholar] [CrossRef] [Green Version]
- Parra-Tapia, Elena, Guillermo Perales-Ortiz, Amado D. Quezada, and Pilar Torres-Pereda. 2019. Salud y seguridad laboral: Intervención educativa en trabajadores de limpieza en áreas de investigación. Salud Pública de México 61: 657–61. [Google Scholar] [CrossRef] [Green Version]
- Pfefferbaum, Betty, and Carol S. North. 2020. Mental health and the COVID-19 pandemic. New England Journal of Medicine 383: 510–12. [Google Scholar] [CrossRef]
- Rek, Stephanie V., Markus Bühner, Matthias A. Reinhard, Daniel Freeman, Daniel Keeser, Kristina Adorjan, Peter Falkai, and Frank Padberg. 2021. The COVID-19 Pandemic Mental Health Questionnaire (CoPaQ): Psychometric evaluation and compliance with countermeasures in psychiatric inpatients and non-clinical individuals. BMC Psychiatry 21: 426. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, Alice, Ana Falcato, Antónia Baptista, Carlos Silva Santos, Helena Krippahl, João Paulo Moreira, Maria José Liberat, and Sandra Moreira. 2013. Documento de referência: Atuação dos Industriais no âmbito do SIR (Segurança e Saúde do Trabalho); Lisboa: ACT, (PDF). Available online: https://www.act.gov.pt/(pt-PT)/crc/PublicacoesElectronicas/Documents/ATUACAODOSINDUSTRIAISNOAMBITODOSISTEMADAINDUSTRIARESPONSAVEL_SIR.pdf (accessed on 30 May 2022).
- Roig, Rosa, Cristina Aybar, and Jose M. Pavía. 2022. COVID-19, Gender Housework Division and Municipality Size in Spain. Social Sciences 11: 37. [Google Scholar] [CrossRef]
- Rosário, Susel, Luís F. Azevedo, João A. Fonseca, Albert Nienhaus, Matthias Nübling, and José Torres Costa. 2017. The Portuguese long version of the Copenhagen Psychosocial Questionnaire II (COPSOQ II)—A validation study. Journal of Occupational Medicine and Toxicology 12: 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruokolainen, Joonas, Marko Hyttinen, Jouni Sorvari, and Pertti Pasanen. 2022. Exposure of cleaning workers to chemical agents and physical conditions in swimming pools and spas. Air Quality, Atmosphere & Health 15: 521–40. [Google Scholar] [CrossRef]
- Scandella, Fabienne. 2010. The Hidden Face of a Booming Industry. HesaMag: European Trade Union Institute, pp. 12–15. Available online: https://www.etui.org/topics/health-safety-working-conditions/hesamag/cleaning-up-workers-under-pressure/the-hidden-face-of-a-booming-industry. (accessed on 23 March 2021).
- Soo-Jeong, Lee, Minjung Kyung, Cherry Leung, and OiSaeng Hong. 2021. Gender differences in experience and reporting of acute symptoms among cleaning staff. American Journal of Industrial Medicine 64: 528–39. [Google Scholar] [CrossRef]
- Suleiman, Abdulqadir M., and Kristin V. H. Svendsen. 2015. Effectuality of cleaning workers’ training and cleaning enterprises’ chemical health hazard risk profiling. Safety and Health at Work 6: 345–52. [Google Scholar] [CrossRef] [Green Version]
- Sun, Pengfei, Xiaosheng Lu, Chao Xu, Wenjuan Sun, and Bo Pan. 2020. Understanding of COVID-19 based on current evidence. Journal of Medical Virology 92: 548–51. [Google Scholar] [CrossRef]
- Taş, Tuncay Aydin, Nalan Akiş, and Hayriye Saricaoğlu. 2021. Occupational Contact Dermatitis in Hospital Cleaning Worker. Dermatitis 32: 388–96. [Google Scholar] [CrossRef]
- Toffolutti, Veronica, David Stuckler, Martin McKee, Ineke Wolsey, Judith Chapman, Theo J Pimm, Joanne Ryder, Heather Salt, and David M Clark. 2021. The employment and mental health impact of integrated Improving Access to Psychological Therapies: Evidence on secondary health care utilization from a pragmatic trial in three English counties. Journal of Health Services Research & Policy 26: 224–33. [Google Scholar] [CrossRef]
- Toffolutti, Veronica, Martin McKee, and David Stuckler. 2017. Evidence points to ‘gaming’ at hospitals subject to National Health Service Cleanliness Inspections. Health Affairs 36: 355–61. [Google Scholar] [CrossRef] [PubMed]
- Unge, Jeannette, Kerstina Ohlsson, Catarina Nordander, Gert-Åke Hansson, StaVan Skerfving, and Istvan Balogh. 2007. Differences in physical workload, psychosocial factors and musculoskeletal disorders between two groups of female hospital cleaners with two diverse organizational models. International Archives of Occupational and Environmental Health 81: 209–20. [Google Scholar] [CrossRef] [PubMed]
- Wännström, Ingrid, Ulla Peterson, Marie Åsberg, Åke Nygren, and J. Petter Gustavsson. 2009. Psychometric properties of scales in the General Nordic Questionnaire for Psychological and Social Factors at Work (QPS): Confirmatory factor analysis and prediction of certified long-term sickness absence. Scandinavian Journal of Psychology 50: 231–44. [Google Scholar] [CrossRef] [PubMed]
- Young, Marisa. C. 2010. Gender differences in precarious work settings. Relations Industrielles/Industrial Relations 65: 74–97. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Activities performed at the workplace.


{kind=link}
Table 1.
Prevalence of pre-existing diseases in the sample by disease.
| Prevalence of Pre-Existing Diseases | n | % |
|---|---|---|
| Cardiovascular disease | 105 | 24.1 |
| Chronic disease of the respiratory system | 59 | 13.5 |
| Diabetes | 35 | 8.0 |
| Immunodeficiency, or taking immunosuppressant medication | 15 | 3.4 |
| Cancer in the last five years | 7 | 1.6 |
| Chronic kidney disease | 6 | 1.4 |
| Cancer | 5 | 1.1 |
| Chronic liver disease | 3 | 0.7 |
Table 2.
Sociodemographic characterisation.
| Age Groups | No. | % |
|---|---|---|
| ≤20 years old | 3 | 0.7 |
| 21–30 years old | 22 | 5.0 |
| 31–40 years old | 64 | 14.7 |
| 41–50 years old | 124 | 28.4 |
| 51–60 years old | 186 | 42.7 |
| 61–70 years old | 37 | 8.5 |
| Marital Status | ||
| Single/never married | 92 | 21.1 |
| Married | 186 | 42.7 |
| De facto union | 42 | 9.6 |
| Separated/divorced | 86 | 19.7 |
| Widow | 30 | 6.9 |
| Level of Schooling | ||
| Did not finish 4th grade | 14 | 3.2 |
| 4th grade | 143 | 32.8 |
| 5th/6th grade | 83 | 19.0 |
| 7th/8th or 9th grade | 136 | 31.2 |
| 10th/11th or 12th grade | 56 | 12.8 |
| Higher | 4 | 0.9 |
Table 3.
Concerns about the pandemic.
| Concerns about the Pandemic | It Worries Me a Lot | It Worries Me a Little | I Don’t Care at All | I Never Think about It | ||||
|---|---|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | No. | % | |
| I have no means of control over the COVID-19 pandemic. | 251 | 57.8 | 134 | 30.9 | 43 | 9.9 | 6 | 1.4 |
| I will become infected with COVID-19 | 283 | 64.9 | 96 | 22 | 45 | 10.3 | 12 | 2.8 |
| People close to me are infected with COVID-19 | 346 | 79.4 | 72 | 16.5 | 16 | 3.7 | 2 | 0.5 |
| I will infect other people with COVID-19 | 374 | 85.5 | 40 | 9.2 | 18 | 4.1 | 4 | 0.9 |
| In case of infection by COVID-19 the health consequences will be severe | 343 | 78.7 | 70 | 16.1 | 16 | 3.7 | 5 | 1.2 |
| I will die of COVID-19 | 295 | 67.8 | 45 | 10.3 | 49 | 11.3 | 46 | 10.6 |
| People close to me will die of COVID-19 | 375 | 86.0 | 33 | 7.6 | 10 | 2.3 | 18 | 4.1 |
Note: There are two omitted cases in the options “feeling that you do not have the means to control the COVID-19 pandemic” and “in case of infection by COVID-19, the health consequences will be severe”, and one omitted case in the option “dying of COVID-19” that corresponds to the answer “I don’t know”.
Table 4.
Feelings caused by the pandemic.
| Feelings Caused by the COVID-19 Pandemic | I Feel This Many Times | I Feel This Sometimes | It Never Happened to Me | |||
|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | |
| 24 | 5.5 | 66 | 15.2 | 343 | 79.2 |
| 42 | 9.6 | 73 | 16.7 | 321 | 73.6 |
| 139 | 31.9 | 161 | 36.9 | 136 | 31.2 |
| 212 | 48.6 | 136 | 31.2 | 88 | 20.2 |
| 244 | 56.2 | 146 | 33.6 | 44 | 10.1 |
| 113 | 26.0 | 156 | 35.9 | 166 | 38.2 |
| 30 | 6.9 | 64 | 14.7 | 342 | 78.4 |
| 48 | 11.0 | 77 | 17.7 | 311 | 71.3 |
| 123 | 28.2 | 144 | 33.0 | 169 | 38.8 |
| 114 | 26.1 | 158 | 36.2 | 164 | 37.6 |
| 70 | 16.1 | 149 | 34.3 | 216 | 49.7 |
| 105 | 24.1 | 158 | 36.2 | 173 | 39.7 |
| 85 | 19.5 | 104 | 23.9 | 246 | 56.6 |
Note: There are three omitted cases in the option “I have had upsetting dreams that replay part of the experience of the COVID-19 pandemic or are clearly related to it” that correspond to the answer “I don’t know”; two omitted cases in the option “I have been ‘super-alert’, watchful, or on guard” that corresponds to the answer “does not reply”; and one omitted case in the options “I have been feeling jumpy or easily startled”, “I have been feeling frail and susceptible of getting sick”, and “I have thought: ‘I cannot take this anymore’” that corresponds to the answer “I don’t know”.
Table 5.
Overload factors aggravated by the pandemic.
| Overload Factors Aggravated by the Pandemic | It Disturbs Me a lot | It Disturbs Me a Little | It Does Not Disturb Me | I Never Think about It | ||||
|---|---|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | No. | % | |
| Living in small accommodation | 47 | 10.8 | 55 | 12.6 | 305 | 70.0 | 29 | 6.7 |
| Being under curfew | 253 | 58.0 | 82 | 18.8 | 79 | 18.1 | 22 | 5.0 |
| Childcare services and schools shut down | 123 | 28.2 | 78 | 17.9 | 177 | 40.6 | 58 | 13.3 |
| Taking over school lessons | 49 | 11.2 | 35 | 8.0 | 241 | 55.3 | 111 | 25.2 |
| Not being able to get medical care | 264 | 60.7 | 99 | 22.8 | 69 | 15.9 | 3 | 0.7 |
| Increased conflicts with people close to me | 76 | 17.4 | 63 | 14.4 | 289 | 66.3 | 8 | 1.8 |
| Financial worries | 189 | 43.3 | 71 | 16.3 | 175 | 40.1 | 1 | 0.2 |
| Uncertainties regarding my job (unemployment, lay-off, working more hours, working less hours) | 187 | 42.9 | 78 | 17.9 | 165 | 37.8 | 6 | 1.4 |
| Concerns for my own personal safety | 137 | 31.5 | 132 | 30.3 | 158 | 36.3 | 8 | 1.8 |
| Concerns for the well-being of family or friends | 236 | 54.1 | 132 | 30.3 | 64 | 14.7 | 4 | 0.9 |
| Fears of what the future will bring, or that I will not be able to cope with everything | 242 | 55.8 | 124 | 28.6 | 59 | 13.6 | 9 | 2.1 |
Note: There is one omitted case in the options “not being able to get medical care” and “concerns for my own personal safety” and two omitted cases in the option “fears of what the future will bring, or that I will not be able to cope with everything” that corresponds to the answer “I don’t know”.
Table 6.
Final items, factor loadings, commonalities and Cronbach’s alpha of the subscales in the sample.
Table 6.
Final items, factor loadings, commonalities and Cronbach’s alpha of the subscales in the sample.
| Items on the Subscale | Component Loadings | Communalities | Cronbach’s Alpha |
|---|---|---|---|
| COVID-19 infection anxiety | |||
| I will become infected by COVID-19. | 0.766 | 0.667 | |
| People close to me are infected with COVID-19. | 0.836 | 0.716 | 0.715 |
| I will infect other people with COVID-19. | 0.741 | 0.577 | |
| COVID-19 health consequences anxiety | |||
| In case of infection by COVID-19 the consequences for my health will be severe. | 0.641 | 0.534 | 0.700 |
| I will die of COVID-19. | 0.838 | 0.722 | |
| People close to me will die of COVID-19. | 0.825 | 0.702 | |
| COVID-19 social distancing stress | |||
| I have avoided external reminders of the experience of the COVID-19 pandemic (e.g., people, places, conversations, objects, activities, or situations). | 0.777 | 0.615 | - |
| I have been “super-alert”, watchful, or on guard. | 0.807 | 0.657 | - |
| COVID-19 post-traumatic stress | |||
| I have had upsetting dreams that replay part of the experience of the COVID-19 pandemic or are clearly related to it. | 0.846 | 0.764 | - |
| I have had powerful images or memories that sometimes come to into my mind in which I feel the experience of the COVID-19 pandemic is happening again here and now. | 0.832 | 0.741 | - |
| COVID-19 internal stress | |||
| I have suffered from unforeseeable severe anxiety attacks (panic) with physical symptoms (e.g., palpitations, chest pain, dizziness). | 0.557 | 0.319 | |
| I have been sleeping badly and restless. | 0.655 | 0.471 | 0.825 |
| I have been feeling exhausted and worn-out. | 0.716 | 0.554 | |
| I have been feeling sad. | 0.645 | 0.521 | |
| I have been feeling frail and susceptible to getting sick. | 0.713 | 0.539 | |
| I felt or behaved in a more irritable, rageful, angry way. | 0.762 | 0.583 | |
| I have thought: “I cannot take this anymore”. | 0.718 | 0.523 | |
| COVID-19 parental workload | |||
| Childcare services and schools shut down. | 0.819 | 0.744 | - |
| Taking over school lessons. | 0.864 | 0.777 | - |
| COVID-19 health resources | |||
| Being under curfew. | 0.816 | 0.675 | - |
| Not being able to get medical care. | 0.735 | 0.572 | - |
| COVID-19 socioeconomic resources | |||
| Increased conflicts with people close to me. | 0.656 | 0.465 | 0.650 |
| Financial worries. | 0.817 | 0.697 | - |
| Uncertainties regarding my job (unemployment, lay-off, working more hours, working less hours). | 0.768 | 0.629 | - |
Table 7.
Correlations between the subscales in the sample.
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | ||
|---|---|---|---|---|---|---|---|---|
| 1 | COVID-19 infection anxiety | - | ||||||
| 2 | COVID-19 health consequences anxiety | 0.486 ** | - | |||||
| 3 | COVID-19 internal stress | 0.118 * | 0.230 ** | - | ||||
| 4 | COVID-19 social distancing stress-I have avoided external reminders | 0.201 ** | 0.241 | 0.379 ** | - | |||
| 5 | COVID-19 social distancing stress-I have been “super-alert” | 0.287 ** | 0.214 ** | 0.060 | 0.175 ** | - | ||
| 6 | COVID-19 post-traumatic stress-I have had powerful images | 0.362 ** | 0.181 ** | 0.121 * | 0.342 ** | 0.156 ** | - | |
| 7 | COVID-19 post-traumatic stress-I have had upsetting dreams | 0.137 ** | 0.149 ** | 0.358 ** | 0.173 ** | 0.115 ** | 0.518 ** | - |
* Significant at 5% (two-sided); ** significant at 1% (two-sided).
Table 8.
Statistical tests.
| COVID-19 Infection Anxiety | COVID-19 Health Consequences Anxiety | COVID-19 Internal Stress | ||||
|---|---|---|---|---|---|---|
| Test | p-Value | Test | p-Value | Test | p-Value | |
| Age-groups (1) | 0.669 | 0.881 | 3.192 | 0.363 | 0.122 | 0.989 |
| Lives with spouse (yes) (2) | −0.472 | 0.637 | −0.081 | 0.936 | −0.583 | 0.560 |
| Full-time work (yes) (2) | −0.014 | 0.989 | −0.310 | 0.756 | −0.423 | 0.672 |
| Got information on COVID-19 from employer (yes) (2) | −1.013 | 0.311 | −2.083 * | 0.037 | −0.319 | 0.750 |
| Got information on COVID-19 from supervisor (yes) (2) | −0.816 | 0.415 | −2.582 * | 0.010 | −0.508 | 0.612 |
| Got written information on COVID-19 from employer (yes) (2) | −3.711 * | <0.001 | −2.765 * | 0.006 | −0.406 | 0.685 |
| Got training sessions on how to handle COVID-19 (yes) (2) | −0.246 | 0.805 | −0.445 | 0.656 | −0.270 | 0.787 |
(1) Kruskal–Wallis test; (2) Mann–Whitney U test; * statistically significant.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Dias, I.; Lopes, A.; Azevedo, J.; Maia, A.S.; Baptista, J.S. Cleaning in Times of Pandemic: Perceptions of COVID-19 Risks among Workers in Facility Services. Soc. Sci. 2022, 11, 276. https://doi.org/10.3390/socsci11070276
AMA Style
Dias I, Lopes A, Azevedo J, Maia AS, Baptista JS. Cleaning in Times of Pandemic: Perceptions of COVID-19 Risks among Workers in Facility Services. Social Sciences. 2022; 11(7):276. https://doi.org/10.3390/socsci11070276
Chicago/Turabian StyleDias, Isabel, Alexandra Lopes, José Azevedo, Ana Sofia Maia, and João Santos Baptista. 2022. "Cleaning in Times of Pandemic: Perceptions of COVID-19 Risks among Workers in Facility Services" Social Sciences 11, no. 7: 276. https://doi.org/10.3390/socsci11070276
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.