Multidimensional Effectiveness of Botulinum Toxin in Neuropathic Pain: A Systematic Review of Randomized Clinical Trials

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. BoNT Intervention
2.2. Main Findings
2.2.1. Primary Outcome-Multidimensional Pain Assessment
2.2.2. Secondary Outcomes
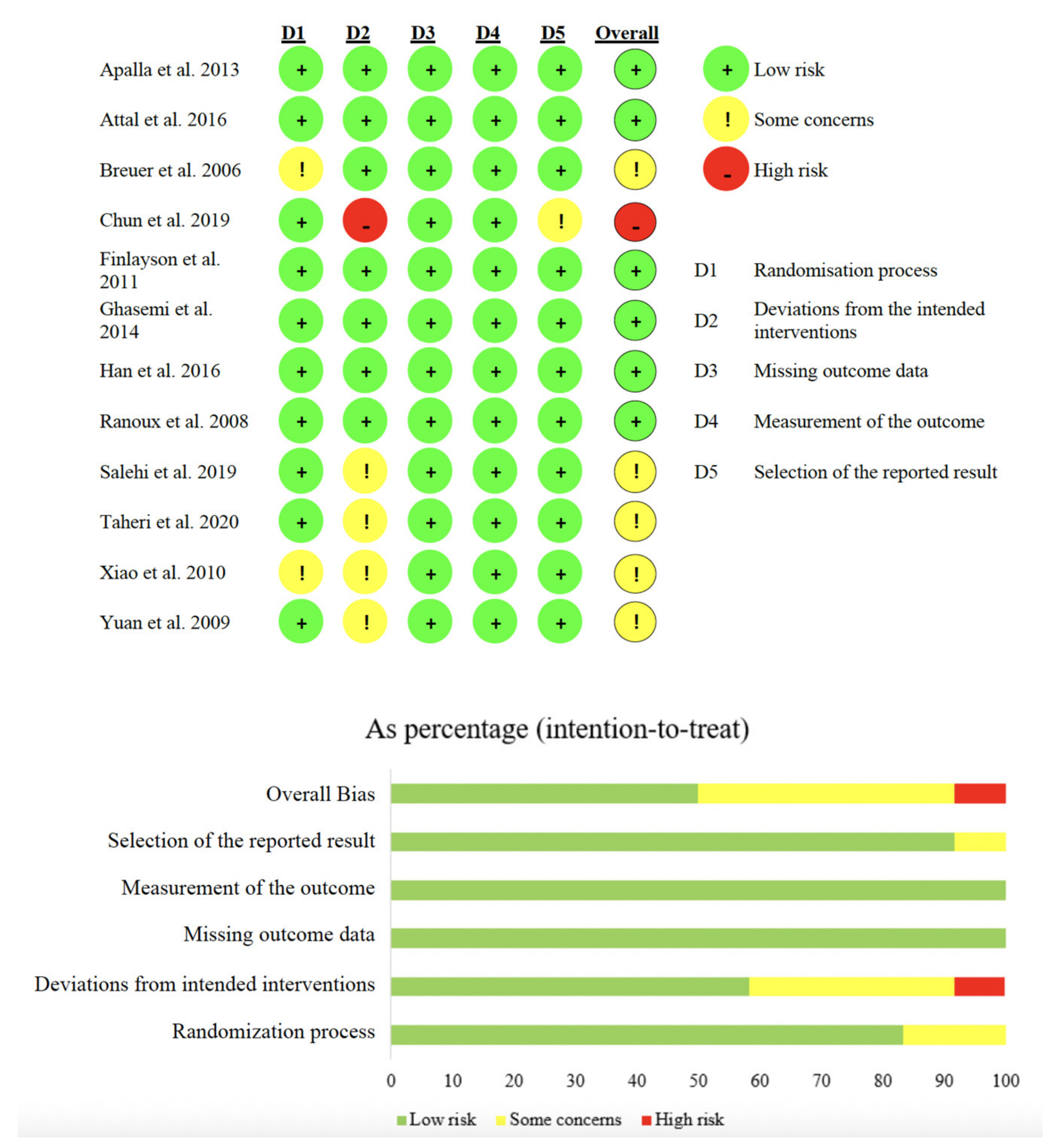
2.3. Study Quality
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Registration
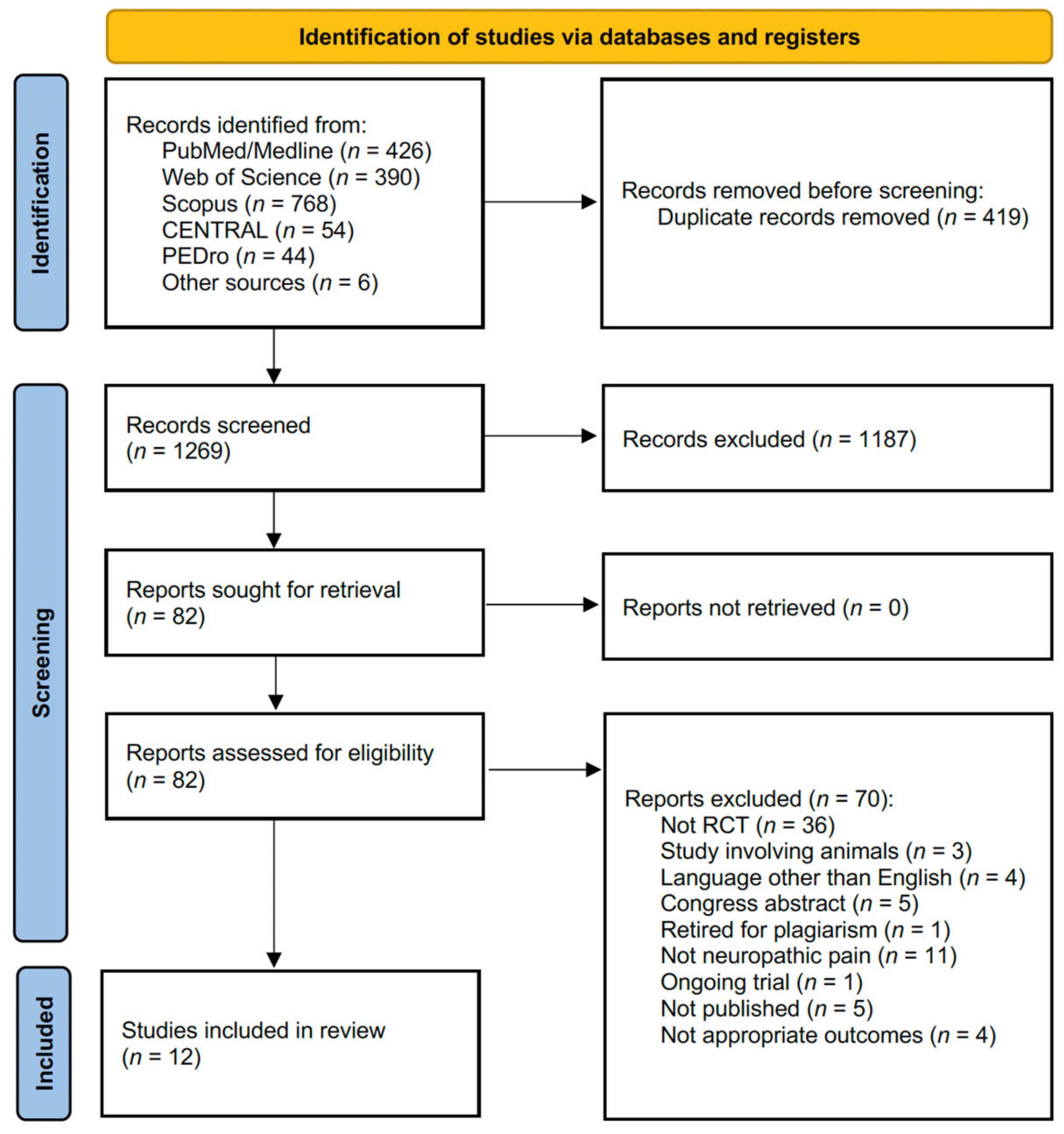
5.2. Search Strategy
5.3. Selection Criteria
- (P) Participants: adults suffering from neuropathic pain.
- (I) Intervention: BoNT type A (BoNT-A) or BoNT type B (BoNT-B) administration.
- (C) Comparator: any comparator, including placebo, other pharmacological treatment, non-pharmacological treatment or no treatment.
- (O) Outcome: the primary outcome was self-reported pain relief in terms of multidimensional pain scales. The secondary outcomes were HR-QoL, physical function, anxiety and depression, and sleep quality.
5.4. Data Extraction and Synthesis
5.5. Quality Assessment and Risk of Bias
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BoNT | botulinum toxin |
| BoNT-A | BoNT type A |
| BoNT-B | BoNT type B |
| CENTRAL | Cochrane Central Register of Controlled Trials |
| HADS | Hospital Anxiety and Depression Scale |
| HR-QoL | health-related quality of life |
| NRS | Numerical Rating Scale |
| NS | non significant |
| PEDro | Physiotherapy Evidence Database |
| RCTs | randomized controlled trials |
| SNRIs | Serotonin and norepinephrine reuptake inhibitors |
| TENS | Transcutaneous Electrical Nerve Stimulator |
| TRPM8 | Transient Receptor Potential Member 8 |
| TRPV1 | Transient Receptor Potential Vanilloid 1 |
| VAS | Visual Analogue Scale |
| WHOQOL-BREF | World Health Organization Quality of Life questionnaire |
References
- Scholz, J.; Finnerup, N.B.; Attal, N.; Aziz, Q.; Baron, R.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Cruccu, G.; Davis, K.D.; et al. The IASP classification of chronic pain for ICD-11: Chronic neuropathic pain. Pain 2019, 160, 53–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doth, A.H.; Hansson, P.T.; Jensen, M.P.; Taylor, R.S. The burden of neuropathic pain: A systematic review and meta-analysis of health utilities. Pain 2010, 149, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Bernetti, A.; Agostini, F.; de Sire, A.; Mangone, M.; Tognolo, L.; Di Cesare, A.; Ruiu, P.; Paolucci, T.; Invernizzi, M.; Paoloni, M. Neuropathic Pain and Rehabilitation: A Systematic Review of International Guidelines. Diagnostics 2021, 11, 74. [Google Scholar] [CrossRef] [PubMed]
- Langley, P.C.; Van Litsenburg, C.; Cappelleri, J.C.; Carroll, D. The burden associated with neuropathic pain in Western Europe. J. Med. Econ. 2013, 16, 85–95. [Google Scholar] [CrossRef]
- Colloca, L.; Ludman, T.; Bouhassira, D.; Baron, R.; Dickenson, A.H.; Yarnitsky, D.; Freeman, R.; Truini, A.; Attal, N.; Finnerup, N.B.; et al. Neuropathic pain. Nat. Rev. Dis. Primers 2017, 3, 17002. [Google Scholar] [CrossRef] [Green Version]
- Van Hecke, O.; Austin, S.K.; Khan, R.A.; Smith, B.H.; Torrance, N. Neuropathic pain in the general population: A systematic review of epidemiological studies. Pain 2014, 155, 654–662. [Google Scholar] [CrossRef]
- Deng, Y.; Luo, L.; Hu, Y.; Fang, K.; Liu, J. Clinical practice guidelines for the management of neuropathic pain: A systematic review. BMC Anesth. 2016, 16, 12. [Google Scholar] [CrossRef] [Green Version]
- Bates, D.; Schultheis, B.C.; Hanes, M.C.; Jolly, S.M.; Chakravarthy, K.V.; Deer, T.R.; Levy, R.M.; Hunter, C.W. A Comprehensive Algorithm for Management of Neuropathic Pain. Pain Med. 2019, 20, S2–S12. [Google Scholar] [CrossRef] [Green Version]
- Baron, R.; Binder, A.; Wasner, G. Neuropathic pain: Diagnosis, pathophysiological mechanisms, and treatment. Lancet Neurol. 2010, 9, 807–819. [Google Scholar] [CrossRef]
- Braz, J.; Solorzano, C.; Wang, X.; Basbaum, A.I. Transmitting pain and itch messages: A contemporary view of the spinal cord circuits that generate gate control. Neuron 2014, 82, 522–536. [Google Scholar] [CrossRef] [Green Version]
- Tsuda, M.; Koga, K.; Chen, T.; Zhuo, M. Neuronal and microglial mechanisms for neuropathic pain in the spinal dorsal horn and anterior cingulate cortex. J. Neurochem. 2017, 141, 486–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, T.S.; Fu, W.; Donahue, R.R.; Corder, G.F.; Hokfelt, T.; Wiley, R.G.; Taylor, B.K. Facilitation of neuropathic pain by the NPY Y1 receptor-expressing subpopulation of excitatory interneurons in the dorsal horn. Sci. Rep. 2019, 9, 7248. [Google Scholar] [CrossRef] [PubMed]
- Papuc, E.; Rejdak, K. The role of neurostimulation in the treatment of neuropathic pain. Ann. Agric. Environ. Med. 2013, 1, 14–17. [Google Scholar]
- Wu, G.; Ringkamp, M.; Hartke, T.V.; Murinson, B.B.; Campbell, J.N.; Griffin, J.W.; Meyer, R.A. Early onset of spontaneous activity in uninjured C-fiber nociceptors after injury to neighboring nerve fibers. J. Neurosci. 2001, 21, RC140. [Google Scholar] [CrossRef]
- Caterina, M.J.; Julius, D. The vanilloid receptor: A molecular gateway to the pain pathway. Ann. Rev. Neurosci. 2001, 24, 487–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serra, J.; Sola, R.; Quiles, C.; Casanova-Molla, J.; Pascual, V.; Bostock, H.; Valls-Sole, J. C-nociceptors sensitized to cold in a patient with small-fiber neuropathy and cold allodynia. Pain 2009, 147, 46–53. [Google Scholar] [CrossRef]
- Wasner, G.; Schattschneider, J.; Binder, A.; Baron, R. Topical menthol—A human model for cold pain by activation and sensitization of C nociceptors. Brain 2004, 127, 1159–1171. [Google Scholar] [CrossRef]
- Chaparro, L.E.; Wiffen, P.J.; Moore, R.A.; Gilron, I. Combination pharmacotherapy for the treatment of neuropathic pain in adults. Cochrane Database Syst. Rev. 2012, 2020, CD008943. [Google Scholar] [CrossRef]
- Smith, E.S.J. Advances in understanding nociception and neuropathic pain. J. Neurol. 2018, 265, 231–238. [Google Scholar] [CrossRef] [Green Version]
- De Sire, A.; Ammendolia, A.; Lippi, L.; Farì, G.; Cisari, C.; Invernizzi, M. Percutaneous Electrical Nerve Stimulation (PENS) as a Rehabilitation Approach for Reducing Mixed Chronic Pain in Patients with Musculoskeletal Disorders. Appl. Sci. 2021, 11, 4257. [Google Scholar] [CrossRef]
- De Sire, A.; Lippi, L.; Curci, C.; Calafiore, D.; Cisari, C.; Ammendolia, A.; Invernizzi, M. Effectiveness of Combined Treatment Using Physical Exercise and Ultrasound-Guided Radiofrequency Ablation of Genicular Nerves in Patients with Knee Osteoarthritis. Appl. Sci. 2021, 11, 4338. [Google Scholar] [CrossRef]
- Harden, N.; Cohen, M. Unmet Needs in the Management of Neuropathic Pain. J. Pain Symptom Manag. 2003, 25, S12–S17. [Google Scholar] [CrossRef]
- Intiso, D.; Basciani, M.; Santamato, A.; Intiso, M.; Di Rienzo, F. Botulinum Toxin Type A for the Treatment of Neuropathic Pain in Neuro-Rehabilitation. Toxins 2015, 7, 2454–2480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fishman, L.M.; Anderson, C.; Rosner, B. BOTOX and physical therapy in the treatment of piriformis syndrome. Am. J. Phys. Med. Rehabil. 2002, 81, 936–942. [Google Scholar] [CrossRef] [PubMed]
- Baricich, A.; Picelli, A.; Carda, S.; Smania, N.; Cisari, C.; Santamato, A.; de Sire, A.; Invernizzi, M. Electrical stimulation of antagonist muscles after botulinum toxin type A for post-stroke spastic equinus foot. A randomized single-blind pilot study. Ann. Phys. Rehabil. Med. 2019, 62, 214–219. [Google Scholar] [CrossRef]
- Attal, N.; de Andrade, D.C.; Adam, F.; Ranoux, D.; Teixeira, M.J.; Galhardoni, R.; Raicher, I.; Uceyler, N.; Sommer, C.; Bouhassira, D. Safety and efficacy of repeated injections of botulinum toxin A in peripheral neuropathic pain (BOTNEP): A randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2016, 15, 555–565. [Google Scholar] [CrossRef]
- Foster, L.; Clapp, L.; Erickson, M.; Jabbari, B. Botulinum toxin A and chronic low back pain: A randomized, double-blind study. Neurology 2001, 56, 1290–1293. [Google Scholar] [CrossRef]
- Park, H.J.; Lee, Y.; Lee, J.; Park, C.; Moon, D.E. The effects of botulinum toxin A on mechanical and cold allodynia in a rat model of neuropathic pain. Can. J. Anaesth. 2006, 53, 470–477. [Google Scholar] [CrossRef] [Green Version]
- Finnerup, N.B.; Attal, N.; Haroutounian, S.; McNicol, E.; Baron, R.; Dworkin, R.H.; Gilron, I.; Haanpaa, M.; Hansson, P.; Jensen, T.S.; et al. Pharmacotherapy for neuropathic pain in adults: A systematic review and meta-analysis. Lancet Neurol. 2015, 14, 162–173. [Google Scholar] [CrossRef] [Green Version]
- Moisset, X.; Bouhassira, D.; Avez Couturier, J.; Alchaar, H.; Conradi, S.; Delmotte, M.H.; Lanteri-Minet, M.; Lefaucheur, J.P.; Mick, G.; Piano, V.; et al. Pharmacological and non-pharmacological treatments for neuropathic pain: Systematic review and French recommendations. Rev. Neurol. 2020, 176, 325–352. [Google Scholar] [CrossRef]
- Morra, M.E.; Elgebaly, A.; Elmaraezy, A.; Khalil, A.M.; Altibi, A.M.; Vu, T.L.; Mostafa, M.R.; Huy, N.T.; Hirayama, K. Therapeutic efficacy and safety of Botulinum Toxin A Therapy in Trigeminal Neuralgia: A systematic review and meta-analysis of randomized controlled trials. J. Headache Pain 2016, 17, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Do, T.M.; Unis, G.D.; Kattar, N.; Ananth, A.; McCoul, E.D. Neuromodulators for Atypical Facial Pain and Neuralgias: A Systematic Review and Meta-Analysis. Laryngoscope 2021, 131, 1235–1253. [Google Scholar] [CrossRef] [PubMed]
- Li, X.L.; Zeng, X.; Zeng, S.; He, H.P.; Zeng, Z.; Peng, L.L.; Chen, L.G. Botulinum toxin A treatment for post-herpetic neuralgia: A systematic review and meta-analysis. Exp. Med. 2020, 19, 1058–1064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Battista, S.; Buzzatti, L.; Gandolfi, M.; Finocchi, C.; Falsiroli Maistrello, L.; Viceconti, A.; Giardulli, B.; Testa, M. The Use of Botulinum Toxin A as an Adjunctive Therapy in the Management of Chronic Musculoskeletal Pain: A Systematic Review with Meta-Analysis. Toxins 2021, 13, 640. [Google Scholar] [CrossRef]
- Dawson, A.; Dawson, J.; Ernberg, M. The effect of botulinum toxin A on patients with persistent idiopathic dentoalveolar pain—A systematic review. J. Oral Rehabil. 2020, 47, 1184–1191. [Google Scholar] [CrossRef]
- Apalla, Z.; Sotiriou, E.; Lallas, A.; Lazaridou, E.; Ioannides, D. Botulinum toxin A in postherpetic neuralgia: A parallel, randomized, double-blind, single-dose, placebo-controlled trial. Clin. J. Pain 2013, 29, 857–864. [Google Scholar] [CrossRef]
- Chun, A.; Levy, I.; Yang, A.; Delgado, A.; Tsai, C.Y.; Leung, E.; Taylor, K.; Kolakowsky-Hayner, S.; Huang, V.; Escalon, M.; et al. Treatment of at-level spinal cord injury pain with botulinum toxin A. Spinal Cord Ser. Cases 2019, 5, 77. [Google Scholar] [CrossRef]
- Finlayson, H.C.; O’Connor, R.J.; Brasher, P.M.A.; Travlos, A. Botulinum toxin injection for management of thoracic outlet syndrome: A double-blind, randomized, controlled trial. Pain 2011, 152, 2023–2028. [Google Scholar] [CrossRef]
- Ghasemi, M.; Ansari, M.; Basiri, K.; Shaigannejad, V. The effects of intradermal botulinum toxin type a injections on pain symptoms of patients with diabetic neuropathy. J. Res. Med. Sci. 2014, 19, 106–111. [Google Scholar]
- Han, Z.A.; Song, D.H.; Oh, H.M.; Chung, M.E. Botulinum toxin type A for neuropathic pain in patients with spinal cord injury. Ann. Neurol. 2016, 79, 569–578. [Google Scholar] [CrossRef]
- Ranoux, D.; Attal, N.; Morain, F.; Bouhassira, D. Botulinum toxin type A induces direct analgesic effects in chronic neuropathic pain. Ann. Neurol. 2008, 64, 274–283. [Google Scholar] [CrossRef] [PubMed]
- Salehi, H.; Moussaei, M.; Kamiab, Z.; Vakilian, A. The effects of botulinum toxin type A injection on pain symptoms, quality of life, and sleep quality of patients with diabetic neuropathy: A randomized double-blind clinical trial. Iran. J. Neurol. 2019, 18, 99–107. [Google Scholar] [CrossRef]
- Taheri, M.; Sedaghat, M.; Solhpour, A.; Rostami, P.; Lima, B.S. The Effect of Intradermal Botulinum Toxin a injections on painful diabetic polyneuropathy. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 1823–1828. [Google Scholar] [CrossRef] [PubMed]
- Xiao, L.; Mackey, S.; Hui, H.; Xong, D.; Zhang, Q.; Zhang, D. Subcutaneous injection of botulinum toxin a is beneficial in postherpetic neuralgia. Pain Med. 2010, 11, 1827–1833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, R.Y.; Sheu, J.J.; Yu, J.M.; Chen, W.T.; Tseng, I.J.; Chang, H.H.; Hu, C.J. Botulinum toxin for diabetic neuropathic pain: A randomized double-blind crossover trial. Neurology 2009, 72, 1473–1478. [Google Scholar] [CrossRef] [PubMed]
- Breuer, B.; Sperber, K.; Wallenstein, S.; Kiprovski, K.; Calapa, A.; Snow, B.; Pappagallo, M. Clinically significant placebo analgesic response in a pilot trial of botulinum B in patients with hand pain and carpal tunnel syndrome. Pain Med. 2006, 7, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Egeo, G.; Fofi, L.; Barbanti, P. Botulinum Neurotoxin for the Treatment of Neuropathic Pain. Front. Neurol. 2020, 11, 716. [Google Scholar] [CrossRef]
- Oh, H.M.; Chung, M.E. Botulinum Toxin for Neuropathic Pain: A Review of the Literature. Toxins 2015, 7, 3127–3154. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Chung, M.E. Botulinum Toxin for Central Neuropathic Pain. Toxins 2018, 10, 224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.; Park, H.J. Botulinum Toxin for the Treatment of Neuropathic Pain. Toxins 2017, 9, 260. [Google Scholar] [CrossRef] [Green Version]
- Wei, J.; Zhu, X.; Yang, G.; Shen, J.; Xie, P.; Zuo, X.; Xia, L.; Han, Q.; Zhao, Y. The efficacy and safety of botulinum toxin type A in treatment of trigeminal neuralgia and peripheral neuropathic pain: A meta-analysis of randomized controlled trials. Brain Behav. 2019, 9, e01409. [Google Scholar] [CrossRef] [PubMed]
- Lakra, C.; Cohen, H. A clinical review of the use of Botulinum Toxin type A in managing central neuropathic pain in patients with spinal cord injury. J. Spinal Cord Med. 2020, 2, 1–5. [Google Scholar] [CrossRef]
- Ahmed, S.; Subramaniam, S.; Sidhu, K.; Khattab, S.; Singh, D.; Babineau, J.; Kumbhare, D.A. Effect of Local Anesthetic Versus Botulinum Toxin-A Injections for Myofascial Pain Disorders: A Systematic Review and Meta-Analysis. Clin. J. Pain 2019, 35, 353–367. [Google Scholar] [CrossRef] [PubMed]
- Forstenpointner, J.; Rice, A.S.C.; Finnerup, N.B.; Baron, R. Up-date on Clinical Management of Postherpetic Neuralgia and Mechanism-Based Treatment: New Options in Therapy. J. Infect. Dis. 2018, 218, S120–S126. [Google Scholar] [CrossRef] [PubMed]
- Hary, V.; Schitter, S.; Martinez, V. Efficacy and safety of botulinum A toxin for the treatment of chronic peripheral neuropathic pain: A systematic review of randomized controlled trials and meta-analysis. Eur. J. Pain 2022, 26, 980–990. [Google Scholar] [CrossRef] [PubMed]
- Van Boekel, R.L.M.; Vissers, K.C.P.; van der Sande, R.; Bronkhorst, E.; Lerou, J.G.C.; Steegers, M.A.H. Moving beyond pain scores: Multidimensional pain assessment is essential for adequate pain management after surgery. PLoS ONE 2017, 12, e0177345. [Google Scholar] [CrossRef]
- Teasell, R.; Foley, N.; Pereira, S.; Sequeira, K.; Miller, T. Evidence to practice: Botulinum toxin in the treatment of spasticity post stroke. Top. Stroke Rehabil. 2012, 19, 115–121. [Google Scholar] [CrossRef]
- Baricich, A.; Picelli, A.; Santamato, A.; Carda, S.; de Sire, A.; Smania, N.; Cisari, C.; Invernizzi, M. Safety Profile of High-Dose Botulinum Toxin Type A in Post-Stroke Spasticity Treatment. Clin. Drug Investig. 2018, 38, 991–1000. [Google Scholar] [CrossRef]
- Hernandez Herrero, D.; Miangolarra Page, J.C. Descriptive analysis of the annual cost of treating spasticity with different types of botulinum toxin A. Neurologia, 2019; in press. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.H.; Hebert, H.L.; Veluchamy, A. Neuropathic pain in the community: Prevalence, impact, and risk factors. Pain 2020, 161 (Suppl. 1), S127–S137. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Zhang, Q.; Wang, R.; Xu, L. Botulinum Toxin Type A for Diabetic Peripheral Neuropathy Pain: A Systematic Review and Meta-Analysis. J. Pain Res. 2021, 14, 3855–3863. [Google Scholar] [CrossRef] [PubMed]
- Fitzmaurice, B.C.; Rayen, A.T.A. Treatments for neuropathic pain: Up-to-date evidence and recommendations. BJA Educ. 2018, 18, 277–283. [Google Scholar] [CrossRef] [Green Version]
- Rhon, D.I.; Fritz, J.M.; Greenlee, T.A.; Dry, K.E.; Mayhew, R.J.; Laugesen, M.C.; Dragusin, E.; Teyhen, D.S. Move to health-a holistic approach to the management of chronic low back pain: An intervention and implementation protocol developed for a pragmatic clinical trial. J. Transl. Med. 2021, 19, 357. [Google Scholar] [CrossRef] [PubMed]
- Sdrulla, A.; Chen, G. Minimally invasive procedures for neuropathic pain. Pain Manag. 2016, 2, 6:103-9. [Google Scholar] [CrossRef]
- Szok, D.; Tajti, J.; Nyari, A.; Vecsei, L. Therapeutic Approaches for Peripheral and Central Neuropathic Pain. Behav. Neurol. 2019, 2019, 8685954. [Google Scholar] [CrossRef]
- Varshney, V.; Osborn, J.; Chaturvedi, R.; Shah, V.; Chakravarthy, K. Advances in the interventional management of neuropathic pain. Ann. Transl. Med. 2021, 9, 187. [Google Scholar] [CrossRef]
- De Sire, A.; Moggio, L.; Demeco, A.; Fortunato, F.; Spano, R.; Aiello, V.; Marotta, N.; Ammendolia, A. Efficacy of rehabilitative techniques in reducing hemiplegic shoulder pain in stroke: Systematic review and meta-analysis. Ann. Phys. Rehabil. Med. 2021, 65, 101602. [Google Scholar] [CrossRef]
- Cavalli, E.; Mammana, S.; Nicoletti, F.; Bramanti, P.; Mazzon, E. The neuropathic pain: An overview of the current treatment and future therapeutic approaches. Int. J. Immunopathol. Pharm. 2019, 33, 2058738419838383. [Google Scholar] [CrossRef] [Green Version]
- Petrosino, S.; Schiano Moriello, A. Palmitoylethanolamide: A Nutritional Approach to Keep Neuroinflammation within Physiological Boundaries-A Systematic Review. Int. J. Mol. Sci. 2020, 21, 9526. [Google Scholar] [CrossRef] [PubMed]
- Rowin, J. Integrative neuromuscular medicine: Neuropathy and neuropathic pain: Consider the alternatives. Muscle Nerve 2019, 60, 124–136. [Google Scholar] [CrossRef] [PubMed]
- Leitzelar, B.N.; Koltyn, K.F. Exercise and Neuropathic Pain: A General Overview of Preclinical and Clinical Research. Sports Med. Open 2021, 7, 21. [Google Scholar] [CrossRef] [PubMed]
- Andersen Hammond, E.; Pitz, M.; Shay, B. Neuropathic Pain in Taxane-Induced Peripheral Neuropathy: Evidence for Exercise in Treatment. Neurorehabil. Neural. Repair. 2019, 33, 792–799. [Google Scholar] [CrossRef] [PubMed]
- Mokhtari, T.; Ren, Q.; Li, N.; Wang, F.; Bi, Y.; Hu, L. Transcutaneous Electrical Nerve Stimulation in Relieving Neuropathic Pain: Basic Mechanisms and Clinical Applications. Curr. Pain Headache Rep. 2020, 24, 14. [Google Scholar] [CrossRef]
- Domoto, R.; Sekiguchi, F.; Tsubota, M.; Kawabata, A. Macrophage as a Peripheral Pain Regulator. Cells 2021, 10, 1881. [Google Scholar] [CrossRef]
- Matak, I.; Bolcskei, K.; Bach-Rojecky, L.; Helyes, Z. Mechanisms of Botulinum Toxin Type A Action on Pain. Toxins 2019, 11, 459. [Google Scholar] [CrossRef] [Green Version]
- Lai, J.; Hunter, J.C.; Porreca, F. The role of voltage-gated sodium channels in neuropathic pain. Curr. Opin. Neurobiol. 2003, 13, 291–297. [Google Scholar] [CrossRef]
- Black, J.A.; Nikolajsen, L.; Kroner, K.; Jensen, T.S.; Waxman, S.G. Multiple sodium channel isoforms and mitogen-activated protein kinases are present in painful human neuromas. Ann. Neurol. 2008, 64, 644–653. [Google Scholar] [CrossRef]
- Siqueira, S.R.; Alves, B.; Malpartida, H.M.; Teixeira, M.J.; Siqueira, J.T. Abnormal expression of voltage-gated sodium channels Nav1.7, Nav1.3 and Nav1.8 in trigeminal neuralgia. Neuroscience 2009, 164, 573–577. [Google Scholar] [CrossRef]
- Kim, D.W.; Lee, S.K.; Ahnn, J. Botulinum Toxin as a Pain Killer: Players and Actions in Antinociception. Toxins 2015, 7, 2435–2453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liampas, A.; Rekatsina, M.; Vadalouca, A.; Paladini, A.; Varrassi, G.; Zis, P. Non-Pharmacological Management of Painful Peripheral Neuropathies: A Systematic Review. Adv. Ther. 2020, 37, 4096–4106. [Google Scholar] [CrossRef] [PubMed]
- Couto, D.S.; Goulart, G.; Luciano, L.L.; Cardoso, E.J.R. Quality of life in neuropathic pain: A literature review. Res. Soc. Dev. 2021, 10, e416101422250. [Google Scholar] [CrossRef]
- Binder, A.; Baron, R. The Pharmacological Therapy of Chronic Neuropathic Pain. Dtsch. Arztebl. Int. 2016, 113, 616–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.2; John Wiley & Sons: Hoboken, NJ, USA, 2021. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Lin, J.; Demner-Fushman, D. Evaluation of PICO as a knowledge representation for clinical questions. AMIA Annu. Symp. Proc. 2006, 2006, 359–363. [Google Scholar]



{kind=link}
{kind=link}
| Article | Design | Intervention Characteristics | Comparison | Sample Size | Outcomes Measures | Follow-Up | Main Findings | Indications | |
|---|---|---|---|---|---|---|---|---|---|
| Intervention | Comparator | ||||||||
| Apalla et al. [36] | Randomized, double-blind, placebo-controlled clinical trial | Forty injections of Onabotulinumtoxin-A (100 units) in the painful area | Placebo (normal saline) injections | Patients with post-herpetic neuropathy n: 15 male/female: 8/7 Mean age: 73.2 ± 10.5 | Patients with post-herpetic neuropathy n: 15 male/female: 10/5 Mean age: 77.5 ± 8.2 | Quality of sleep, assessed by five-item questionnaire with a score ranging from 0 to 3 | 24 weeks | Intervention Group Sleep scores: significant improvements at week 2, which remained stable between weeks 2 and 4; after the initial decline, sleep scores remain unchanged until week 12 Comparator Group Sleep scores: no significant improvement at week 2, which remained unchanged between weeks 2 and 4 Between groups Sleep scores: significant differences at week 2 | BoNT-A administration significantly improves quality of sleep at 2 weeks. |
| Xiao et al. [44] | Randomized, double-blind, placebo-controlled clinical trial | BoNT-A group: administrations (comprising several injections) of LanbotulinumtoxinA (up to 200 units). | Lidocaine (active control) group: administrations (comprising several injections) of 0.5% lidocaine. Placebo group: placebo (normal saline) injections. | BoNT-A group: patients with postherpetic neuropathy n: 20 male/female: 11/9 Mean age: 70 ± 15.4 | Lidocaine group: patients with postherpetic neuropathy n: 20 male/female: 8/12 Mean age: 65 ± 14.2 Placebo group: patients with postherpetic neuropathy n:20 male/female: 9/11 Mean age: 67 ± 12.1 | Sleep time (hours) | 3 months | Intervention Group Sleep time: significant improvement on day 7 and after 3 months Comparator Group Sleep time: significant improvement on day 7 and after 3 months in both lidocaine group and placebo group Between groups Sleep time: improvement of IG was significantly greater compared with lidocaine and placebo groups | BoNT-A administration significantly improves sleep time. |
| Attal et al. [26] | Randomized, double-blind, placebo-controlled, parallel-group clinical trial | Two administrations of Onabotulinumtoxin A (up to 300 units), 12 weeks apart. | Two administrations of saline, 12 weeks apart. | Patients with peripheral nerve lesion n: 34 male/female: 17/17 Mean age: 51.6 ± 16.7 | Patients with peripheral nerve lesion n: 32 male/female: 20/12 Mean age: 52.3 ± 15.8 | BPI, NPSI, EQ5D VAS, HADS, Sleep Problem Index | 24 weeks | Intervention Group BPI VAS: significant reduction NPSI burning pain and paroxysmal pain subitem: significant improvement HADS, EQ5D VAS, Sleep Problem Index: p = NS Comparator Group BPI, NPSI, HADS, EQ5D VAS, Sleep Problem Index: p = NS Between groups BPI VAS: significant differences NPSI subscales: significant differences in paroxysmal pain and allodynia HADS: significant differences in anxiety Sleep Problem Index—6 items: significant differences Sleep Problem Index—9 items: significant differences | BoNT-A administration significantly improves of BPI VAS, NPSI burning pain and paroxysmal pain subitem, HADS, and Sleep Problem Index |
| Ranoux et al. [41] | Randomized, double-blind, placebo-controlled, parallel-group clinical trial | Administrations of Onabotulinumtoxin A (up to 200 units). | Administrations of saline. | Patients with posttraumatic/ postoperative or postherpetic neuropathy n: 15 male/female: 6/9 Mean age: 53.8 ± 13.9 | Patients with posttraumatic/ postoperative or postherpetic neuropathy n: 14 male/female: 4/10 mean age: 49.7 ± 15.9 | NPSI, BPI, HADS | 24 weeks | Intervention Group NPSI subitems (burning, paroxysmal pain, allodynia): significant improvement at 12 weeks General activity and mood: improvement without significance HADS anxiety: slight improvement without significance Comparator Group NPSI, BPI, HADS: p = NS Between groups NPSI subscales (burning, electric shock and evoked pain to cold): significant differences at 12 weeks, without significant differences at week 24 BPI pain intensity: significant differences HADS: NS at 24 weeks | BoNT-A administration significantly improves NPSI subscales (burning, electric shock, and evoked pain to cold), and BPI pain intensity |
| Finlayson et al. [38] | Randomized, double-blind, placebo-controlled clinical trial | Seventy-five units of OnabotulinumtoxinA injected in the anterior and middle scalene muscles under EMG guidance. | Saline injected in the anterior and middle scalene muscles under EMG guidance. | Patients with thoracic outlet syndrome n: 20 male/female: 3/17 Mean age: 36.8 ± 8.9 | Patients with thoracic outlet syndrome n: 18 male/female: 4/14 Mean age: 38.7 ± 7.0 | DASH, SF-36 | 6 months | Intervention Group DASH, SF-36: not significant Comparator Group DASH, SF-36: not significant Between groups DASH, SF-36: not significant differences | BoNT-A administration did not improve DASH and SF-36 |
| Ghasemi et al. [39] | Randomized, double-blind, placebo-controlled clinical trial | 100 units of AbobotulinumtoxinA in 0.9% saline were injected, each injection approximately 8–10 units | Placebo (normal saline) injections | Patients with diabetic neuropathy n: 20 male/female: 9/11 Mean age: 62.7 ± 9.9 | Patients with diabetic neuropathy n: 20 male/female: 13/7 Mean age: 59.3 ± 9.6 | NPS and DN4 questionnaire. | 3 weeks | Intervention Group NPS subitems: significant differences, except for cold sensation DN4 questionnaire subitems: significant improvement (electric shocks, burning, pins and needle, and brushing) Comparator Group NPS subitems: NS DN4 questionnaire subitems: NS Between groups NR | BoNT-A administration significantly improves NPS (except for cold sensation) and DN4 questionnaire subitems (electric shocks, burning, pins and needles, and brushing subitems) |
| Salehi et al. [42] | Randomized double-blind, placebo-controlled clinical trial | Twelve injections of AbobotulinumtoxinA (8.33 units each point) in the dorsal foot surface | Placebo (normal saline) injections | Patients with diabetic neuropathy n:16 male/female: 6/10 Mean age: 58.3 ± 5.3 | Patients with diabetic neuropathy n:16 male/female: 6/10 Mean age: 56.7 ± 7.5 | NPS, SF-36, and PSQI questionnaires. | 12 weeks | Intervention Group NPS, SF-36 subitems: significant improvement PSQI: significant decrease Comparator Group NR Between groups SF-36: significant differences PSQI: significant differences NPS subitems: significant differences, except for sharp sensation, sensory sensation, and deep sensation | BoNT-A administration significantly improve SF-36, PSQI and NPS subitems (except for sharp sensation, sensory sensation, and deep sensation) |
| Taheri et al. [43] | Randomized, double-blind, placebo-controlled clinical trial | Group 1: twenty injections of BoNT-A (for a total of 150 units) in the sole of the right foot (7.5 units each injection); in the other feet, same procedure with saline placebo. Group 2: twenty injections of BoNT-A (for a total of 75 units) in the sole of both feet (3.75 units each injection, for a total of 150 units). | Placebo group: both feet with placebo (normal saline) injections. | Group 1: Patients with diabetic neuropathic pain n: 47 male/female: 16/31 Mean age: 54.5 ± 7.6 Group 2: Patients with diabetic neuropathic pain n: 47 male/female: 20/27 Mean age: 56.9 ± 6.2 | Group N: Patients with diabetic neuropathic pain n: 47 male/female: 19/28 Mean age: 54.3 ± 8.2 | NPS | 4 weeks | Intervention Group Group 1: NPS subitems: significant improvements, except for dull sensation and cold sensation Group 2: NPS subitems: significant improvements, except for dull sensation (p = 0.622) and cold sensation Comparator Group NPS subitems: significant improvements, except for dull sensation, cold sensation (p = 0.067), unpleasant sensation and surface pain. Between groups NPS subitems: pain intensity, sharp sensation, hot sensation, sensitive sensation, unpleasant sensation, deep pain, and surface pain improved significantly after IGs vs. CG. Hot sensation subitem showed a significant difference between Group 1 vs. Group 2. Dull and cold sensations improvement did not show a significant difference between Group 2 and N. | BoNT-A administration significantly improve NPS (pain intensity, sharp sensation, hot sensation, sensitive sensation, unpleasant sensation, deep pain, and surface pain subitems) |
| Yuan et al. [45] | Randomized, double-blind, placebo-controlled, crossover clinical trial | OnabotulinumtoxinA injection of 50 units into each foot (4 units per injection); then crossover after 12 weeks. | Saline injection into each foot; then crossover after 12 weeks. | Patients with diabetic neuropathy n: 9 male/female: 6/12 Mean age: 65.6 ± 9.2 | Patients with diabetic neuropathy n: 9 male/female: 6/12 Mean age: 65.6 ± 9.2 | CPSQI, and SF-36 | 24 weeks | Intervention Group CPSQI: NS at week 12 Comparator Group NR Between groups CPSQI: significant improvements at 4 weeks SF-36: NS | BoNT-A administration significantly improve CPSQI |
| Chun et al. [37] | Randomized, double-blind, placebo-controlled, crossover clinical trial | Injection of up to 400 units OnabotulinumtoxinA (phase 1). After 12 weeks of follow up, cross-over of participants was performed and subcutaneous injection of normal saline was administered (phase 2, P2) | Injection of normal saline (placebo) (phase 1). After 12 weeks of follow up, crossover of participants was performed and subcutaneous injection of up to 400 units Onabotulinumtoxin A were administered (phase 2, P2) | Patients with SCI n: 8 male/female: 6/2 Mean age: 45 (32–61) | Patients with SCI n: 8 male/female: 6/2 Mean age: 45 (32–61) | ISCIPBDS and QOL | 20 weeks | Intervention Group ISCIPBDS subitems: change in pain intensity at 8 and 12 weeks in 33% of patients. QOL: 33% of patients reported at least moderate improvements at 2, 4, and 12 weeks, 17% at 8 weeks Comparator Group ISCIPBDS subitems: no patient reported a change in pain intensity at 8 and 12 weeks. 17% reported decreased pain interference with daily activities at 2 and 4 weeks QOL: no changes at 2, 4, 8 and 12 weeks Between groups NR | BoNT-A administration improve ISCIPBDS subitems |
| Han et al. [40] | Randomized, double-blind, placebo-controlled clinical trial | 200 units Letibotulinumtoxin A in 4 mL saline solution 1-time injection in painful area | Placebo (normal saline) injections | Patients with SCI n: 20 male/female: 15/5 Mean age: 53.1 ± 9.1 | Patients with SCI n: 20 male/female: 14/6 Mean age: 48.9 ± 14.2 | SF-MPQ and WHOQOL-BREF. | 8 weeks | Intervention Group NR Comparator Group NR Between groups SF-MPQ: significant differences at 4 weeks and 8 weeks WHOQOL-BREF: NS | BoNT-A administration significantly improves SF-MPQ |
| Breuer et al. [46] | Randomized, double-blind, placebo-controlled clinical pilot trial | 2500 units of rimabotulinumtoxin B in 0.5 mL of normal saline divided in 3 intramuscular under EMG guidance for opponens digiti minimi and flexor digiti minimi, and anatomically located for palmaris brevis muscle | Placebo (normal saline) intramuscular under EMG guidance for opponens digiti minimi and flexor digiti minimi, and anatomically located for palmaris brevis muscle | Patients with carpal tunnel syndrome n: 11 male/female: NR Mean age: NR | Patients with carpal tunnel syndrome n: 9 male/female: NR Mean age: NR | WHYMPI, Quality of sleep | 13 weeks | Intervention Group WHYMPI quality of life indicators: improvements with statistical or borderline significance at different time points Pain interference with sleep (assessed with diary report): improved for weeks 2 through 8 Comparator Group Pain interference with sleep (assessed with phone report): improved for weeks 2 through 8 Between groups WHYMPI, Quality of sleep: no significant differences | BoNT-B administration did not show differences between groups in WHYMPI, and Quality of sleep |
| Study | Type of BoNT | Source of BoNT | Amount of BoNT | Injection Sites | Number of Injections | Rout of Injection |
|---|---|---|---|---|---|---|
| Post Herpetic Neuropathy | ||||||
| Apalla et al. [36] | Onabotulinumtoxin A | Botox, Allergan | 100 units | Painful area | Chessboard distribution, with a minimum distance of 1 cm between injections’ sites, 40 injections in total. | Subcutaneous |
| Xiao et al. [44] | NA | BoNT-A (Lanzhou Institute of Biological Products, Lanzhou, China) | Total maximum administration of 200 units | Painful area | Over the affected area, injections every 1.0–2.0 cm radius of skin. | Subcutaneous |
| Peripheral nerve lesion | ||||||
| Attal et al. [26] | Onabotulinumtoxin A | Botox; Allergan | Total maximum administration of 300 units, 5 units per injection | Painful area | Up to 60 injections, at sites 1.5–2 cm apart. | Subcutaneous |
| Posttraumatic/Postoperative Nerve Lesion or Post Herpetic Neuropathy | ||||||
| Ranoux et al. [41] | Onabotulinumtoxin A | Botox, Allergan | Total maximum administration of 200 units, 5 units per injection | Painful area | Up to 40 injections, at sites 1.5 cm apart in the area mapped with a pen. | Subcutaneous |
| Thoracic Outlet Syndrome | ||||||
| Finlayson et al. [38] | Onabotulinumtoxin A | Botox, Allergan | 75 units | Anterior and middle scalene muscles | 1 injection | Intramuscular under EMG guidance |
| Diabetic neuropathy | ||||||
| Ghasemi et al. [39] | Abobotulinumtoxin A | Dysport, Ipsen | 100 units; each injection approximately 8–10 units | Dorsum of the foot | Grid distribution pattern covering a total of 12 (3 × 4) sites. | Subcutaneous |
| Salehi et al. [42] | Abobotulinumtoxin A | Dysport, Ipsen | 100 units; 0.1 mL (8.33 units) injection per site | Foot surface | Grid pattern of 12 points (3 × 4). | Subcutaneous |
| Taheri et al. [43] | NA | NA | 150 units total; Group D1 each injection 7.5 U, Group D2 each injection 3.75 units. | Sole of the foot | Twenty points at distance of 1 cm from each other (a 5 × 4 grid). | Subcutaneous |
| Yuan et al. [45] | Onabotulinumtoxin A | Botox, Allergan | 50 units per foot; each injection 4 units | Dorsum of the foot | Grid distribution pattern covering a total of 12 (3 × 4) sites. | Subcutaneous |
| Spinal Cord Injury | ||||||
| Chun et al. [37] | Onabotulinumtoxin A | Botox, Allergan | Total maximum administration of 400 units, 5 units per injection | Painful area | Up to 80 injections; the area of pain was marked using a skin marker and a plastic cut-out template for injection sites separated from each other by a 1 cm radius. | Subcutaneous |
| Han et al. [40] | Letibotulinumtoxin A | Meditoxin (Medytox, Seoul, Korea) | 200 units | Painful area | Checkerboard pattern over the maximally affected area. | Subcutaneous |
| Carpal Tunnel Syndrome | ||||||
| Breuer et al. [46] | Rimabotulinumtoxin B | Myobloc, Supernus Pharmaceuticals | 2500 units divided in 3 injections | Opponens digiti minimi, flexor digiti minimi, palmaris brevis muscle | 3 injections (one for each muscle) | Intramuscular under EMG guidance for opponens digiti minimi and flexor digiti minimi, and anatomically located for palmaris brevis muscle |
| Articles | Domain | Score | ||||
|---|---|---|---|---|---|---|
| Random Sequence Generation | Appropriate Randomization | Blinding of Participants or Personnel | Blinding of Outcome Assessors | Withdrawals and Dropouts | ||
| Apalla et al. [36] | 1 | 1 | 1 | 1 | 1 | 5 |
| Attal et al. [26] | 1 | 1 | 1 | 1 | 1 | 5 |
| Breuer et al. [46] | 1 | 0 | 1 | 1 | 0 | 3 |
| Chun et al. [37] | 1 | 1 | 1 | 1 | 1 | 5 |
| Finlayson et al. [38] | 1 | 1 | 1 | 1 | 1 | 5 |
| Ghasemi et al. [39] | 1 | 1 | 1 | 1 | 1 | 5 |
| Han et al. 2016 [40] | 1 | 1 | 1 | 1 | 1 | 5 |
| Ranoux et al. [41] | 1 | 1 | 1 | 1 | 1 | 5 |
| Salehi et al. [42] | 1 | 1 | 1 | 0 | 1 | 4 |
| Taheri et al. [43] | 1 | 1 | 1 | 1 | 0 | 4 |
| Xiao et al. [44] | 1 | 0 | 1 | 1 | 1 | 4 |
| Yuan et al. [45] | 1 | 0 | 1 | 1 | 1 | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lippi, L.; de Sire, A.; Folli, A.; D’Abrosca, F.; Grana, E.; Baricich, A.; Carda, S.; Invernizzi, M. Multidimensional Effectiveness of Botulinum Toxin in Neuropathic Pain: A Systematic Review of Randomized Clinical Trials. Toxins 2022, 14, 308. https://doi.org/10.3390/toxins14050308
Lippi L, de Sire A, Folli A, D’Abrosca F, Grana E, Baricich A, Carda S, Invernizzi M. Multidimensional Effectiveness of Botulinum Toxin in Neuropathic Pain: A Systematic Review of Randomized Clinical Trials. Toxins. 2022; 14(5):308. https://doi.org/10.3390/toxins14050308
Chicago/Turabian StyleLippi, Lorenzo, Alessandro de Sire, Arianna Folli, Francesco D’Abrosca, Elisa Grana, Alessio Baricich, Stefano Carda, and Marco Invernizzi. 2022. "Multidimensional Effectiveness of Botulinum Toxin in Neuropathic Pain: A Systematic Review of Randomized Clinical Trials" Toxins 14, no. 5: 308. https://doi.org/10.3390/toxins14050308