
The Working Informal Caregiver Model: A Mixed Methods Approach to Explore Future Informal Caregiving by Working Caregivers

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Context of the Dutch Long-Term Care System and Support for Informal Caregivers
2.2. Process of Developing the Working Informal Caregiver Model
- Step 1: Literature review
- Step 2: Group Model Building exercise
- Step 3: Delphi study
- Step 3A: Round 1 of the Delphi study
- Step 3B: Round 2 of the Delphi study
3. Results
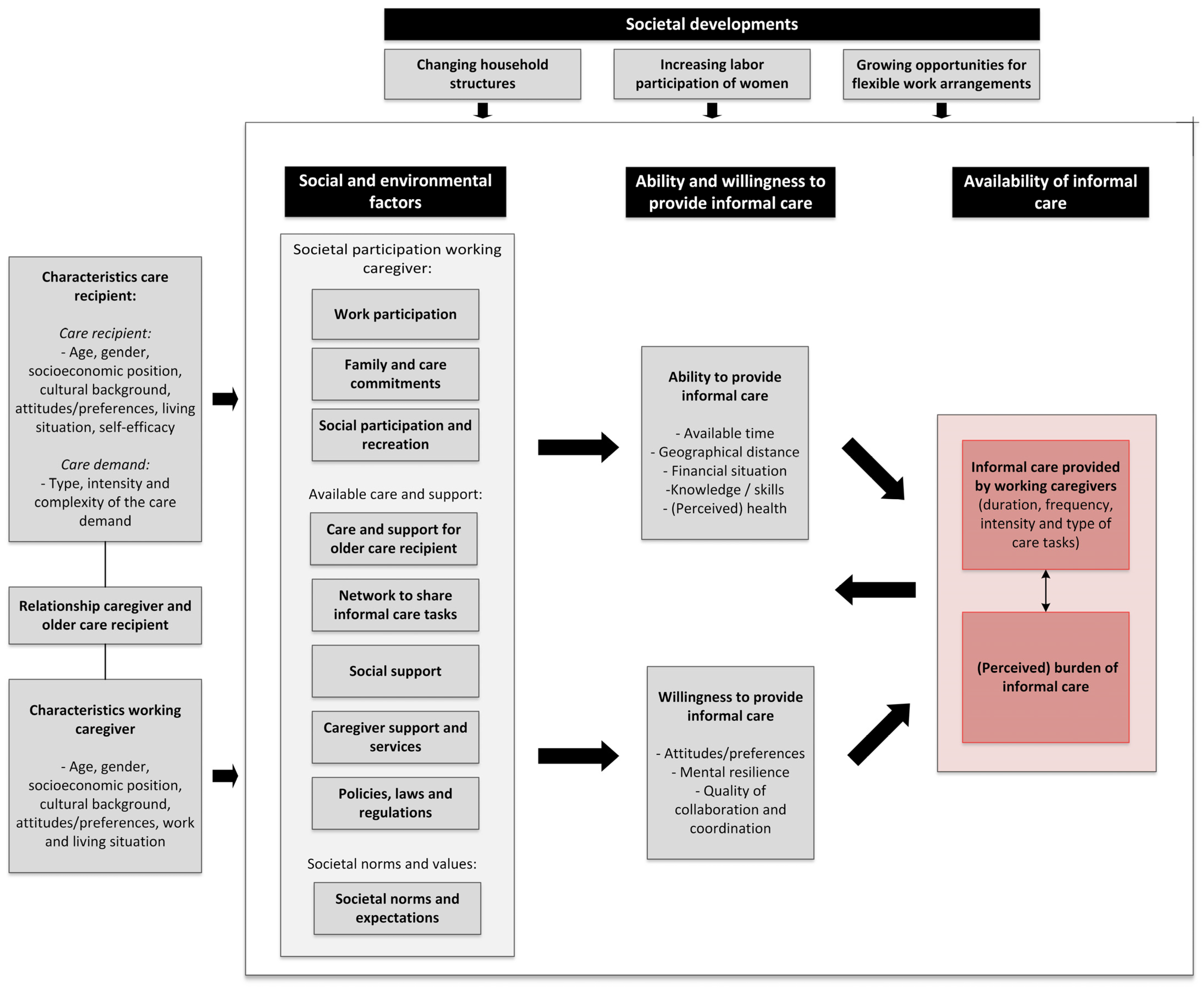
3.1. Explanation of the WIC Model
3.1.1. Social and Environmental Factors
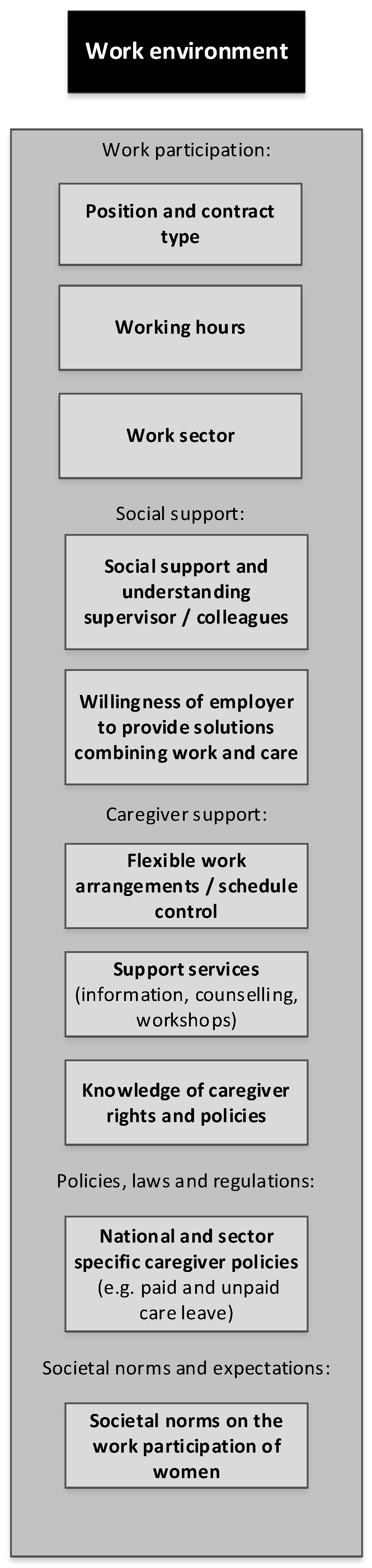
Work-Related Environmental Factors in Detail
3.1.2. Ability and Willingness to Provide Care
Ability Factors
Willingness Factors
3.2. Impactful Societal Developments Influencing the Future Availability of Informal Care
4. Discussion
4.1. The Added Value of the WIC Model
4.2. Applicability of the WIC Model
4.3. Reflections on the Development Process
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Uhlenberg, P. (Ed.) International Handbook of Population Aging; Springer: Dordrecht, The Netherlands, 2009; Volume 1. [Google Scholar]
- World Health Organization. The Growing Need for Home Health Care for the Elderly: Home Health Care for the Elderly as an Integral Part of Primary Health Care Services; Regional Office for the Eastern Mediterranean: Cairo, Egypt, 2015. [Google Scholar]
- Eurostat. Ageing Europe. Looking at the Lives of Older People in the EU; European Commission: Luxembourg, 2019. [Google Scholar]
- Mulliner, E.; Riley, M.; Maliene, V. Older people’s preferences for housing and environment characteristics. Sustainability 2020, 12, 5723. [Google Scholar] [CrossRef]
- Triantafillou, J.; Naiditch, M.; Repkova, K.; Stiehr, K.; Carretero, S.; Emilsson, T.; Di Santo, P.; Bednarik, R.; Brichtova, L.; Ceruzzi, F.; et al. Informal Care in the Long-Term Care System European Overview Paper; European Centre for Social Welfare Policy and Research: Athens, Greece; Vienna, Austria, 2010. [Google Scholar]
- de Boer, A.; Plaisier, I.; de Klerk, M. Werk en Mantelzorg Kwaliteit van Leven en Het Gebruik van Ondersteuning op Het Werk. [Work and Informal Care. Quality of Life and the Use of Support in the Workplace]; The Netherlands Institute for Social Research: The Hague, The Netherlands, 2019. [Google Scholar]
- de Klerk, M.; de Boer, A.; Plaisier, I.; Schyns, P.; Kooiker, S. Informele Hulp: Wie Doet Er Wat? Omvang, Aard en Kenmerken van mAntelzorg en Vrijwilligerswerk in de Zorg en Ondersteuning in 2014 [Informal Care: Who Does What? Volume, Type and Characteristics of Informal Care and Volunteering in 2014]; The Netherlands Institute for Social Research: The Hague, The Netherlands, 2015. [Google Scholar]
- Broese van Groenou, M.I.; De Boer, A. Providing informal care in a changing society. Eur. J. Ageing 2016, 13, 271–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cross, A.J.; Garip, G.; Sheffield, D. The psychosocial impact of caregiving in dementia and quality of life: A systematic review and meta-synthesis of qualitative research. Psychol. Health 2018, 33, 1321–1342. [Google Scholar] [CrossRef] [PubMed]
- Walker, A.J.; Pratt, C.C.; Eddy, L. Informal caregiving to aging family members: A critical review. Fam. Relat. 1995, 44, 402–411. [Google Scholar] [CrossRef]
- Zuba, M.; Schneider, U. What helps working informal caregivers? The role of workplace characteristics in balancing work and adult-care responsibilities. J. Fam. Econ. Issues 2013, 34, 460–469. [Google Scholar] [CrossRef]
- Bauer, J.M.; Sousa-Poza, A. Impacts of informal caregiving on caregiver employment, health, and family. J. Popul. Ageing 2015, 8, 113–145. [Google Scholar] [CrossRef] [Green Version]
- Grzywacz, J.G.; Marks, N.F. Reconceptualizing the work-family interface: An ecological perspective on the correlates of positive and negative spillover between work and family. J. Occup. Health Psychol. 2000, 5, 111–126. [Google Scholar] [CrossRef]
- Wittenberg, Y.; Kwekkeboom, R.; Staaks, J.; Verhoeff, A.; de Boer, A. Informal caregivers’ views on the division of responsibilities between themselves and professionals: A scoping review. Health Soc. Care Community 2018, 26, 460–473. [Google Scholar] [CrossRef] [PubMed]
- Schulz, R.; Sherwood, P.R. Physical and mental health effects of family caregiving. Am. J. Nurs. 2008, 108, 23–27. [Google Scholar] [CrossRef]
- Kraijo, H.; Brouwer, W.; de Leeuw, R.; Schrijvers, G.; van Exel, J. The perseverance time of informal carers of dementia patients: Validation of a new measure to initiate transition of care at home to nursing home care. J. Alzheimers Dis. 2014, 40, 631–642. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, F.R.; Michel, J.P.; Robine, J.M. Worldwide decline in the oldest old support ratio. Eur. Geriatr. Med. 2010, 1, 3–8. [Google Scholar] [CrossRef]
- De Koker, B. Socio-demographic determinants of informal caregiving: Co-resident versus extra-resident care. Eur. J. Ageing 2009, 6, 3–15. [Google Scholar] [CrossRef] [Green Version]
- Pickard, L. A growing care gap? The supply of unpaid care for older people by their adult children in England to 2032. Ageing Soc. 2015, 35, 96–123. [Google Scholar] [CrossRef] [Green Version]
- Geerts, J.; Willeme, P.; Mot, E. Long-Term Care Use and Supply in Europe: Projection Models and Results for Germany, the Netherlands, Spain and Poland. ENEPRI Research Report No. 116; European Network of Economic Policy Research Institutes. 2012. Available online: https://ssrn.com/abstract=2060145 (accessed on 1 January 2022).
- Mentzakis, E.; McNamee, P.; Ryan, M. Who cares and how much: Exploring the determinants of co-residential informal care. Rev. Econ. Househ. 2009, 7, 283–303. [Google Scholar] [CrossRef]
- Zigante, V. Informal Care in Europe. Exploring Formalisation, Availability and Quality; Directorate-General for Employment, Social Affairs and Inclusion, European Commission: Brussels, Belgium, 2018. [Google Scholar]
- Wittenberg, R.; Pickard, L.; Comas-Herrera, A.; Davies, B.D.; Darton, R. Demand for Long-Term Care: Projections of Long-Term Care Finance for Elderly People; The university of Kent: Canterbury, UK, 1998. [Google Scholar]
- Pearlin, L.I.; Mullan, J.T.; Semple, S.J.; Skaff, M.M. Caregiving and the stress process: An overview of concepts and their measures. Gerontologist 1990, 30, 583–594. [Google Scholar] [CrossRef] [PubMed]
- Gérain, P.; Zech, E. Informal caregiver burnout? Development of a theoretical framework to understand the impact of caregiving. Front. Psychol. 2019, 10, 1748. [Google Scholar] [CrossRef] [Green Version]
- Chou, K.-R. Caregiver burden: A concept analysis. J. Pediatr. Nurs. 2000, 15, 398–407. [Google Scholar] [CrossRef]
- Lindt, N.; van Berkel, J.; Mulder, B.C. Determinants of overburdening among informal carers: A systematic review. BMC Geriatr. 2020, 20, 304. [Google Scholar] [CrossRef]
- de Boer, A.; van Groenou, M.B.; Keuzenkamp, S. Belasting van werkende mantelzorgers [Burden of working caregivers]. TSG 2010, 88, 313–319. [Google Scholar] [CrossRef]
- Calvano, L. Tug of war: Caring for our elders while remaining productive at work. Acad. Manag. Perspect. 2013, 27, 204–218. [Google Scholar] [CrossRef]
- Clancy, R.L.; Fisher, G.G.; Daigle, K.L.; Henle, C.A.; McCarthy, J.; Fruhauf, C.A. Eldercare and work among informal caregivers: A multidisciplinary review and recommendations for future research. J. Bus. Psychol. 2020, 35, 9–27. [Google Scholar] [CrossRef]
- Börjeson, L.; Höjer, M.; Dreborg, K.-H.; Ekvall, T.; Finnveden, G. Scenario types and techniques: Towards a user’s guide. Futures 2006, 38, 723–739. [Google Scholar] [CrossRef]
- Kroneman, M.; Boerma, W.; van den Berg, M.; Groenewegen, P.; de Jong, J.; van Ginneken, E. Netherlands: Health System Review; European Observatory on Health Systems and Policies: Brussels, Belgium, 2016. [Google Scholar]
- de Boer, A.; de Klerk, M.; Verbeek-Oudijk, D.; Plaisier, I. Blijvende Bron van Zorg. Ontwikkelingen in Het Geven van Informele Hulp 2014–2019 [Ongoing Source of Care. Trends in the Provision of Informal Help from 2014 to 2019]; The Netherlands Institute for Social Research: The Hague, The Netherlands, 2020. [Google Scholar]
- Hasson, F.; Keeney, S.; McKenna, H. Research guidelines for the Delphi survey technique. J. Adv. Nurs. 2000, 32, 1008–1015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelitz, M.A.; Beardmore, B.; Machtans, C.S.; Hall, A.W.; Wedeles, C. Addressing complexity and uncertainty: Conceptual models and expert judgments applied to migratory birds in the oil sands of Canada. Ecol. Soc. 2015, 20, 1–46. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, B.; Svedin, U.; Wittrock, B. Methods in Futures Studies: Problems and Applications; Westview Press: Boulder, CO, USA, 1982. [Google Scholar]
- Lembani, M.; de Pinho, H.; Delobelle, P.; Zarowsky, C.; Mathole, T.; Ager, A. A Guide for Participatory Systems Analysis Using a Group Model Building Approach; SAGE Research Methods Cases; SAGE Publications Ltd.: London, UK, 2020. [Google Scholar] [CrossRef]
- Siokou, C.; Morgan, R.; Shiell, A. Group model building: A participatory approach to understanding and acting on systems. Public Health Res. Pract. 2014, 25, e2511404. [Google Scholar] [CrossRef] [Green Version]
- Keeney, S.; Hasson, F.; McKenna, H. The Delphi Technique in Nursing and Health Research; Wiley-Blackwell: Chichester, UK, 2011. [Google Scholar]
- Dahlgren, G.; Whitehead, M. Policies and Strategies to Promote Social Equity in Health; Institute for Futures Studies: Stockholm, Sweden, 1991. [Google Scholar]
- Babitsch, B.; Gohl, D.; von Lengerke, T. Re-revisiting Andersen’s Behavioral Model of Health Services Use: A systematic review of studies from 1998–2011. GMS Psycho Soc. Med. 2012, 9, 1–15. [Google Scholar] [CrossRef]
- Andersen, R.; Newman, J.F. Societal and Individual Determinants of Medical Care Utilization in the United States. Milbank Q. 2005, 83, 95–124. [Google Scholar] [CrossRef]
- Grembowski, D.; Patrick, D.; Diehr, P.; Durham, M.; Beresford, S.; Kay, E.; Hecht, J. Self-Efficacy and health behavior among older adults. J. Health Soc. Behav. 1993, 34, 89–104. [Google Scholar] [CrossRef] [PubMed]
- de Klerk, M.; de Boer, A.; Plaisier, I. Determinants of informal care-giving in various social relationships in the Netherlands. Health Soc. Care Community 2021, 29, 1779–1788. [Google Scholar] [CrossRef]
- Arksey, H.; Kemp, P.; Glendinning, C.; Kotchetkova, I.; Tozer, R. Carers’ Aspirations and Decisions around Work and Retirement. Research Report 290; Department for Work and Pensions, University of York: Leeds, UK, 2005. [Google Scholar]
- Bohlmann, C.; Zacher, H. Supporting employees with caregiving responsibilities. In Creating Psychologically Healthy Workplaces; Burke, R.J., Richardsen, A.M., Eds.; Edward Elgar Publishing Limited: Cheltenham, UK, 2019; pp. 431–451. [Google Scholar]
- Ireson, R.; Sethi, B.; Williams, A. Availability of caregiver-friendly workplace policies (CFWPs): An international scoping review. Health Soc. Care Community 2018, 26, e1–e14. [Google Scholar] [CrossRef]
- Rindfuss, R.R.; Brewster, K.L.; Kavee, A.L. Women, work, and children: Behavioral and attitudinal change in the United States. Popul. Dev. Rev. 1996, 22, 457–482. [Google Scholar] [CrossRef]
- Schmidt, A.E.; Ilinca, S.; Schulmann, K.; Rodrigues, R.; Principi, A.; Barbabella, F.; Sowa, A.; Golinowska, S.; Deeg, D.; Galenkamp, H. Fit for caring: Factors associated with informal care provision by older caregivers with and without multimorbidity. Eur. J. Ageing 2016, 13, 103–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Beer, P. De Arbeidsmarkt in 2040: Ingrijpende Veranderingen, Maar Ook Veel Continuïteit [The Labor Market in 2040: Far-Reaching Changes, but Also Continuity]; Amsterdam Institute for Advanced Labour Studies: Amsterdam, The Netherlands, 2016. [Google Scholar]
- van Echtelt, P.; Croezen, S.; Vlasblom, J.D.; de Voogd-Hamelink, M. Aanbod van Arbeid. Werken, Zorgen en Leren op een Flexibele Arbeidsmarkt [Supply of Labor. Working, Caring and Learning in a Flexible Labor Market]; The Netherlands Institute for Social Research: The Hague, The Netherlands, 2016. [Google Scholar]
- Gigauri, I. Effects of COVID-19 on Human Resource Management from the perspective of digitilization and work-life balance. Int. J. Innov. Technol. 2020, 31, 1–10. [Google Scholar] [CrossRef]
- Van Soest, A.; Ciccarelli, N. Mantelzorg, Arbeidsparticipatie en Gezondheid [Informal Care, Labor Participation and Health]; Tilburg University, The Netherlands: Tilburg, The Netherlands, 2016. [Google Scholar]
- Josten, E.; de Boer, A. Concurrentie Tussen Mantelzorg en Betaald Werk [Competition between Informal Care and Paid Work]; The Netherlands Institute for Social Research: The Hague, The Netherlands, 2015. [Google Scholar]
- The Netherlands Institute for Social Research. Veranderde Zorg en Ondersteuning Voor Mensen Met een Beperking. Landelijke Evaluatie van de Hervorming Langdurige Zorg [Changing Care and Support for Persons with Limitations]; The Netherlands Institute for Social Research: The Hague, The Netherlands, 2017. [Google Scholar]
- Social and Economic Council of the Netherlands. Een Werkende Combinatie. Advies over het Combineren van Werken, Leren en Zorgen in de Toekomst. [A Working Combination. Advice on Combining Work, Education and Care in the Future]; Social and Economic Council of the Netherlands: The Hague, The Netherlands, 2016. [Google Scholar]
- Martin, T.; Burgman, M.; Fidler, F.; Kuhnert, P.; Low-Choy, S.; McBride, M.; Mengersen, K. Eliciting expert knowledge in conservation science. Conserv. Biol. 2012, 26, 29–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Bruggen, A.; Nikolic, I.; Kwakkel, J. Modeling with Stakeholders for Transformative Change. Sustainability 2019, 11, 825. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Social and Environmental Factors (e.g., Social Environment, Family, Community, Work, Formal and Informal Care Environment, Policy Environment) | |
| Societal participation of working caregiver | |
| Work participation | The employment status of the (intended) caregiver, such as position, contract type, work hours and work sector. |
| Family and care commitments | Other care tasks of the caregiver, such as family commitments or pre-existing informal care or volunteering tasks. |
| Social participation and recreation | Social and recreational activities of the caregiver, such as social visits, club activities, religious activities, sports and hobbies. |
| Available care and support | |
| Care and support for older care recipient | Available public, private, formal and informal amenities, care and (technological) support for the older care recipient, which can vary locally. Within formal care organizations, the attention paid to caregivers’ roles is also important. |
| Network to share informal care tasks | Opportunities for the caregiver to share informal care tasks within his or her social network, family or with volunteers. This may depend on the size, composition, task distribution and quality of relationships within the social and family networks. |
| Social support | The (emotional) support and understanding that the caregiver receives from his or her social environment (family, friends), the care environment (other formal or informal caregivers), and work environment (employer, supervisor, colleagues). |
| Caregiver support and services | Available private and public caregiver support options in different settings, such as at home (e.g., technological support to assist in the care for the older adult, domestic help), in the community (e.g., respite care, support meetings), at work (e.g., flexible work arrangements, care leave, technological infrastructure to work from home) and in general (e.g., available information for caregivers). |
| Policies, laws and regulations | Policies, laws and (fiscal) regulations at the municipal, national or collective labor agreement level that may hinder or promote informal care by workers, such as care leave, entitlements to care and support for older adults, and the retirement age. |
| Societal norms and values | |
| Societal norms and expectations | Societal norms and expectations that may influence the extent to which a caregiver prefers, or feels ‘obligated’ to provide informal care (e.g., norms about gender and having a caring role, and about the responsibility of the state versus personal responsibility to provide support for older adults). |
| Factors Related to Ability and Willingness to Provide Informal Care | |
| Ability to provide informal care | |
| Available time | The available amount of time that could be spent on informal care according to the intended caregiver. |
| Geographical distance | The geographical distance and travel time between the (workplace of the) caregiver and the care recipient. |
| Financial situation | The caregiver’s ability to bear the financial costs associated with the care tasks, to outsource certain care tasks (e.g., to private care), or to reduce working hours in order to provide informal care. |
| Knowledge/skills | Knowledge and skills that may help the caregiver to fulfil the informal care role, such as medical or digital skills, or knowledge about the care and support system. |
| (Perceived) health | The caregiver’s assessment of his or her own health, based on the presence of health afflictions, but also lifestyle and psychosocial factors. |
| Willingness to provide care | |
| Attitudes/preferences | The extent to which the caregiver prefers to provide informal care, and how he or she feels about it, depending on the individual’s motives, norms, values and on societal norms and expectations. |
| Mental resilience | The extent to which the caregiver is able to cope with challenges and changes related to the informal care situation, to adapt to it and maintain it. |
| Quality of collaboration and coordination | The quality of collaboration and coordination between the caregiver and the older care recipient, other informal caregivers, volunteers, or health and social care professionals. |
| Availability Related Outcomes for the Working Caregiver | |
| Informal care provided | The level of engagement in informal care provision by workers: duration, frequency and intensity of the provided care and the type of informal care tasks. |
| (Perceived) burden of informal care | The burden that is experienced by the caregiver due to the informal care tasks, determined by the objective burden (frequency, duration and intensity of care) and how the provision of care is perceived by the person itself. The experience of burden may influence the amount of provided care and the amount of time that a caregiver can maintain their caregiving role. |
| Work Participation | |
|---|---|
| Position and contract type | The job position and contract type of the caregiver (e.g., self-employed, salaried, flexible contract). |
| Working hours | The number of working hours per week. |
| Work sector | The work sector in which the caregiver works, including the existence of collective labor agreements with policies aimed at caregivers. |
| Social Support at Work | |
| Social support and understanding at work | The extent to which the caregiver feels safe to share his or her care situation, and feels (emotionally) supported and understood by the employer, supervisors and/or colleagues. |
| Employer’s willingness to offer solutions combining work and care | The extent to which the employer, supervisors and/or colleagues are willing to find and offer solutions that help the caregiver combine work and care. |
| Caregiver Support at Work | |
| Flexible work arrangements and schedule control | Agreements between employer and caregiver to help the caregiver combine work and care, such as workload adaptations, schedule control, the ability to work outside the office and to choose their own working hours. |
| Support services | Support services provided by the employer, such as information for employed caregivers or supervisors, counselling, caregiver meetings or ICT support that enables working remotely. |
| Knowledge of caregiver rights and policies | The extent to which employers and employees are aware and knowledgeable of existing rights and policies for employed caregivers. |
| Work Policies, Laws and Regulations | |
| National and sector specific caregiver policies | The existence of policies and regulation for working caregivers at the national level or in collective labor agreements, such as the Work and Care Act, the retirement age or fiscal/tax regulations. |
| Societal Norms and Expectations | |
| Societal norms on the work participation of women | Changing norms and expectations, where women are increasingly expected to participate (more) in the workforce. |
| Rank | Societal Developments | Points * |
|---|---|---|
| 1 | Declining birth rates contribute to households becoming relatively smaller, and there is an increase in the number of single-person households. As a result, opportunities for (potential) caregivers to share care within their households or families diminish. | 39 |
| 2 | Rising workforce participation rates, in particular among women, result in more caregivers combining work and care | 34 |
| 3 | Growing flexibility for workers in some sectors in terms of contract types, schedule control, part-time work and options to work from home, increase working caregivers’ ability to provide care | 26 |
| 4 | A decline in the number of caregivers in relation to the number of older care recipients, due to demographic changes | 16 |
| 5 | Changing societal norms where people are increasingly expected to take on multiple societal roles at once (e.g., caregiving, volunteering, maintaining many social relationships) | 15 |
| 6 | Emerging innovations and increasing options in the public and private sector to support informal caregivers, such as technology or other services | 12 |
| 7 | The emergence of more complex family structures (e.g., blended families, divorces) may affect “obvious” care roles and responsibilities of potential caregivers, but increase care network size | 8 |
| 7 | Due to ongoing emancipation processes, gendered role expectations of women as “obvious” caregivers are expected to decrease, while for men, the negative image of caregiving roles also decreases | 8 |
| 8 | Rising retirement ages result in caregivers combining work and care for a longer time and until a higher age | 6 |
| 8 | Fluctuations in economy and labor markets create financial uncertainty which may impede informal caregivers from exchanging work for providing informal care | 6 |
| 9 | Changing norms about the responsibility of the immediate social environment to provide care to older adults with care needs | 4 |
| - | The education and prosperity level of the general population, and therefore also caregivers, continues to increase | 0 |
| - | The share of self-employed caregivers in the working population is increasing, which may help the combination of work and care | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vos, E.E.; Hilderink, H.B.M.; de Bruin, S.R.; van der Beek, A.J.; Proper, K.I. The Working Informal Caregiver Model: A Mixed Methods Approach to Explore Future Informal Caregiving by Working Caregivers. Sustainability 2022, 14, 3519. https://doi.org/10.3390/su14063519
Vos EE, Hilderink HBM, de Bruin SR, van der Beek AJ, Proper KI. The Working Informal Caregiver Model: A Mixed Methods Approach to Explore Future Informal Caregiving by Working Caregivers. Sustainability. 2022; 14(6):3519. https://doi.org/10.3390/su14063519
Chicago/Turabian StyleVos, Eline E., Henk B. M. Hilderink, Simone R. de Bruin, Allard J. van der Beek, and Karin I. Proper. 2022. "The Working Informal Caregiver Model: A Mixed Methods Approach to Explore Future Informal Caregiving by Working Caregivers" Sustainability 14, no. 6: 3519. https://doi.org/10.3390/su14063519