
The Role of the Hypothalamus–Pituitary–Adrenal (HPA) Axis in Test-Induced Anxiety: Assessments, Physiological Responses, and Molecular Details


1
Division of Education, Lourdes University, Sylvania, OH 43560, USA
2
Department of Physiology and Pharmacology, University of Toledo College of Medicine, Toledo, OH 43614, USA
*
Author to whom correspondence should be addressed.
Stresses 2022, 2(1), 146-155; https://doi.org/10.3390/stresses2010011
Submission received: 2 January 2022
/
Revised: 26 February 2022
/
Accepted: 8 March 2022
/
Published: 14 March 2022
(This article belongs to the Section Animal and Human Stresses)
{kind=link}
{kind=link}
Abstract
:Test anxiety may be a contributing factor to low-performing examination scores among students. There can be numerous physiological responses in the body that lead to test anxiety. One is the body’s response to stress, which activates the brain to release hormones that stimulate central and peripheral nervous responses. The hypothalamus–pituitary–adrenal (HPA) axis is a known responder during stress, causing an elevation of cortisol in the blood, a glucocorticoid (GC) hormone that affects sympathetic nervous responses. Stressors during testing include the method of information delivered, prior knowledge of the subject material, emotional state, or how accurately the student can retain knowledge. A student’s emotional state of mind is essential and may cause hyperactivation of the HPA axis during stress encountered during testing, exacerbating cortisol levels and nervous responsiveness. This review discusses the potential involvement of the HPA stress axis on an individual’s performance during testing and assessment.
1. Introduction
There is an increasing emphasis on testing, especially in math and reading achievement, for national development, economic competitiveness, and fostering of autonomy [1]. However, many students suffer from anxiety because of the stress that ensues from such competitiveness [2,3]. Some students benefit from accommodations that may lower their stress and anxiety [4]. According to Sawker-Miller, test anxiety refers to the psychological, cognitive, and/or behavioral symptoms of anxiety before or during the test-taking situation that may interfere with testing performance [5]. Many students with test anxiety struggle to stay focused on the test, which can lead to poor test performance [6]. Test anxiety is one of the most troublesome factors in school, yet it has not been adequately addressed [7,8,9]. This particularly affects those who are struggling academically or characterized as having a learning disability (LD).
Test anxiety and general anxiety disorders are related to certain kinds of psychological behaviors that are defined under the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). Test anxiety is a significant factor contributing to lower academic performance and test scores, as previous studies have shown that test anxiety is associated with lower academic performance among students [10,11,12,13]. Pekrun et al. showed that test anxiety reduces working memory and causes impairment of performance with more complex or challenging tasks [14]. This may be related to physiological stressors that are triggered by the psychological events of test anxiety. There are accommodations, discussed below, for students to understand their stressors and to take action to help cope with these events during a test.
Test anxiety is an issue among all students but is more pronounced in grades 3 through 12 and may be a factor in poor performance for some learners. Inadequate testing and poorly understood physiological responses during assessment (e.g., cortisol and physiological stress hormones) could be underlying issues that exacerbate test anxiety. Underperforming during testing may affect a student into adulthood and limit a person’s ability to find employment and live independently. Approximately one-third of all students are predicted to have test anxiety, regardless of their ability level [15]. Numerous stressors can lead to test anxiety, affecting how a student receives, stores, and understands information. In this review, we discuss the physiological responses of the human brain and how the stressors signal molecularly to hinder an individual’s cognitive abilities, which can affect anxiety and stress during testing scenarios. We also discuss how accommodations are helpful for preventing stressful scenarios and explain some strategies that may help improve test anxiety.
2. Stress Regulation via the Hypothalamus–Pituitary–Adrenal Axis (HPA)
The stress hormone glucocorticoids (GCs) can affect how an individual remembers events and stores information. This endocrine response activates the hypothalamic–pituitary–adrenal (HPA) axis, providing the functionality of the body that coordinates physiological responses to different stimuli that control peripheral and central nervous responses [16,17,18]. The HPA axis responds to physical or psychological stressors that are known to provoke the secretion of catecholamine, epinephrine, and norepinephrine via the sympathetic nervous system and GCs via the adrenal gland [19]. Having a steady rate of GCs is vital, especially in hormonal control of cognitive abilities. When an individual consistently has too much or too little GCs, such as cortisol, it can affect their daily functions. An excessive amount of cortisol can cause Cushing’s syndrome, while a cortisol deficiency can cause Addison’s disease. When there are extended periods of elevated cortisol, it can cause anxiety and affect one’s memory. There is minimal information about how the human brain reacts in stressful situations, especially during testing.
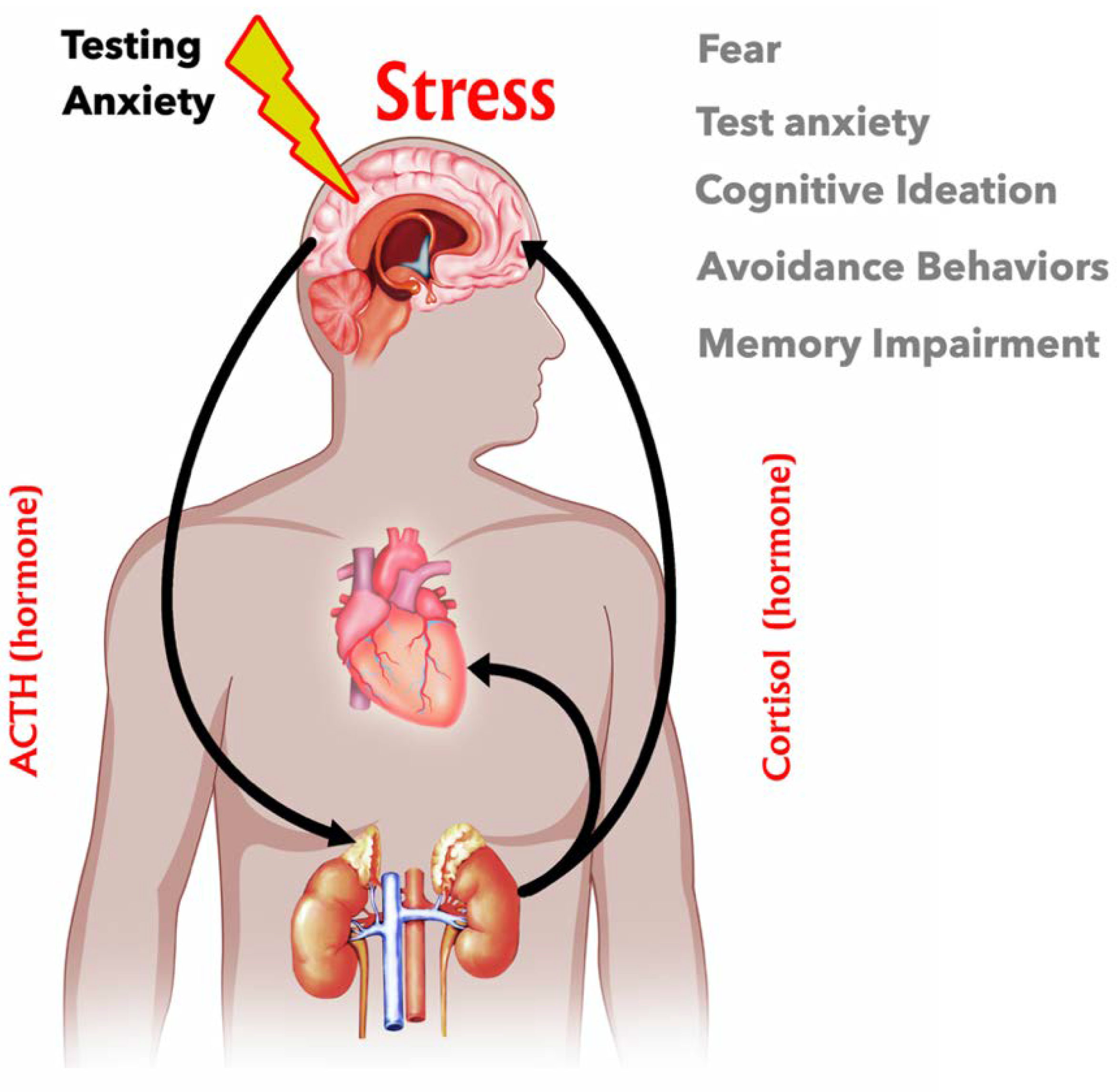
Many factors can contribute to psychological stress, including test-taking, post-traumatic stress disorder (PTSD), anxiety, depression, restraint stress, and social anxiety. Stress causes the release of hormones that physiologically regulate several processes of the nervous system. Beginning in the hypothalamus, stress activates the first step in the process of the HPA axis (Figure 1). The hypothalamus impacts many aspects of everyday life, such as energy, food intake, body weight, fluid intake and balance, sleep cycle, blood pressure, thirst, and body temperature [20]. The hypothalamus contains neuroendocrine cells that synthesize and release corticotrophin-releasing hormone (CRH) [20]. This is the area of the brain that coordinates the physiological responses of different organs, which, together, maintain homeostasis. The secretion of CRH activates the release of adrenocorticotropic hormone (ACTH) from the pituitary that enters the blood and activates the adrenal gland to produce cortisol, the most dominant glucocorticoid (GC) in humans. Glucocorticoids are derived from cholesterol through synthesis via the steroid biosynthesis pathway. GCs have homeostatic control over several aspects of the body, including suppressing osteoblast formation [21] and gluconeogenesis in the liver produced from the amino acid breakdown in muscle and fat in adipose tissue [17]. In the immune system, GCs cause rapid suppression and management of overgrowth of T cells [22], and because of this, they are the number one prescribed anti-inflammatory drug. For these reasons, physiological stress that increases blood levels of cortisol may lead to hyperglycemia, insulin resistance, decreased protein in bone and muscle, hyperlipemia, infection, or decreased ACTH [23]. On the other hand, reducing plasma cortisol levels may result in hypoglycemia, insulin sensitivity, weight loss, hypotension, anorexia, fatigue, increased ACTH, or pigmentation of the skin [23]. Overall, the HPA axis plays an integral part in one’s homeostasis, affecting whether cortisol levels increase or decrease.
The adrenal glands are small, but they play a significant role in the body. Hormones released from the adrenal glands can be in minute levels in the blood but serve as significant mediators of homeostasis. The purposes of the adrenal glands are to protect an individual against acute and chronic stress [23]. These hormones are commonly referred to as epinephrine and norepinephrine. Epinephrine accounts for 80 percent of the adrenal catecholamine secretion, and norepinephrine accounts for the remaining 20 percent. Epinephrine is also known as adrenaline and is an amino-acid-derived hormone that is secreted from the adrenal glands in response to stress. Norepinephrine is a neurotransmitter found in the locus coeruleus, which is combined with dopamine [23]. These hormones increase one’s heart rate, improve eyesight for a period of time, increase blood pressure, and increase the amount of oxygen that one breathes [24]. The sympathetic nervous system is also known as the fight-or-flight neurological response. With acute stress, catecholamines (adrenaline) mobilize glucose and fatty acids for energy and prepare the heart, liver, and skeletal muscle for action [23]. Glucocorticoids protect against overreactions from the body’s responses to chronic stress, threatening homeostasis [23]. With chronic stress and food and fluid deprivation, the cortical steroid hormone cortisol stimulates gluconeogenesis to maintain the supply of glucose. At the same time, the mineralocorticoid aldosterone serves to increase sodium reabsorption to maintain body fluid content [23]. Glucocorticoids are essential in maintaining processes at times of prolonged stress and suppressing inflammatory pathways [23]. When there is a deficit in the amount of cortisol produced, it is known as Addison’s disease, which is usually caused by tuberculosis destroying the glands or by genetic mutations. Patients with Addison’s disease, such as U.S. President John F. Kennedy, exhibit weakness in the skeletal muscle, fatigue, and browning of the skin. Other symptoms may include fatigue, muscle weakness, loss of appetite, weight loss, or abdominal pain [25]. Treatments for Addison’s disease include medications containing synthetic glucocorticoids.
When there is an excessive amount of cortisol and an overproduction of ACTH by the pituitary or by the ecotopic, the hyper ACTH secretion might be produced by a tumor, which then causes the adrenals to overproduce cortisol chronically. This is commonly referred to as Cushing’s syndrome and is the overproduction of cortisol from a tumor in the pituitary or adrenal gland. Patients with Cushing’s syndrome, such as U.S. President George Bush Sr., may experience upper body weight gain, a rounded face, or increased fat in the neck region. Other symptoms may include fatigue, muscle weakness, depression, anxiety, high blood pressure, high blood sugar, or headache. How Cushing’s syndrome is treated is dependent on the symptoms that each individual may have. For individuals with a tumor, it would be necessary to remove the tumor, the pituitary, or adrenal glands. Other treatments may include hormone-inhibiting drugs, chemotherapy, or radiation [16,25].
3. Cellular and Molecular Actions of GCs
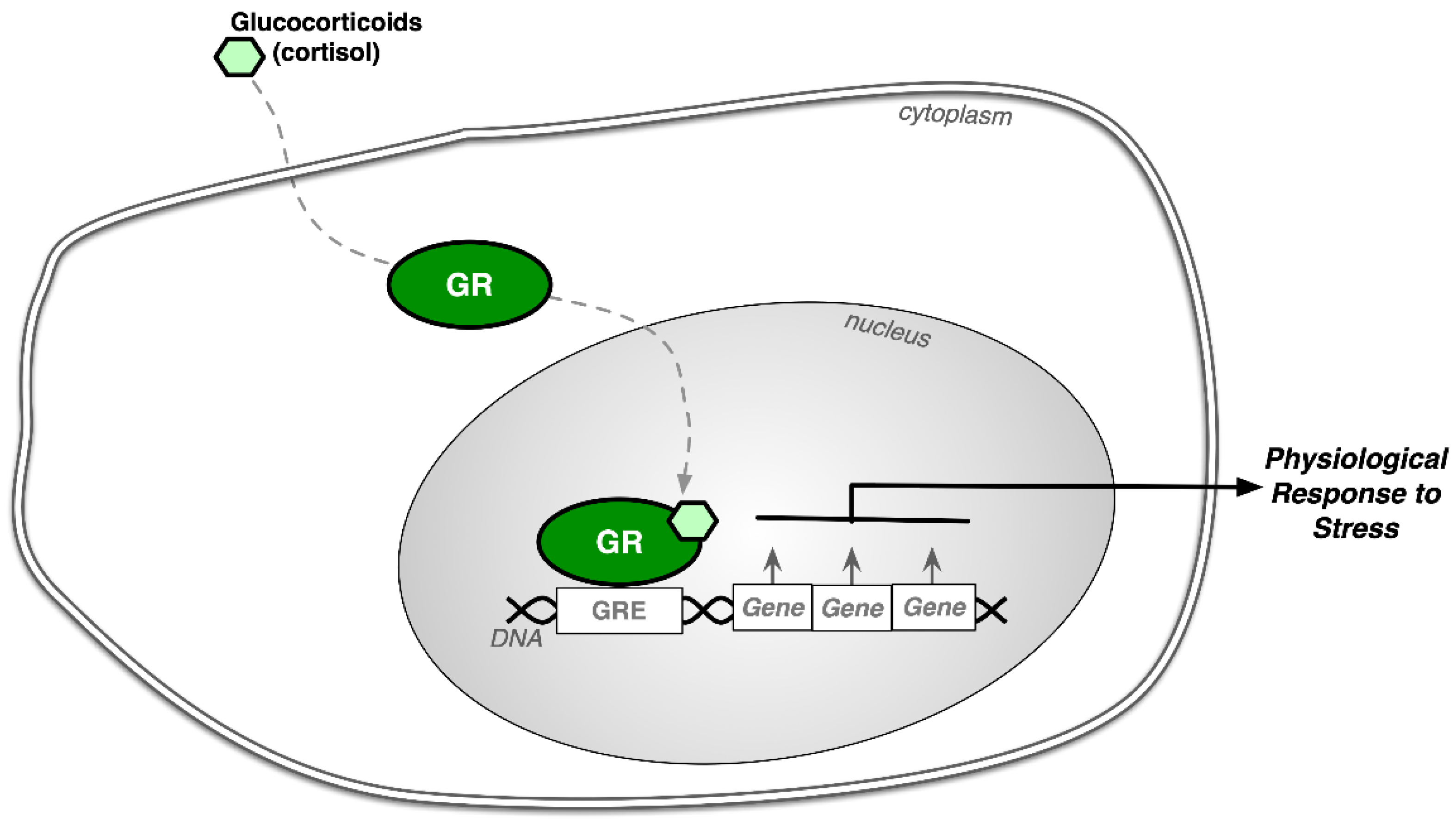
The cellular and molecular actions of GCs start when the adrenal steroids enter cells by passive diffusion and then bind to the glucocorticoid receptor (GR). The GR is a polypeptide that binds GCs with high affinity [23]. Once the steroid cortisol binds to the GR, the receptor translocates to the nucleus, where it binds to glucocorticoid response elements in specific DNA sequences (Figure 2) [23,26]. At this time, a change occurs in the transcriptional rate of messenger RNA of specific genes regulated by the GR. This then changes the cell’s content of specific proteins via gene regulation [23]. Mineralocorticoids, a group of corticosteroid hormones, bind to the mineralocorticoid receptor (MR), predominantly found in tissues in the kidney, colon, and salivary glands [17]. These areas have a high affinity for aldosterone, a natural mineralocorticoid, and are considered type I receptors (MR), whereas GR is considered a type II receptor [23]. Within living organisms, mineralocorticoid targeted tissues have 11beta-hydroxysteroid dehydrogenase (11beta HSD), a type II enzyme that helps convert the natural glucocorticoid cortisol into cortisone, which has low affinity to GR but high affinity to MR [17,23]. Mineralocorticoids and MR are essential for electrolyte balance and sodium and potassium uptake and, therefore, essential for blood pressure control. On the other hand, cortisol has a high affinity for GR and is the primary adrenal steroid controlling the GR-mediated physiological processes described earlier.
4. Effects of Glucocorticoids on the Brain
GCs play an essential role in brain function and how the body responds to stress and environmental situations. The primary GC in humans is cortisol, and the primary GC in rodents is corticosterone [27]. A review by Peffer et al. discussed the difference that cortisol can make in one’s life starting in the womb and the essential role that the timing of stress and release of GCs play during gestation [28]. If maternal stress occurs throughout the second half of gestation, it may lead to increased cortisol and stress responses in childhood and adolescence. Also, in this study, female children who were born to mothers with anxiety in the first trimester were found to be susceptible to affective disorders, whereas children whose mothers experienced stress later in gestation were more prone to developing attention deficit hyperactivity disorder (ADHD).
The effects of GCs on the brain are significant to the cognition functions of the brain [29]. The combination of the levels of GCs and the history of exposure prior to assessment may influence learning and memory [27]. The level of GCs has an impact on the measures of how the brain functions and the retention involved in learning and memory [27]. The presence of stressors before assessing learning and memory may either deteriorate or enhance memory [30]. With chronic stress, dehydroepiandrosterone (DHEA) concentrations decrease while cortisol levels may remain steady or rise, resulting in hormone imbalance [31]. If the hormone imbalance is chronic, it can result in permanent changes to the body and brain [32]. If the overproduction of GCs lasts for several weeks, it can cause atrophy of hippocampal dendrites and permanent loss of hippocampal neurons [33]. Chronic stress has also been shown to adversely affect hippocampus-dependent spatial learning [16]. Damage to the hippocampal part of the brain could result in depression or post-traumatic stress disorder (PTSD). There is an increase in GCs during PTSD, but it is unknown if the atrophy occurs before the PTSD and depression or if the atrophy results from the depression and PTSD [33].
When the GC receptor is activated due to traumatic events, the deleterious effects of stress-associated psychiatric disorders are greatened [34], which might form the basis for the development of PTSD. According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) [35], PTSD is the development of disturbances that interfere with social, occupational, or other areas of functioning following a traumatic event for more than one month. The DSM-5 is a handbook used by health care professionals in the United States (U.S.) and other parts of the world as a guide to diagnosing mental disorders. The DSM-5 contains descriptions, symptoms, and other bases for diagnosing mental disorders. The language used in DSM establishes a common language for trained clinicians. The DSM-5 also gives researchers criteria to study for potential future revisions and aid in developing interventions and medications. PTSD may have an abnormal effect on stress, which may be prevalent in the neurobiological systems inducing stress, including endocrine and neurotransmitter pathways [18]. However, patients with PTSD may have abnormal regulations of cortisol and thyroid hormones [18]. Gender can also play a role in PTSD. Women tend to develop PTSD more frequently than men by a margin of 2:1 [18].
Approximately one in six individuals will suffer from depression in their lifetime [36]. According to the World Health Organization [37], depression was expected to be the second leading cause of disability in 2020, behind heart disease. Some sources suggest that depression could be caused by an increase in the levels of GC hormones in individuals and the hyperactivity of the HPA axis [38]. The DSM-5 defined depression as the presence of a sad, empty, or irritable mood, along with somatic and cognitive changes in how an individual may function [35].
Individuals may also have decreased sleeping hours, energy levels, and self-image. The symptoms typically last two or more weeks, depending on the individual and the scenario. Both gender and age play a role in depression. It occurs more often during the ages of 18 to 29 and in individuals older than 60 years of age. Females experience a 1.5- to 3-fold higher rate than males in adolescent years [35]. According to the Anxiety and Depression Association of America [39], there are three main types of depressive disorders: major depression, persistent depressive disorder (PDD), and bipolar disorder. Major depression involves disruptions in eating, sleep, and the ability to work. Some individuals may feel that their life is not worth living, and some will attempt to end their lives. PDD is a more chronic form of depression that typically lasts for two years. The symptoms are similar to those of major depression, including low energy, poor appetite or overeating, and insomnia or oversleeping. The third type of depression is bipolar disorder. This is characterized as a shift in behaviors from extreme and mild highs to extreme lows. Symptoms of the extreme highs of bipolar disorder include abnormal or excessive elevation of behaviors, irritability, a decreased need to sleep, increased talking, racing thoughts, increased energy, poor judgment, and inappropriate social behavior. With extreme lows in bipolar disorder, the following characteristics may occur: depression, insomnia or hypersomnia, disinterest in activities, weight loss, loss of energy, feelings of worthlessness or guilt, inability to focus, and recurrent thoughts of death [35]. Taken as a whole, the above observations show that GCs are critical to overall mental health by regulating brain morphology and function, memory and learning, and psychological disorders such as PTSD and depression.
5. Memory and the Effects of Glucocorticoids
Glucocorticoid hormones influence the cognitive performance of individuals and can affect memory retention and an individual’s testing performance. Short-term and long-term memory are in different parts of the human brain. Short-term memory is located in the front part of the brain, known as the pre-frontal lobe. Short-term memory is transformed into long-term memory in the hippocampus, an area of the deeper part of the brain that has a high density of GRs [40]. The amygdala also plays a vital role in processing memory and emotional reaction, in social and sexual behaviors, and in regulating the sense of smell [40]. This area of the brain is an area that can grow new neurons but can also be impaired by stress-related GRs [41]. The way that GR affects memory depends on the basolateral complex of the amygdala (BLA) and the actions of GR in memory [42]. Not all elevated GCs are disruptive to memory. The acute form of stress typically adapts to the stress levels [43]. A study conducted by Roozendaal [44] showed that GCs and epinephrine influence memory retention by activating similar neural systems. The study showed a decline in memory retention with GCs when given shortly before retention testing. This effect is dependent on the noradrenergic activation of the BLA and the interchange of the BLA with other regions of the brain. With high circulating levels of GCs, memory retention can be hindered. When this occurs, memory retrieval may seem impaired for students. It has been suggested that this may favor memory consolidation, allowing a more pertinent response [44]. The study showed that the BLA is vital in memory retention that regulates stress and GCs’ effects on memory concentration and retrieval [44].
6. Effects of Anxiety on Cortisol Levels
A psychological stressor can activate the HPA axis. The HPA axis causes an increase in cortisol secretion to the adrenal cortex; this then leads to an increase in salivary cortisol [45]. When this occurs, an individual may have an increase in anxiety levels. Anxiety is defined in the DSM-5 as a disorder that can cause severe fears and stress-related behaviors. Anxiety disorders can be different in situations that can increase someone’s fear, anxiety, cognitive ideation, or avoidance behaviors. It is good to recognize what fear is causing the anxiety and then use strategies to help resolve it. The DSM-5 also states that anxiety disorders are typically developed in childhood and can worsen if not treated. Test anxiety may be present when the symptoms persist and are not attributable to the physiological effects of a substance/medication [35]. Substance abuse can alter the GR isoforms in the brain regions [46], which might cause an overall change in the HPA axis. However, this is yet to be tested, and more work in this area is needed.
A study completed by Tronche et al. showed that conditional mutation of GR in the nervous system provides genetic evidence for the importance of GR signaling in emotional behavior, because mutated animals showed an impaired behavioral response to stress and showed reduced anxiety [47]. Although restrained stress is not precisely “anxiety”, it can be viewed as extreme stress. However, more subtle increases in anxiety in animal models are non-existent. Such studies are hard to perform on animals. The study suggests that brain GR participates in the modification of anxiety-related behavior observed in the animal models. These mouse models will be of great value to address the role of GR in aspects of brain function such as learning and memory, drug dependence, and GC-dependent neurotoxicity associated with chronic stress [47].
7. Test Anxiety and Psychological Assessments: Accommodations as Treatments
It is important to know what strategies may help reduce test anxiety. During testing, teachers and professionals can provide accommodations in situations to help with test anxiety. Heiman and Precel shared accommodations for test anxiety that may assist students, which included: (1) providing extra time for the examination; (2) using copies of notes or an outline; (3) providing an alternate exam; (4) allowing the use of a computer; or (5) taking breaks. Together, these are all alternatives that can aid in the relief of anxiety that may ensue in an individual [48].
A study completed by Porrman, Mastorovich, and Gerwick shared some strategies to help reduce test anxiety during an exam. These included progressive relaxation to combat muscle tension. By relaxing the muscles, individuals can focus on the task they are working on [4,49]. Another suggestion that was described included the use of earplugs to help with aural distractions around the students [4,50]. The use of earplugs can help with noises such as student and teacher movements, shuffling of papers, and tapping of pencils [4].
Some other evidence-based strategies to help reduce test anxiety include cognitive behavior therapy (CBT), Interpersonal Therapy (IPT), dialectical behavior therapy (DBT), and eye movement desensitization and reprocessing (EMDR). CBT is a therapy used to help overcome an anxiety disorder. CBT focuses on the cognitive and behavioral aspects of anxiety. The concept behind CBT is to focus on one’s thoughts about a situation and determine how it affects the way one feels and how one behaves in that situation [51]. IPT is a time-limited treatment that focuses on individuals gaining control of their mood, typically lasting 12–16 months. The DPT strategy is a behavioral and problem-solving approach, blended with acceptance-based strategies and an emphasis on dialectical processes. The DBT strategy balances behavioral change, problem-solving, and emotional control with validation, mindfulness, and acceptance in patients [52]. EMDR therapy is not a traditional type of psychotherapy. Instead, it is usually used to treat post-traumatic stress disorder (PTSD). PTSD often occurs after traumatic experiences, such as military combat, physical assault, rape, or car accidents. EMDR uses a patient’s own rapid, rhythmic eye movements. Their eye movements dampen the power of emotionally charged memories of past traumatic events [53]. CBT seems to be the most widely used therapy for anxiety disorders in schools [51].
Ergene found that test anxiety is a serious problem for many children and adolescents attending elementary and secondary school [54]. Ergene’s study was conducted to test which test anxiety intervention approach works the best. The groups included cognitive interventions, cognitive-behavioral interventions, skill-focused approaches, behavioral and skill-focused techniques, cognitive and skill-focused treatments, and cognitive, behavioral, and skill-focused combined with techniques such as meditation or exercise [54]. Ergene used the following experimental groups: (1) 42 groups used cognitive interventions; (2) 17 groups used cognitive-behavioral interventions (3) 16 groups used a skill-focused approach; (4) 5 groups used behavioral and skill-focused techniques; (5) 3 groups used cognitive and skill-focused treatments, or cognitive, behavioral, and skill-focused, and (6) 7 groups used meditation or exercise [54]. Overall, Ergene’s study showed that psychological treatment was successful in reducing test anxiety.
8. Conclusions
Test anxiety is a significant factor contributing to lower academic performance and test scores. Developing an understanding of test anxiety in teachers, parents, scientists, clinicians, and professionals may help toward improving methods to help students cope during examinations and improve performance. Possible ways to help with test anxiety include providing accommodations in the classroom and coordinating with others to hold their tests in different environments. The student can also play a role in helping to reduce their test anxiety, as they can understand their stressors and then act to help cope with the stressors during an assessment. Although there is limited research on how test anxiety affects students with LD, there is anecdotal evidence that students with LD have higher test anxiety than students without LD. Gender differences in test anxiety have also been suggested, as females might be more willing to admit that they have anxiety compared to males. This could be a reason why the female-to-male ratio among those with test anxiety is two to one. Efforts can be made to encourage male students to improve their anxiety with proper accommodations. An individual with a disability may experience more difficulty during evaluative situations than students without any disabilities. Therefore, test anxiety needs to be taken into consideration on a per-child basis. These efforts will hopefully identify and improve adequate accommodations to improve test scores. Given the current dearth of information on how GCs affect test anxiety and performance in humans, this review will hopefully stimulate further investigation of this hypothesis, ultimately leading to better accommodations for test anxiety in all students.
Author Contributions
J.A.H. conceived the project. Figure 1 was commissioned from a graphical illustrator by the authors; J.A.H. created the illustration in Figure 2 using OmniGraffle. J.A.H. and E.R.S. wrote the manuscript and reviewed and revised the final manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the National Institutes of Health NIDDK grant R01DK121017 (E.R.S). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- National Mathematics Advisory Panel Foundations for Success: The Final Report of the National Mathematics Advisory Panel; U.S. Department of Education: Washington, DC, USA, 2008.
- Hu, Q.; Wu, Q.; Cheng, H. Investigation on test anxiety and coping style of middle school students in different nationalities. Creat. Educ. 2018, 9, 1071–1083. [Google Scholar] [CrossRef] [Green Version]
- Sari, S.A.; Bilek, G.; Celik, E. Test anxiety and self-esteem in senior high school students: A cross-sectional study. Nord. J. Psychiatry 2017, 72, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Poorman, S.G.; Mastorovich, M.L.; Gerwick, M. Interventions for test anxiety: How faculty can help. Teach. Learn. Nurs. 2019, 14, 186–191. [Google Scholar] [CrossRef]
- Sawka-Miller, K.D. Test anxiety. In Encyclopedia of Child Behavior and Development; Goldstein, S., Naglieri, J.A., Eds.; Springer: Boston, MA, USA, 2011; pp. 1478–1479. [Google Scholar] [CrossRef]
- Atasheneh, N.; Izadi, A. The role of teachers in reducing/increasing listening comprehension test anxiety: A case of Iranian EFL learners. Engl. Lang. Teach. 2012, 5, 178–187. [Google Scholar] [CrossRef] [Green Version]
- Embse, N.; Jester, D.; Roy, D.; Post, J. Test anxiety effects, predictors, and correlates: A 30-year meta-analytic review. J. Affect. Disord. 2018, 227, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Birenbaum, M.; Gutvirtz, Y. The relationship between test anxiety and seriousness of errors in algebra. J. Psychoeduc. Assess. 1993, 11, 12–19. [Google Scholar] [CrossRef]
- Farooqi, Y.N.; Ghani, R.; Spielberger, C.D. Gender differences in test anxiety and academic performance of medical students. Int. J. Psychol. Behav. Res. 2012, 2, 38–43. [Google Scholar]
- Duraku, Z.H.; Hoxha, L. Self-esteem, study skills, self-concept, social support, psychological distress, and coping mechanism effects on test anxiety and academic performance. Health Psychol. Open 2018, 5, 2055102918799963. [Google Scholar]
- Hembree, R. Correlates, causes, effects, and treatment of test anxiety. Rev. Educ. Res. 1988, 58, 47–77. [Google Scholar] [CrossRef]
- Zeidner, M. Test Anxiety: The State of the Art; Plenum Press: New York, NY, USA, 1998. [Google Scholar]
- Seipp, B. Anxiety and academic performance: A meta-analysis of findings. Anxiety Res. 1991, 4, 27–41. [Google Scholar] [CrossRef]
- Pekrun, R.; Goetz, T.; Titz, W. Academic emotions in students’ self-regulated learning and achievement: A program of qualitative and quantitative research. Educ. Psychol. 2002, 37, 91–105. [Google Scholar] [CrossRef]
- Methia, R.A. Help Your Child Overcome Test Anxiety and Achieve Higher Test Scores; Virtual Bookworm. Com Pub Incorporated: College Station, TX, USA, 2004. [Google Scholar]
- Smedlund, K.B.; Sanchez, E.R.; Hinds, T.D., Jr. FKBP51 and the molecular chaperoning of metabolism. Trends Endocrinol. Metab. 2021, 32, 862–874. [Google Scholar] [CrossRef] [PubMed]
- John, K.; Marino, J.S.; Sanchez, E.R.; Hinds, T.D., Jr. The glucocorticoid receptor: Cause of or cure for obesity? Am. J. Physiol. Endocrinol. Metab. 2016, 310, E249–E257. [Google Scholar] [CrossRef] [Green Version]
- Sherin, J.E.; Nemeroff, C.B. Post-traumatic stress disorder: The neurobiological impact of psychological trauma. Dialogues Clin. Neurosci. 2011, 13, 263–278. [Google Scholar]
- McEwen, B.S.; Sapolsky, R.M. Stress and cognitive function. Curr. Opin. Neurobiol. 1995, 5, 205–216. [Google Scholar] [CrossRef]
- Molina, P. Endocrine Physiology, 3rd ed.; McGraw-Hill Companies: New York, NY, USA, 2010; p. 301. [Google Scholar]
- Doga, M.; Bonadonna, S.; Giustina, A. Glucocorticoids and bone: Cellular, metabolic and endocrine effects. Hormones 2004, 3, 184–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashwell, J.D.; Lu, F.W.; Vacchio, M.S. Glucocorticoids in T cell development and function*. Annu. Rev. Immunol. 2000, 18, 309–345. [Google Scholar] [CrossRef]
- Kaplan, N. The adrenal glands. In Textbook of Endocrine Physiology, 2nd ed.; Griffin, J.E., Ojeda, S.R., Eds.; Oxford University Press: Oxford, UK, 1992; pp. 247–275. [Google Scholar]
- Caron, S.; Staels, B. Apolipoprotein CIII: A link between hypertriglyceridemia and vascular dysfunction? Circ. Res. 2008, 103, 1348–1350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adrenal Insufficiency and Addison’s Disease. Available online: https://www.niddk.nih.gov/health-information/endocrine-diseases/adrenal-insufficiency-addisons-disease (accessed on 20 January 2022).
- Hinds, T.D., Jr.; Sanchez, E.R. Protein phosphatase 5. Int. J. Biochem. Cell Biol. 2008, 40, 2358–2362. [Google Scholar] [CrossRef] [PubMed]
- Goosens, K.A.; Sapolsky, R.M. Stress and glucocorticoid contributions to normal and pathological aging. In Brain Aging: Models, Methods, and Mechanisms; Taylor & Francis Group, LLC: Boca Raton, FL, USA, 2007. [Google Scholar]
- Peffer, M.E.; Zhang, J.Y.; Umfrey, L.; Rudine, A.C.; Monaghan, A.P.; DeFranco, D.B. Minireview: The impact of antenatal therapeutic synthetic glucocorticoids on the developing fetal brain. Mol. Endocrinol. 2015, 29, 658–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Quervain, D.J.; Aerni, A.; Schelling, G.; Roozendaal, B. Glucocorticoids and the regulation of memory in health and disease. Front. Neuroendocrinol. 2009, 30, 358–370. [Google Scholar] [CrossRef] [PubMed]
- De Quervain, D.; Roozendaal, B.; McGaugh, J.L. Stress and glucocorticoids impair retrieval of long-term spatial memory. Nature 1998, 394, 787–790. [Google Scholar] [CrossRef] [PubMed]
- Wolkowitz, O.M.; Epel, E.S.; Reus, V.I. Stress hormone-related psychopathology: Pathophysiological and treatment implications. World J. Biol. Psychiatry 2001, 2, 115–143. [Google Scholar] [CrossRef] [PubMed]
- Holtzman, C.W.; Trotman, H.D.; Goulding, S.M.; Ryan, A.T.; Macdonald, A.N.; Shapiro, D.I.; Brasfield, J.L.; Walker, E.F. Stress and neurodevelopmental processes in the emergence of psychosis. Neuroscience 2013, 249, 172–191. [Google Scholar] [CrossRef] [Green Version]
- Sapolsky, R.M. Why stress is bad for your brain. Science 1996, 273, 749–750. [Google Scholar] [CrossRef]
- Jia, M.; Smerin, S.E.; Zhang, L.; Xing, G.; Li, X.; Benedek, D.; Ursano, R.; Li, H. Corticosterone mitigates the stress response in an animal model of PTSD. J. Psychiatr. Res. 2015, 60, 29–39. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Krishnan, V.; Nestler, E.J. The molecular neurobiology of depression. Nature 2008, 455, 894–902. [Google Scholar] [CrossRef]
- Burden of Mental And Behavioural Disorder; World Health Organization: Geneva, Switzerland, 2001; pp. 20–46. Available online: https://www.who.int/whr/2001/en/whr01_en.pdf (accessed on 20 January 2022).
- Anacker, C.; Zunszain, P.A.; Carvalho, L.A.; Pariante, C.M. The glucocorticoid receptor: Pivot of depression and of antidepressant treatment? Psychoneuroendocrinology 2011, 36, 415–425. [Google Scholar] [CrossRef] [Green Version]
- Parmenon, C.; Guillard, J.; Caignard, D.H.; Hennuyer, N.; Staels, B.; Audinot-Bouchez, V.; Boutin, J.A.; Dacquet, C.; Ktorza, A.; Viaud-Massuard, M.C. 4,4-Dimethyl-1,2,3,4-tetrahydroquinoline-based PPARalpha/gamma agonists. Part. II: Synthesis and pharmacological evaluation of oxime and acidic head group structural variations. Bioorganic Med. Chem. Lett. 2009, 19, 2683–2687. [Google Scholar] [CrossRef]
- Ashford, M. How are Memories Stored in the Brain. Available online: http://www.livescience.com/32798-how-are-memories-stored-in-the-brain.html (accessed on 20 January 2022).
- Mastin, L. Parts of the Brain. Available online: https://human-memory.net/parts-of-the-brain/ (accessed on 29 January 2022).
- McGaugh, J.L.; Roozendaal, B. Role of adrenal stress hormones in forming lasting memories in the brain. Neurobiology 2002, 12, 205–210. [Google Scholar] [CrossRef]
- Wolf, O.T. Stress and memory in humans: Twelve years of progress? Brain Res. 2009, 1293, 142–154. [Google Scholar] [CrossRef] [PubMed]
- Roozendaal, B. Stress and memory: Opposing effects of glucocorticoids on memory consolidation and memory retrieval. Neurobiol. Learn. Mem. 2002, 78, 578–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takai, N.; Yamaguchi, M.; Aragaki, T.; Eto, K.; Uchihashi, K.; Nishikawa, Y. Effect of psychological stress on the salivary cortisol and amylase levels in healthy young adults. Arch. Oral Biol. 2004, 49, 963–968. [Google Scholar] [CrossRef] [PubMed]
- Alhaddad, H.; Gordon, D.M.; Bell, R.L.; Jarvis, E.E.; Kipp, Z.A.; Hinds, T.D., Jr.; Sari, Y. Chronic ethanol consumption alters glucocorticoid receptor isoform expression in stress neurocircuits and mesocorticolimbic brain regions of alcohol-preferring rats. Neuroscience 2020, 437, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Tronche, F.; Kellendonk, C.; Kretz, O.; Gass, P.; Anlag, K.; Orban, P.C.; Bock, R.; Klein, R.; Schutz, G. Disruption of the glucocorticoid receptor gene in the nervous system results in reduced anxiety. Nat. Genet. 1999, 23, 99–103. [Google Scholar] [CrossRef]
- Heiman, T.; Precel, K. Students with learning disabilities in higher education: Academic strategies profile. J. Learn. Disabil. 2003, 36, 248–258. [Google Scholar] [CrossRef] [Green Version]
- Zargarzadeh, M.; Shirazi, M. The effect of progressive muscle relaxation method on test anxiety in nursing students. Iran J. Nurs. Midwifery 2014, 19, 607. [Google Scholar]
- Killu, K.; Crundwell, M.A. Students with anxiety in the classroom: Educational accommodations and interventions. Beyond Behav. 2016, 25, 30–40. [Google Scholar] [CrossRef]
- More on CBT. Available online: http://www.anxietybc.com/help-resources/cbt/more-on-cbt (accessed on 7 July 2015).
- Dialectical Behavior Therapy. Available online: http://www.nrepp.samhsa.gov/ViewIntervention.aspx?id=36 (accessed on 30 July 2020).
- Eye Movement Desensitization and Reprocessing. Available online: http://www.nrepp.samhsa.gov/ViewIntervention.aspx?id=199 (accessed on 30 July 2020).
- Ergene, T. Effective interventions on test anxiety reduction: A meta-analysis. Sch. Psychol. Int. 2003, 24, 313–328. [Google Scholar] [CrossRef]
Figure 1.
Stress Response in the Human Body. In response to stress, cerebral cortex signaling stimulates the hypothalamus to release corticotropin-releasing hormone (CRH). In turn, CRH stimulates the pituitary gland to produce and release adrenocorticotropic hormone (ACTH) into the blood. ACTH then activates pathways in the adrenal glands for the synthesis and release of the stress hormone cortisol. As a consequence of chronic stress, such as repeated test anxiety, over-stimulation by cortisol can lead to the indicated deleterious side effects in the brain and central nervous system.
Figure 1.
Stress Response in the Human Body. In response to stress, cerebral cortex signaling stimulates the hypothalamus to release corticotropin-releasing hormone (CRH). In turn, CRH stimulates the pituitary gland to produce and release adrenocorticotropic hormone (ACTH) into the blood. ACTH then activates pathways in the adrenal glands for the synthesis and release of the stress hormone cortisol. As a consequence of chronic stress, such as repeated test anxiety, over-stimulation by cortisol can lead to the indicated deleterious side effects in the brain and central nervous system.

Figure 2.
Cellular Response to Stress. Glucocorticoid hormones (cortisol) enter through the cell membrane to bind the glucocorticoid receptor (GR) in the cytoplasm. Cortisol-bound GR then moves to the nucleus to regulate gene expression by binding to glucocorticoid response elements (GREs) in the regulatory regions of select target genes. This signaling mechanism determines how each person responds physiologically to stress.
Figure 2.
Cellular Response to Stress. Glucocorticoid hormones (cortisol) enter through the cell membrane to bind the glucocorticoid receptor (GR) in the cytoplasm. Cortisol-bound GR then moves to the nucleus to regulate gene expression by binding to glucocorticoid response elements (GREs) in the regulatory regions of select target genes. This signaling mechanism determines how each person responds physiologically to stress.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Hinds, J.A.; Sanchez, E.R. The Role of the Hypothalamus–Pituitary–Adrenal (HPA) Axis in Test-Induced Anxiety: Assessments, Physiological Responses, and Molecular Details. Stresses 2022, 2, 146-155. https://doi.org/10.3390/stresses2010011
AMA Style
Hinds JA, Sanchez ER. The Role of the Hypothalamus–Pituitary–Adrenal (HPA) Axis in Test-Induced Anxiety: Assessments, Physiological Responses, and Molecular Details. Stresses. 2022; 2(1):146-155. https://doi.org/10.3390/stresses2010011
Chicago/Turabian StyleHinds, Jenalee A., and Edwin R. Sanchez. 2022. "The Role of the Hypothalamus–Pituitary–Adrenal (HPA) Axis in Test-Induced Anxiety: Assessments, Physiological Responses, and Molecular Details" Stresses 2, no. 1: 146-155. https://doi.org/10.3390/stresses2010011