
Characteristics of COVID-19 Breakthrough Infections among Vaccinated Individuals and Associated Risk Factors: A Systematic Review

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
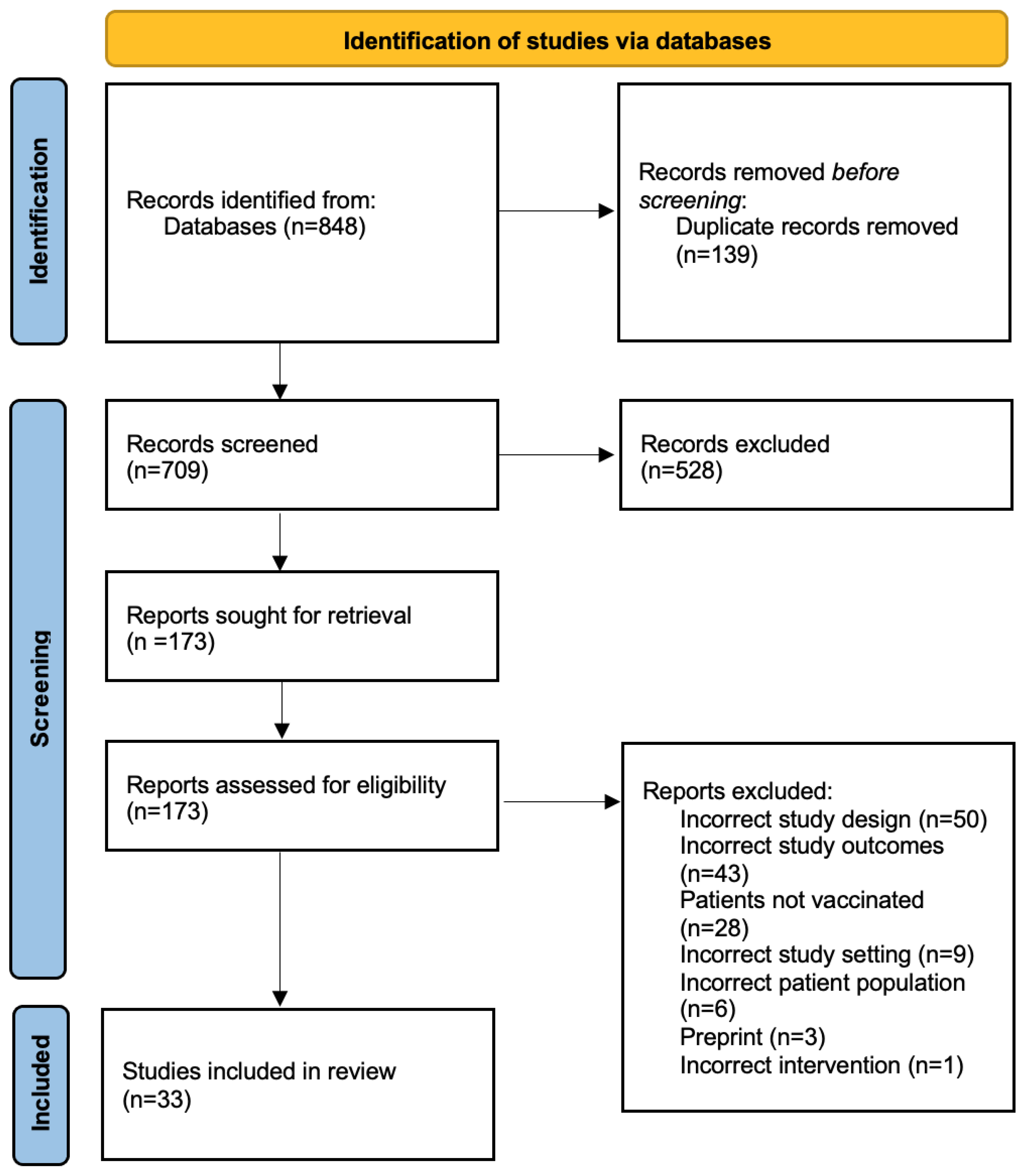
2.1. Search Strategy and Selection Criteria
- Were conducted on adult patients with confirmed COVID-19 diagnosis.
- Reported COVID-19 breakthrough infections.
- Were written in the English language.
- Were peer-reviewed.
- Were either clinical trials, observational studies consisting of prospective cohort, retrospective cohort, case-control studies, case reports, or case series.
- Studies were excluded if they:
- Contained incomplete data.
- Were animal studies.
- Presented outcomes of no interest.
2.2. Data Extraction and Analysis
3. Results
Study Type and Geographical Distribution
4. Discussion
4.1. COVID-19 Vaccines and Efficacy
4.2. SARS-CoV-2 Variants and Breakthrough Infections
4.3. Breakthrough Infections in at-Risk Populations
4.3.1. Immunosuppression
4.3.2. Aging
4.3.3. Occupational Risk
4.3.4. Ct (Cycle Threshold) Values & Viral Loads
4.3.5. Heterogenous Vaccination Regimens
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. 2022. Available online: https://covid19.who.int/ (accessed on 4 February 2022).
- CDC COVID-19 Vaccine Breakthrough Case Investigations Team. COVID-19 Vaccine Breakthrough Infections Reported to CDC—United States, 1 January—30 April 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 792–793. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Rates of COVID-19 Cases and Deaths by Vaccination Status. 2022. Available online: https://covid.cdc.gov/covid-data-tracker/#rates-by-vaccine-status (accessed on 4 March 2022).
- Centers for Disease Control and Prevention. Investigative Criteria for Suspected Cases of SARS-CoV-2 Reinfection (ICR). 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/php/invest-criteria.html (accessed on 9 January 2022).
- Krause, P.R.; Fleming, T.R.; Longini, I.M.; Peto, R.; Briand, S.; Heymann, D.L.; Beral, V.; Snape, M.D.; Rees, H.; Ropero, A.M.; et al. SARS-CoV-2 Variants and Vaccines. N. Engl. J. Med. 2021, 385, 179–186. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Classification of Omicron (B.1.1.529): SARS-CoV-2 Variant of Concern. 2021. Available online: https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-SARS-CoV-2-variant-of-concern (accessed on 27 November 2021).
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of COVID-19 Vaccines against the B.1.617.2 (Delta) Variant. N. Engl. J. Med. 2021, 385, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Fendler, A.; Shepherd, S.; Au, L.; Wilkinson, K.; Wu, M.; Byrne, F.; Cerrone, M.; Schmitt, A.M.; Joharatnam-Hogan, N.; Shum, B.; et al. Adaptive immunity and neutralizing antibodies against SARS-CoV-2 variants of concern following vaccination in patients with cancer: The Capture study. Nat. Cancer 2021, 2, 1321–1337. [Google Scholar] [CrossRef] [PubMed]
- Seyed Alinaghi, S.; Oliaei, S.; Kianzad, S.; Afsahi, A.M.; MohsseniPour, M.; Barzegary, A.; Barzegary, A.; Mirzapour, P.; Behnezhad, F.; Noori, T.; et al. Reinfection risk of novel coronavirus (COVID-19): A systematic review of current evidence. World J. Virol. 2020, 9, 79–90. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. COVID-19 Breakthrough Infections in Vaccinated Health Care Workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef]
- Estofolete, C.F.; Banho, C.A.; Campos, G.R.F.; Marques, B.C.; Sacchetto, L.; Ullmann, L.S.; Possebon, F.S.; Machado, L.F.; Syrio, J.D.; Araújo Junior, J.P.; et al. Case Study of Two Post Vaccination SARS-CoV-2 Infections with P1 Variants in CoronaVac Vaccinees in Brazil. Viruses 2021, 13, 1237. [Google Scholar] [CrossRef]
- Fabiani, M.; Margiotti, K.; Viola, A.; Mesoraca, A.; Giorlandino, C. Mild Symptomatic SARS-CoV-2 P.1 (B.1.1.28) Infection in a Fully Vaccinated 83-Year-Old Man. Pathogens 2021, 10, 614. [Google Scholar] [CrossRef]
- Philomina, J.B.; Jolly, B.; John, N.; Bhoyar, R.C.; Majeed, N.; Senthivel, V.; Cp, F.; Rophina, M.; Vasudevan, B.; Imran, M.; et al. Genomic survey of SARS-CoV-2 vaccine breakthrough infections in healthcare workers from Kerala, India. J. Infect. 2021, 83, 237–279. [Google Scholar] [CrossRef]
- Hacisuleyman, E.; Hale, C.; Saito, Y.; Blachere, N.E.; Bergh, M.; Conlon, E.G.; Schaefer-Babajew, D.J.; DaSilva, J.; Muecksch, F.; Gaebler, C.; et al. Vaccine Breakthrough Infections with SARS-CoV-2 Variants. N. Engl. J. Med. 2021, 384, 2212–2218. [Google Scholar] [CrossRef] [PubMed]
- Kroidl, I.; Mecklenburg, I.; Schneiderat, P.; Müller, K.; Girl, P.; Wölfel, R.; Sing, A.; Dangel, A.; Wieser, A.; Hoelscher, M. Vaccine breakthrough infection and onward transmission of SARS-CoV-2 Beta (B.1.351) variant, Bavaria, Germany, February to March 2021. Eurosurveillance 2021, 26, 2100673. [Google Scholar] [CrossRef] [PubMed]
- Almaghrabi, R.S.; Alhamlan, F.S.; Dada, A.; Al-Tawfiq, J.A.; Al Hroub, M.K.; Saeedi, M.F.; Alamri, M.; Alhothaly, B.; Alqasabi, A.; Al-Qahtani, A.A.; et al. Outcome of SARS-CoV-2 variant breakthrough infection in fully immunized solid organ transplant recipients. J. Infect. Public Health 2022, 15, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Olsen, R.J.; Christensen, P.A.; Long, S.W.; Subedi, S.; Hodjat, P.; Olson, R.; Nguyen, M.; Davis, J.J.; Yerramilli, P.; Saavedra, M.O.; et al. Trajectory of Growth of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Variants in Houston, Texas, January through May 2021, Based on 12,476 Genome Sequences. Am. J. Pathol. 2021, 191, 1754–1773. [Google Scholar] [CrossRef]
- Schmidt, T.; Klemis, V.; Schub, D.; Schneitler, S.; Reichert, M.C.; Wilkens, H.; Sester, U.; Sester, M.; Mihm, J. Cellular immunity predominates over humoral immunity after homologous and heterologous mRNA and vector-based COVID-19 vaccine regimens in solid organ transplant recipients. Am. J. Transplant. 2021, 21, 3990–4002. [Google Scholar] [CrossRef]
- Chau, N.V.V.; Ngoc, N.M.; Nguyet, L.A.; Quang, V.M.; Ny, N.T.H.; Khoa, D.B.; Phong, N.T.; Toan, L.M.; Hong, N.T.; Tuyen, N.T.K.; et al. An observational study of breakthrough SARS-CoV-2 Delta variant infections among vaccinated healthcare workers in Vietnam. EClinicalMedicine 2021, 41, 101143. [Google Scholar] [CrossRef]
- Connor, B.A.; Couto-Rodriguez, M.; Barrows, J.E.; Gardner, M.; Rogova, M.; O’Hara, N.B.; Nagy-Szakal, D. Monoclonal Antibody Therapy in a Vaccine Breakthrough SARS-CoV-2 Hospitalized Delta (B1.617.2) Variant Case. Int. J. Infect. Dis. 2021, 110, 232–234. [Google Scholar] [CrossRef]
- Gharpure, R.; Sami, S.; Vostok, J.; Johnson, H.; Hall, N.; Foreman, A.; Sabo, R.T.; Schubert, P.L.; Shephard, H.; Brown, V.R.; et al. Multistate Outbreak of SARS-CoV-2 Infections, Including Vaccine Breakthrough Infections, Associated with Large Public Gatherings, United States. Emerg. Infect. Dis. 2022, 28, 35–43. [Google Scholar] [CrossRef]
- Galán-Huerta, K.A.; Flores-Treviño, S.; Salas-Treviño, D.; Bocanegra-Ibarias, P.; Rivas-Estilla, A.M.; Pérez-Alba, E.; Lozano-Sepúlveda, S.A.; Arellanos-Soto, D.; Camacho-Ortiz, A. Prevalence of SARS-CoV-2 Variants of Concern and Variants of Interest in COVID-19 Breakthrough Infections in a Hospital in Monterrey, Mexico. Viruses 2022, 14, 154. [Google Scholar] [CrossRef]
- Deng, X.; Evdokimova, M.; O’Brien, A.; Rowe, C.L.; Clark, N.M.; Harrington, A.; Reid, G.E.; Uprichard, S.L.; Baker, S.C. Breakthrough Infections with Multiple Lineages of SARS-CoV-2 Variants Reveals Continued Risk of Severe Disease in Immunosuppressed Patients. Viruses 2021, 13, 1743. [Google Scholar] [CrossRef]
- De Souza, W.M.; Muraro, S.P.; Souza, G.F.; Amorim, M.R.; Sesti-Costa, R.; Mofatto, L.S.; Forato, J.; Barbosa, P.P.; Toledo-Teixeira, D.A.; Bispo-Dos-Santos, K.; et al. Clusters of SARS-CoV-2 Lineage B.1.1.7 Infection after Vaccination with Adenovirus-Vectored and Inactivated Vaccines. Viruses 2021, 13, 2127. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Kaur, H.; Yadav, P.D.; Mukhopadhyay, L.; Sahay, R.R.; Kumar, A.; Nyayanit, D.A.; Shete, A.M.; Patil, S.; Majumdar, T.; et al. Clinical Characterization and Genomic Analysis of Samples from COVID-19 Breakthrough Infections during the Second Wave among the Various States of India. Viruses 2021, 13, 1782. [Google Scholar] [CrossRef] [PubMed]
- Kale, P.; Gupta, E.; Bihari, C.; Patel, N.; Rooge, S.; Pandey, A.; Bajpai, M.; Khillan, V.; Chattopadhyay, P.; Devi, P.; et al. Vaccine Breakthrough Infections by SARS-CoV-2 Variants after ChAdOx1 nCoV-19 Vaccination in Healthcare Workers. Vaccines 2021, 10, 54. [Google Scholar] [CrossRef]
- Schulte, B.; Marx, B.; Korencak, M.; Emmert, D.; Aldabbagh, S.; Eis-Hübinger, A.M.; Streeck, H. Case Report: Infection With SARS-CoV-2 in the Presence of High Levels of Vaccine-Induced Neutralizing Antibody Responses. Front. Med. 2021, 8, 704719. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, S.; Mani, K.; Lodha, R.; Bakhshi, S.; Mathur, V.P.; Gupta, P.; Kedia, S.; Sankar, J.; Kumar, P.; Kumar, A.; et al. SARS-CoV-2 Reinfection Rate and Estimated Effectiveness of the Inactivated Whole Virion Vaccine BBV152 Against Reinfection Among Health Care Workers in New Delhi, India. JAMA Netw. Open 2022, 5, e2142210. [Google Scholar] [CrossRef]
- Shastri, J.; Parikh, S.; Aggarwal, V.; Agrawal, S.; Chatterjee, N.; Shah, R.; Devi, P.; Mehta, P.; Pandey, R. Severe SARS-CoV-2 Breakthrough Reinfection with Delta Variant After Recovery from Breakthrough Infection by Alpha Variant in a Fully Vaccinated Health Worker. Front. Med. 2021, 8, 737007. [Google Scholar] [CrossRef] [PubMed]
- Rovida, F.; Cassaniti, I.; Paolucci, S.; Percivalle, E.; Sarasini, A.; Piralla, A.; Giardina, F.; Sammartino, J.C.; Ferrari, A.; Bergami, F.; et al. SARS-CoV-2 vaccine breakthrough infections with the alpha variant are asymptomatic or mildly symptomatic among health care workers. Nat. Commun. 2021, 12, 6032. [Google Scholar] [CrossRef]
- Rümke, L.W.; Groenveld, F.C.; van Os, Y.M.G.; Praest, P.; Tanja, A.A.N.; de Jong, D.T.C.M.; Symons, J.; Schuurman, R.; Reinders, T.; Hofstra, L.M.; et al. In-depth Characterization of Vaccine Breakthrough Infections With SARS-CoV-2 Among Health Care Workers in a Dutch Academic Medical Center. Open Forum Infect. Dis. 2021, 9, ofab553. [Google Scholar] [CrossRef]
- Yi, S.; Kim, J.M.; Choe, Y.J.; Hong, S.; Choi, S.; Ahn, S.B.; Kim, M.; Park, Y.J. SARS-CoV-2 Delta Variant Breakthrough Infection and Onward Secondary Transmission in Household. J. Korean Med. Sci. 2022, 37, e12. [Google Scholar] [CrossRef]
- Robilotti, E.V.; Whiting, K.; Lucca, A.; Poon, C.; Guest, R.; McMillen, T.; Jani, K.; Solovyov, A.; Kelson, S.; Browne, K.; et al. Clinical and Genomic Characterization of SARS-CoV-2 infections in mRNA Vaccinated Health Care Personnel in New York City. Clin. Infect. Dis. 2021, ciab886. [Google Scholar] [CrossRef]
- Vignier, N.; Bérot, V.; Bonnave, N.; Peugny, S.; Ballet, M.; Jacoud, E.; Michaud, C.; Gaillet, M.; Djossou, F.; Blanchet, D.; et al. Breakthrough Infections of SARS-CoV-2 Gamma Variant in Fully Vaccinated Gold Miners, French Guiana, 2021. Emerg. Infect. Dis. 2021, 27, 2673–2676. [Google Scholar] [CrossRef] [PubMed]
- Tober-Lau, P.; Schwarz, T.; Hillus, D.; Spieckermann, J.; Helbig, E.T.; Lippert, L.J.; Thibeault, C.; Koch, W.; Bergfeld, L.; Niemeyer, D.; et al. Outbreak of SARS-CoV-2 B.1.1.7 Lineage after Vaccination in Long-Term Care Facility, Germany, February–March 2021. Emerg. Infect. Dis. 2021, 27, 2169–2173. [Google Scholar] [CrossRef] [PubMed]
- Servellita, V.; Morris, M.K.; Sotomayor-Gonzalez, A.; Gliwa, A.S.; Torres, E.; Brazer, N.; Zhou, A.; Hernandez, K.T.; Sankaran, M.; Wang, B.; et al. Predominance of antibody-resistant SARS-CoV-2 variants in vaccine breakthrough cases from the San Francisco Bay Area, California. Nat. Microbiol. 2022, 7, 277–288. [Google Scholar] [CrossRef] [PubMed]
- Singer, S.R.; Angulo, F.J.; Swerdlow, D.L.; McLaughlin, J.M.; Hazan, I.; Ginish, N.; Anis, E.; Mendelson, E.; Mor, O.; Zuckerman, N.S.; et al. Effectiveness of BNT162b2 mRNA COVID-19 vaccine against SARS-CoV-2 variant Beta (B.1.351) among persons identified through contact tracing in Israel: A prospective cohort study. EClinicalMedicine 2021, 42, 101190. [Google Scholar] [CrossRef] [PubMed]
- Thangaraj, J.W.V.; Yadav, P.; Kumar, C.G.; Shete, A.; Nyayanit, D.A.; Rani, D.S.; Kumar, A.; Kumar, M.S.; Sabarinathan, R.; Saravana Kumar, V.; et al. Predominance of delta variant among the COVID-19 vaccinated and unvaccinated individuals, India, May 2021. J. Infect. 2022, 84, 94–118. [Google Scholar] [CrossRef] [PubMed]
- Motozono, C.; Toyoda, M.; Zahradnik, J.; Saito, A.; Nasser, H.; Tan, T.S.; Ngare, I.; Kimura, I.; Uriu, K.; Kosugi, Y.; et al. SARS-CoV-2 spike L452R variant evades cellular immunity and increases infectivity. Cell Host Microbe 2021, 29, 1124–1136. [Google Scholar] [CrossRef]
- Singh, U.B.; Rophina, M.; Chaudhry, R.; Senthivel, V.; Bala, K.; Bhoyar, R.C.; Jolly, B.; Jamshed, N.; Imran, M.; Gupta, R.; et al. Variants of concern responsible for SARS-CoV-2 vaccine breakthrough infections from India. J. Med. Virol. 2022, 94, 1696–1700. [Google Scholar] [CrossRef]
- Tay, M.Z.; Rouers, A.; Fong, S.W.; Goh, Y.S.; Chan, Y.H.; Chang, Z.W.; Xu, W.; Tan, C.W.; Chia, W.N.; Torres-Ruesta, A.; et al. Decreased memory B cell frequencies in COVID-19 delta variant vaccine breakthrough infection. EMBO Mol. Med. 2022, 14, e15227. [Google Scholar] [CrossRef]
- Sun, J.; Zheng, Q.; Madhira, V.; Olex, A.L.; Anzalone, A.J.; Vinson, A.; Singh, J.A.; French, E.; Abraham, A.G.; Mathew, J.; et al. Association Between Immune Dysfunction and COVID-19 Breakthrough Infection After SARS-CoV-2 Vaccination in the US. JAMA Intern. Med. 2022, 182, 153–162. [Google Scholar] [CrossRef]
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.M.; Wang, W.; Song, Z.G.; Hu, Y.; Tao, Z.W.; Tian, J.H.; Pei, Y.Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [Green Version]
- GISAID. Tracking of Variants. 2022. Available online: https://www.gisaid.org/hcov19-variants (accessed on 5 March 2022).
- Piccoli, L.; Park, Y.J.; Tortorici, M.A.; Czudnochowski, N.; Walls, A.C.; Beltramello, M.; Silacci-Fregni, C.; Pinto, D.; Rosen, L.E.; Bowen, J.E.; et al. Mapping Neutralizing and Immunodominant Sites on the SARS-CoV-2 Spike Receptor-Binding Domain by Structure-Guided High-Resolution Serology. Cell 2020, 183, 1024–1042.e21. [Google Scholar] [CrossRef] [PubMed]
- Starr, T.N.; Greaney, A.J.; Addetia, A.; Hannon, W.W.; Choudhary, M.C.; Dingens, A.S.; Li, J.Z.; Bloom, J.D. Prospective mapping of viral mutations that escape antibodies used to treat COVID-19. Science 2021, 371, 850–854. [Google Scholar] [CrossRef] [PubMed]
- Zhou, D.; Dejnirattisai, W.; Supasa, P.; Liu, C.; Mentzer, A.J.; Ginn, H.M.; Zhao, Y.; Duyvesteyn, H.M.E.; Tuekprakhon, A.; Nutalai, R.; et al. Evidence of escape of SARS-CoV-2 variant B.1.351 from natural and vaccine-induced sera. Cell 2021, 184, 2348–2361.e6. [Google Scholar] [CrossRef] [PubMed]
- Cele, S.; Gazy, I.; Jackson, L.; Hwa, S.; Tegally, H.; Lustig, G.; Giandhari, J.; Pillay, S.; Wilkinson, E.; Naidoo, Y.; et al. Escape of SARS-CoV-2 501Y.V2 from neutralization by convalescent plasma. Nature 2021, 593, 142–146. [Google Scholar] [CrossRef]
- Wang, P.; Casner, R.G.; Nair, M.S.; Wang, M.; Yu, J.; Cerutti, G.; Liu, L.; Kwong, P.D.; Huang, Y.; Shapiro, L.; et al. Increased resistance of SARS-CoV-2 variant P.1 to antibody neutralization. Cell Host Microbe 2021, 29, 747–751.e4. [Google Scholar] [CrossRef]
- Starr, T.N.; Greaney, A.J.; Hilton, S.K.; Ellis, D.; Crawford, K.H.D.; Dingens, A.S.; Navarro, M.J.; Bowen, J.E.; Tortorici, M.A.; Walls, A.C.; et al. Deep Mutational Scanning of SARS-CoV-2 Receptor Binding Domain Reveals Constraints on Folding and ACE2 Binding. Cell 2020, 182, 1295–1310.e20. [Google Scholar] [CrossRef]
- Zhang, L.; Jackson, C.B.; Mou, H.; Ojha, A.; Peng, H.; Quinlan, B.D.; Rangarajan, E.S.; Pan, A.; Vanderheiden, A.; Suthar, M.S.; et al. SARS-CoV-2 spike-protein D614G mutation increases virion spike density and infectivity. Nat. Commun. 2020, 11, 6013. [Google Scholar] [CrossRef]
- Hou, Y.J.; Chiba, S.; Halfmann, P.; Ehre, C.; Kuroda, M.; Dinnon, K.H., 3rd; Leist, S.R.; Schäfer, A.; Nakajima, N.; Takahashi, K.; et al. SARS-CoV-2 D614G variant exhibits efficient replication ex vivo and transmission in vivo. Science 2020, 370, 1464–1468. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease (COVID-19): Vaccines. 2022. Available online: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-(covid-19)-vaccines (accessed on 4 March 2022).
- Lythgoe, M.P.; Middleton, P. Comparison of COVID-19 Vaccine Approvals at the US Food and Drug Administration, European Medicines Agency, and Health Canada. JAMA Netw. Open. 2021, 4, e2114531. [Google Scholar] [CrossRef]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Robertson, C.; Stowe, J.; Tessier, E.; Simmons, R.; Cottrell, S.; Roberts, R.; O’Doherty, M.; et al. Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines on COVID-19 related symptoms, hospital admissions, and mortality in older adults in England: Test negative case-control study. BMJ 2021, 373, n1088. [Google Scholar] [CrossRef]
- Doria-Rose, N.; Suthar, M.S.; Makowski, M.; O’Connell, S.; McDermott, A.B.; Flach, B.; Ledgerwood, J.E.; Mascola, J.R.; Graham, B.S.; Lin, B.C.; et al. mRNA-1273 Study Group. Antibody Persistence through 6 Months after the Second Dose of mRNA-1273 Vaccine for COVID-19. N. Engl. J. Med. 2021, 384, 2259–2261. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Jiang, X.; Qu, M.; Aninwene, G.E.; Jucaud, V.; Moon, J.J.; Gu, Z.; Sun, W.; Khademhosseini, A. Engineering Antiviral Vaccines. ACS Nano 2020, 14, 12370–12389. [Google Scholar] [CrossRef] [PubMed]
- Mascellino, M.T.; Di Timoteo, F.; De Angelis, M.; Oliva, A. Overview of the Main Anti-SARS-CoV-2 Vaccines: Mechanism of Action, Efficacy and Safety. Infect. Drug Resist. 2021, 14, 3459–3476. [Google Scholar] [CrossRef] [PubMed]
- Halperin, S.A.; Ye, L.; MacKinnon-Cameron, D.; Smith, B.; Cahn, P.E.; Ruiz-Palacios, G.M.; Ikram, A.; Lanas, F.; Guerrero, M.L.; Navarro, S.R.M.; et al. CanSino COVID-19 Global Efficacy Study Group. Final efficacy analysis, interim safety analysis, and immunogenicity of a single dose of recombinant novel coronavirus vaccine (adenovirus type 5 vector) in adults 18 years and older: An international, multicentre, randomised, double-blinded, placebo-controlled phase 3 trial. Lancet 2022, 399, 237–248. [Google Scholar] [CrossRef]
- Barouch, D.H.; Stephenson, K.E.; Sadoff, J.; Yu, J.; Chang, A.; Gebre, M.; McMahan, K.; Liu, J.; Chandrashekar, A.; Patel, S.; et al. Durable Humoral and Cellular Immune Responses 8 Months after Ad26.COV2.S Vaccination. N. Engl. J. Med. 2021, 385, 951–953. [Google Scholar] [CrossRef]
- World Health Organization. The Janssen Ad26.COV2.S COVID-19 Vaccine: What You Need to Know. 2021. Available online: https://www.who.int/news-room/feature-stories/detail/the-j-j-covid-19-vaccine-what-you-need-to-know (accessed on 4 March 2022).
- Grifoni, A.; Weiskopf, D.; Ramirez, S.I.; Mateus, J.; Dan, J.M.; Moderbacher, C.R.; Rawlings, S.A.; Sutherland, A.; Premkumar, L.; Jadi, R.S.; et al. Targets of T Cell Responses to SARS-CoV-2 Coronavirus in Humans with COVID-19 Disease and Unexposed Individuals. Cell 2020, 181, 1489–1501.e15. [Google Scholar] [CrossRef]
- National Institute of Health. Adjuvant Developed with NIH Funding Enhances Efficacy of India’s COVID-19 Vaccine. 2021. Available online: https://www.nih.gov/news-events/news-releases/adjuvant-developed-nih-funding-enhances-efficacy-indias-covid-19-vaccine (accessed on 4 March 2022).
- Liu, Y.; Rocklöv, J. The reproductive number of the Delta variant of SARS-CoV-2 is far higher compared to the ancestral SARS-CoV-2 virus. J. Travel Med. 2021, 28, taab124. [Google Scholar] [CrossRef]
- Levine-Tiefenbrun, M.; Yelin, I.; Alapi, H.; Katz, R.; Herzel, E.; Kuint, J.; Chodick, G.; Gazit, S.; Patalon, T.; Kishony, R.; et al. Viral loads of Delta-variant SARS-CoV-2 breakthrough infections after vaccination and booster with BNT162b2. Nat. Med. 2021, 27, 2108–2110. [Google Scholar] [CrossRef]
- Sokal, A.; Barba-Spaeth, G.; Fernández, I.; Broketa, M.; Azzaoui, I.; de La Selle, A.; Vandenberghe, A.; Fourati, S.; Roeser, A.; Meola, A.; et al. mRNA vaccination of naive and COVID-19-recovered individuals elicits potent memory B cells that recognize SARS-CoV-2 variants. Immunity 2021, 54, 2893–2907.e5. [Google Scholar] [CrossRef]
- Abdool Karim, S.S.; de Oliveira, T. New SARS-CoV-2 Variants—Clinical, Public Health, and Vaccine Implications. N. Engl. J. Med. 2021, 384, 1866–1868. [Google Scholar] [CrossRef]
- Emary, K.R.W.; Golubchik, T.; Aley, P.K. Efficacy of ChAdOx1 nCoV-19 (AZD1222) vaccine against SARS-CoV-2 variant of concern 202012/01 (B.1.1.7): An exploratory analysis of a randomized controlled trial. Lancet 2021, 397, 1351–1362. [Google Scholar] [CrossRef]
- Liu, Z.; VanBlargan, L.A.; Bloyet, L.M.; Rothlauf, P.W.; Chen, R.E.; Stumpf, S.; Zhao, H.; Errico, J.M.; Theel, E.S.; Liebeskind, M.J.; et al. Identification of SARS-CoV-2 spike mutations that attenuate monoclonal and serum antibody neutralization. Cell Host Microbe 2021, 29, 477–488.e4. [Google Scholar] [CrossRef] [PubMed]
- Jangra, S.; Ye, C.; Rathnasinghe, R.; Stadlbauer, D.; Personalized Virology Initiative Study Group; Krammer, F.; Simon, V.; Martinez-Sobrido, L.; García-Sastre, A.; Schotsaert, M.; et al. SARS-CoV-2 spike E484K mutation reduces antibody neutralisation. Lancet Microbe 2021, 2, e283–e284. [Google Scholar] [CrossRef]
- Li, Q.; Nie, J.; Wu, J.; Zhang, L.; Ding, R.; Wang, H.; Zhang, Y.; Li, T.; Liu, S.; Zhang, M.; et al. SARS-CoV-2 501Y.V2 variants lack higher infectivity but do have immune escape. Cell 2021, 184, 2362–2371.e9. [Google Scholar] [CrossRef]
- Greaney, A.J.; Starr, T.N.; Barnes, C.O.; Weisblum, Y.; Schmidt, F.; Caskey, M.; Gaebler, C.; Cho, A.; Agudelo, M.; Finkin, S.; et al. Mapping mutations to the SARS-CoV-2 RBD that escape binding by different classes of antibodies. Nat. Commun. 2021, 12, 4196. [Google Scholar] [CrossRef] [PubMed]
- Starr, T.N.; Greaney, A.J.; Dingens, A.S.; Bloom, J.D. Complete map of SARS-CoV-2 RBD mutations that escape the monoclonal antibody LY-CoV555 and its cocktail with LY-CoV016. Cell Rep. Med. 2021, 2, 100255. [Google Scholar] [CrossRef] [PubMed]
- Baj, A.; Novazzi, F.; Pasciuta, R.; Genoni, A.; Ferrante, F.D.; Valli, M.; Partenope, M.; Tripiciano, R.; Ciserchia, A.; Catanoso, G.; et al. Breakthrough Infections of E484K-Harboring SARS-CoV-2 Delta Variant, Lombardy, Italy. Emerg. Infect. Dis. 2021, 27, 3180–3182. [Google Scholar] [CrossRef]
- García, L.F. Immune Response, Inflammation, and the Clinical Spectrum of COVID-19. Front. Immunol. 2020, 11, 1441. [Google Scholar] [CrossRef]
- Zani, A.; Caccuri, F.; Messali, S.; Bonfanti, C.; Caruso, A. Serosurvey in BNT162b2 vaccine-elicited neutralizing antibodies against authentic B.1, B.1.1.7, B.1.351, B.1.525 and P.1 SARS-CoV-2 variants. Emerg. Microbes Infect. 2021, 10, 1241–1243. [Google Scholar] [CrossRef]
- Edridge, A.W.D.; Kaczorowska, J.; Hoste, A.C.R.; Bakker, M.; Klein, M.; Loens, K.; Jebbink, M.F.; Matser, A.; Kinsella, C.M.; Rueda, P.; et al. Seasonal coronavirus protective immunity is short-lasting. Nat. Med. 2020, 26, 1691–1693. [Google Scholar] [CrossRef]
- Becker, M.; Dulovic, A.; Junker, D.; Ruetalo, N.; Kaiser, P.D.; Pinilla, Y.T.; Heinzel, C.; Haering, J.; Traenkle, B.; Wagner, T.R.; et al. Immune response to SARS-CoV-2 variants of concern in vaccinated individuals. Nat. Commun. 2021, 12, 3109. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Schmidt, F.; Weisblum, Y.; Muecksch, F.; Barnes, C.O.; Finkin, S.; Schaefer-Babajew, D.; Cipolla, M.; Gaebler, C.; Lieberman, J.A.; et al. mRNA vaccine-elicited antibodies to SARS-CoV-2 and circulating variants. Nature 2021, 592, 616–622. [Google Scholar] [CrossRef] [PubMed]
- Hall, V.G.; Ferreira, V.H.; Ierullo, M.; Ku, T.; Marinelli, T.; Majchrzak-Kita, B.; Yousuf, A.; Kulasingam, V.; Humar, A.; Kumar, D.; et al. Humoral and cellular immune response and safety of two-dose SARS-CoV-2 mRNA-1273 vaccine in solid organ transplant recipients. Am. J. Transplant. 2021, 21, 3980–3989. [Google Scholar] [CrossRef] [PubMed]
- Holden, I.K.; Bistrup, C.; Nilsson, A.C.; Hansen, J.F.; Abazi, R.; Davidsen, J.R.; Poulsen, M.K.; Lindvig, S.O.; Justesen, U.S.; Johansen, I.S.; et al. Immunogenicity of SARS-CoV-2 mRNA vaccine in solid organ transplant recipients. J. Intern. Med. 2021, 290, 1264–1267. [Google Scholar] [CrossRef] [PubMed]
- Chavarot, N.; Morel, A.; Leruez-Ville, M.; Vilain, E.; Divard, G.; Burger, C.; Serris, A.; Sberro-Soussan, R.; Martinez, F.; Amrouche, L.; et al. Weak antibody response to three doses of mRNA vaccine in kidney transplant recipients treated with belatacept. Am. J. Transplant. 2021, 21, 4043–4051. [Google Scholar] [CrossRef]
- Shroff, R.T.; Chalasani, P.; Wei, R.; Pennington, D.; Quirk, G.; Schoenle, M.V.; Peyton, K.L.; Uhrlaub, J.L.; Ripperger, T.J.; Jergović, M.; et al. Immune responses to two and three doses of the BNT162b2 mRNA vaccine in adults with solid tumors. Nat. Med. 2021, 27, 2002–2011. [Google Scholar] [CrossRef] [PubMed]
- Kamar, N.; Abravanel, F.; Marion, O.; Couat, C.; Izopet, J.; Del Bello, A. Three doses of an mRNA COVID-19 vaccine in solid-organ transplant recipients. N. Engl. J. Med. 2021, 385, 661–662. [Google Scholar] [CrossRef]
- Food and Drug Administration. Coronavirus (COVID-19) Update: FDA Authorizes New Long-Acting Monoclonal Antibodies for Pre-exposure Prevention of COVID-19 in Certain Individuals. 2021. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-new-long-acting-monoclonal-antibodies-pre-exposure (accessed on 4 March 2022).
- O’Brien, M.P.; Forleo-Neto, E.; Musser, B.J.; Isa, F.; Chan, K.C.; Sarkar, N.; Bar, K.J.; Barnabas, R.V.; Barouch, D.H.; Cohen, M.S.; et al. Subcutaneous REGEN-COV Antibody Combination to Prevent COVID-19. N. Engl. J. Med. 2021, 385, 1184–1195. [Google Scholar] [CrossRef]
- Chen, R.E.; Zhang, X.; Case, J.B.; Winkler, E.S.; Liu, Y.; VanBlargan, L.A.; Liu, J.; Errico, J.M.; Xie, X.; Suryadevara, N.; et al. Resistance of SARS-CoV-2 variants to neutralization by monoclonal and serum-derived polyclonal antibodies. Nat. Med. 2021, 27, 717–726. [Google Scholar] [CrossRef]
- Richman, D.D. COVID-19 vaccines: Implementation, limitations, and opportunities. Glob. Health Med. 2021, 3, 1–5. [Google Scholar] [CrossRef]
- Nomura, Y.; Sawahata, M.; Nakamura, Y.; Kurihara, M.; Koike, R.; Katsube, O.; Hagiwara, K.; Niho, S.; Masuda, N.; Tanaka, T.; et al. Age and Smoking Predict Antibody Titres at 3 Months after the Second Dose of the BNT162b2 COVID-19 Vaccine. Vaccines 2021, 9, 1042. [Google Scholar] [CrossRef] [PubMed]
- De Gier, B.; de Oliveira Bressane Lima, P.; van Gaalen, R.D.; de Boer, P.T.; Alblas, J.; Ruijten, M.; van Gageldonk-Lafeber, A.B.; Waegemaekers, T.; Schreijer, A.; van den Hof, S.; et al. Occupation- and age-associated risk of SARS-CoV-2 test positivity, the Netherlands, June to October 2020. Eurosurveillance 2020, 25, 2001884. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Prevention, Identification, and Management of Health Worker Infection in the Context of COVID-19. 2020. Available online: https://www.who.int/publications/i/item/10665-336265 (accessed on 4 March 2022).
- Chou, R.; Dana, T.; Buckley, D.I.; Selph, S.; Fu, R.; Totten, A.M. Epidemiology of and Risk Factors for Coronavirus Infection in Health Care Workers: A Living Rapid Review. Ann. Intern. Med. 2020, 173, 120. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, L.; Levinsky, Y.; Marcus, N.; Hoffer, V.; Gafner, M.; Hadas, S.; Kraus, S.; Mor, M.; Scheuerman, O. SARS-CoV-2 Infection among Health Care Workers Despite the Use of Surgical Masks and Physical Distancing-the Role of Airborne Transmission. Open Forum Infect. Dis. 2021, 8, ofab036. [Google Scholar] [CrossRef]
- Teran, R.A.; Walblay, K.A.; Shane, E.L.; Xydis, S.; Gretsch, S.; Gagner, A.; Samala, U.; Choi, H.; Zelinski, C.; Black, S.R.; et al. Postvaccination SARS-CoV-2 infections among skilled nursing facility residents and staff members—Chicago, Illinois, December 2020–March 2021. Am. J. Transplant. 2021, 21, 2290–2297. [Google Scholar] [CrossRef]
- Nordström, P.; Ballin, M.; Nordström, A. Effectiveness of heterologous ChAdOx1 nCoV-19 and mRNA prime-boost vaccination against symptomatic COVID-19 infection in Sweden: A nationwide cohort study. Lancet Reg. Health Eur. 2021, 11, 100249. [Google Scholar] [CrossRef]
- Gram, M.A.; Nielsen, J.; Schelde, A.B.; Nielsen, K.F.; Moustsen-Helms, I.R.; Sørensen, A.K.B.; Valentiner-Branth, P.; Emborg, H.D. Vaccine effectiveness against SARS-CoV-2 infection, hospitalization, and death when combining a first dose ChAdOx1 vaccine with a subsequent mRNA vaccine in Denmark: A nationwide population-based cohort study. PLoS Med. 2021, 18, e1003874. [Google Scholar] [CrossRef]
- Bignardi, E.; Brogna, C.; Capasso, C.; Brogna, B. A fatal case of COVID-19 breakthrough infection due to the delta variant. Clin. Case Rep. 2022, 10, e05232. [Google Scholar] [CrossRef]


{kind=link}
| Study | Type of Study | Number of Fully Vaccinated Individuals (Breakthrough Infections) | Country | Gender | Age (Years) | Number of Days since Vaccination | Vaccine Received | Symptoms | Comorbidities | Variants [Reported Mutations] | Ct (Cycle Threshold) Value | Complications & Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bergwerk et al., 2021 [11] | Case control | 11,453 (39) | Israel | Females: 25; Males:14 | Mean: 42 | Median: 39 (Range: 11–102) | BNT162b2 (Pfizer-BioNTech) | Upper respiratory congestion (36%), myalgia (28%), loss of smell or taste(28%); fever or rigors (21%); Asymptomatic (33%) | Immunosuppressed (1), CLL*(1), ITP*(1), metabolic syndrome (6), thyroid disorder (3), other (migraines, fibromyalgia, osteoporosis, PCOS*) (4) | Alpha (B.1.1.7): 85% of samples | <30 (74%); >30 (26%) | Recovery |
| Estofolete et al., 2021 [12] | Case Report | 2 (2) | Brazil | Male | 60 | 106 | Corona Vac (Sinovac) | Anosmia, malaise, myalgia, dyspnea | Type 2 diabetes mellitus, hypertension, obesity degree I (BMI*: 32.3 kg/m2) | Gamma (P.1) [K417T, E4844K, N501Y] | Unknown | Hospitalization with supplemental oxygen → Recovery |
| 55 | 122 | Sore throat, headache, malaise, chills, coryza, sneezing, dyspnea, hypoxia | None | |||||||||
| Fabiani et al., 2021 [13] | Case Report | 1 (1) | Italy | Male | 83 | 23 | BNT162b2(Pfizer-BioNTech) | Slight headache, mild cold | None | Gamma (P.1) [K417T, E484K, N501Y, D614G] | 13 | Recovery |
| Philomina et al., 2021 [14] | Retrospective cohort | 6 (6) | India | Female | 25 | 35 | AZD1222/Covishield (SII) | Influenza-like illness | Unknown | B.1.1.306 [E484K] | 16.45 | Recovery |
| Male | 50 | 30 | Fever, malaise, anosmia, headache | Alpha (B.1.1.7) [N501Y] | 20 | |||||||
| Female | 53 | 28 | Rhinitis | 21 | ||||||||
| 25 | 26 | Fever, loose stools, abdominal pain, dry cough, myalgia, rhinitis, anosmia | 24 | |||||||||
| 32 | 25 | Mild nasal congestion, headache | 26 | |||||||||
| 33 | 17 | Loss of smell, loose stools, rhinitis | B.1.1 B.1.560 [S477N] | 14 | ||||||||
| Hacisuleyman et al., 2021 [15] | Prospective cohort | 417 (2) | USA | Female | 51 | 19 | mRNA-1273 (Moderna) | Sore throat, congestion, headache, anosmia | None | Alpha (B.1.1.7) [E484K D614G T95I, del142–144] | 24.2 | Recovery |
| 65 | 36 | BNT162b2 (Pfizer–BioNTech) | Fatigue, sinus congestion, headache | Alpha (B.1.1.7) [S477N T95I, del142–144 R190T F2201 R237K R246T D614G] | 33.3 | |||||||
| Kroidl et al., 2021 [16] | Case report | 1 (1) | Germany | Unknown | Early ‘60s | 26 | BNT162b2 (Pfizer–BioNTech) | Headache, congested nose | None | Beta (B.1.351) | Unknown | Recovery |
| Almaghrabi et al., 2022 [17] | Case series | 4 (4) | Saudi Arabia | Male | 68 | 73 | BNT162b2 (Pfizer-BioNTech) | Fever, chills, vomiting | Liver transplant, diabetes mellitus, hypertension, immunosuppressive medication | Alpha (B.1.1.7) [E484K] | 25 | Severe pneumonia →Mechanical ventilation →Death |
| 69 | 150 | Shortness of breath, hypoxia | Renal transplant, diabetes mellitus, hypertension, immunosuppressive medication | Alpha (B.1.1.7) | 30 | Pneumonia → Mechanical ventilation, septic shock →Death | ||||||
| 41 | 39 | Mild coughs, shortness of breath | Renal transplant, immunosuppressive medications | Beta (B.1.351) | 29 | ICU* admission with HFNC*→ Recovery | ||||||
| Female | 48 | 21 | ChAdOx1 nCoV-19 vaccine (AstraZeneca) | Fever, hypoxia | Renal transplant, post-transplant lymphoma, immunosuppressive medications | Delta (B.1.617.2) | 19 | Hospital acquired infection, HFNC*→ Recovery | ||||
| Baj et al., 2021 [18] | Retrospective cohort Study | 4 (4) | Italy | Female | 80 | 77 | mRNA-1273 (Moderna) | Fatigue, headache, myalgia, dyspnea | Unknown | Delta (B.1.617.2)[E484K] | 22 | Recovery |
| Male | 77 | 67 | Pfizer-BioNTech (BNT162b2) | Fever | 19 | |||||||
| Female | 83 | 87 | BNT162b2 (Pfizer-BioNTech) | Fever, fatigue, ageusia, anosmia | 18 | |||||||
| Female | 81 | 45 | mRNA-1273 (Moderna) | Dyspnea, fever, myalgia, fatigue | 21 | Hospital admission → Recovery | ||||||
| Bignardi et al., 2022 [19] | Case report | 1 (1) | Italy | Male | 61 | 120 | mRNA vaccine -type not specified | Dyspnea, cough, fever | Hypertension, obesity | Delta (B.1.617.2) | Unknown | Pneumonia → Death |
| Chau et al., 2021 [20] | Cohort | 866 (62) a | Vietnam | Females: 29 Males:33 | Median: 41.5 (IQR: 32–50) | 49–56 (97%) | Oxford-AstraZeneca | Fever (27%), cough (37%), sore throat (34%), runny nose (36%), loss of smell (39%), loss of taste (8%), muscle pain (27%), headache (19%), chest pain (3%), nausea (8%), shortness of breath (4%), pneumonia (5%), asymptomatic (21%) | Overweight (6), obesity (3), hypertension (3), hepatitis B (3), diabetes mellitus (2), pregnancy (1) | Delta (B.1.617.2) | 31.9 (IQR: 23.3–34.9) | Recovery |
| Connor et al., 2021 [21] | Case report | 2 (2) | USA | Male | 63 | 60 | BNT162b2 (Pfizer-BioNTech) | Nasal congestion, headache, dry cough | Hypertension, benign prostatic hypertrophy, overweight | B.1.617.2 B.1.619 [35 mutations detected, including 9 in the spike protein] | 31.3 | Recovery |
| 25 | 90 | Upper respiratory symptoms, headaches | None | B.1.617.2 [7/12 shared S-gene mutations] | 25.2 | Recovery | ||||||
| Gharpure et al., 2022 [22] | Cohort | 1128 (918) | USA | Females: 90 Males: 822 | 19–49 (66%), 50–64 (30%), 65–74 (4%), >75 (0.4%) | >14 | BNT162b2 (Pfizer-BioNTech): 504 mRNA-1273 (Moderna): 293 Johnson & Johnson: 121 | Abdominal pain (6%), chills (35%),congestion (58%),cough (73%), diarrhea(20%), shortness of breath (10%), fatigue (41%), fever (43%), headache (47%), loss of appetite (16%), loss of smell or taste (50%), muscle pain (39%), sore throat (42%), vomiting (3%) | Active cancer (3), autoimmune disease (11), cardiovascular disease (36), chronic kidney disease (3), chronic lung disease (22), pregnancy (3), diabetes mellitus (21), HIV* infection (6), solid organ transplant (1), other immunosuppressive conditions (41) | Delta (B.1.617.2): 98%Delta (AY.3 sublineage:0.3%, Delta (AY.4 sublineage): 0.8% Gamma (P.1): 0.8% | Unknown | Hospitalized (7), ICU* (2) → Recovery |
| Galan Huerta et al., 2022 [23] | Case-control | 53 (53) | Mexico | Females: 28; Males: 25 | Mean: 59.7 (50–70) | 7 | AstraZeneca/Oxford: 8 (15%) BNT162b2 (Pfizer/BioNTech): 8 (15%) Convidecia(CanSino): 24 (45%) CoronoVac (Sinovac): 10 (19%) Unspecified: 3 | Mostly mild or asymptomatic | Hospitalized: hypertension (11), Type 2 diabetes mellitus (13), obesity (1), smoking (4); Ambulatory: hypertension (5), Type 2 diabetes mellitus (5), obesity (2), smoking (1) | Delta (B.1.617.2) (AY.1, AY.2, AY.3, AY.4 lineage): 67.92% Gamma (P.1, P.1.1, P.1.2): 7.55% Mu (B.1.621): 7.55% Alpha (B.1.1.7): 5.66% | Hospitalized: 19.58 (17.19–22.49); Ambulatory: 18.81 (15.72–21.24) | Hospitalized: High-flow O2 (14), intubation (10), ICU* admission (1), death (4); Ambulatory: all recovered (30) |
| Deng et al., 2021 [24] | Case control | 14 (14) | USA | Female | 60 | Range: (14–109) | BNT162b2 (Pfizer-BioNTech) | Rhinorrhea | None | Alpha 20I/S: 501Y.V1 | 18.8 | Recovery |
| Male | 58 | Chill, subjective fever | None | Alpha (20I/S: 501Y.V1) | 19.1 | |||||||
| Female | 48 | Weakness, congestion loss of taste/smell, fatigue | Smoker | Alpha (20I/S: 501Y.V1) | 20.9 | |||||||
| 51 | mRNA vaccine type not provided | Headache, cough, rhinorrhea ageusia, anosmia | Immunosuppressive medication, non-alcoholic steatohepatitis | Gamma (20J/S: 501Y.V3) | 17.1 | |||||||
| 37 | mRNA-1273 (Moderna) | Asymptomatic | None | 20G | 19.5 | |||||||
| 50 | BNT162b2 (Pfizer-BioNTech) | Asymptomatic | None | Unknown | 34.2 | |||||||
| 81 | Johnson & Johnson | Shortness of breath, cough | Heart disease, cerebrovascular disease | Alpha (20I/S: 501Y.V1) | 18.8 | Hospitalization → recovery | ||||||
| Male | 65 | BNT162b2 (Pfizer-BioNTech) | Diarrhea, myalgia, chills, fever | Immunosuppressive medication, kidney, and heart transplant | Alpha (20I/S: 501Y.V1) | 20.1 | Pneumonia → recovery | |||||
| 55 | Cough, acute hypoxic respiratory failure, sepsis | Immunosuppressive medication, kidney transplant | Alpha (20I/S: 501Y.V1) | 22.3 | Intensive Care Unit (ICU) → Death | |||||||
| 70 | Cough, weakness, fever, dyspnea | Immunosuppressive medication, liver transplant | Gamma (20J/S: 501Y.V3) | 19.6 | Hospitalization → recovery | |||||||
| 68 | mRNA-1273 (Moderna) | Acute hypoxia, acute pneumonia, hemoptysis | Immunosuppressive medication, lung transplant | Gamma (20J/S: 501Y.V3) | 21.4 | |||||||
| Female | 60 | Shortness of breath, fever, chills, body aches, hypoxia | Immunosuppressive medication, lung transplant | Gamma (20J/S: 501Y.V3) | 15.7 | Intensive Care Unit (ICU) → Recovery | ||||||
| Male | 65 | BNT162b2 (Pfizer-BioNTech) | Diarrhea, nausea, weakness cough, dyspnea | Immunosuppressive medication, liver transplant | Epsilon (CAL.20C) | 22.1 | Hospitalization → Recovery | |||||
| Female | 76 | Fever, chills, acute respiratory failure | None | 20G | 18.3 | Intensive Care Unit (ICU) → Recovery | ||||||
| De Souza et al., 2021 [25] | Case control | 42 (22) | Brazil | Females: 17 Males: 5 | 77 (IQR: 51–87) | 5–27 | CoronaVac (SinoVac) | Asymptomatic (75%) Mild COVID-19 symptoms (25%) | Unknown | Alpha (B.1.1.7) | Unknown | Death: 1% Recovery: 99% |
| Gupta et al., 2021 [26] | Case control | 592 (592) | India | Females: 207; Males: 385 | Mean 44 (31–56) | 39 (19–58) | Covaxin: 71 (10.5%)Covishield (AstraZeneca): 604 (89.2%) Covilo (Sinopharm): 2 (0.3%) | Symptomatic (71%) with one or more symptoms, fever (69%), body ache, headache and nausea (56%), cough (45%), sore throat (37%), loss of smell and taste (22%), diarrhea (6%), breathlessness (6%), ocular irritation, redness (1%); Asymptomatic (29%) | Type 2 diabetes mellitus, hypertension, obesity, chronic cardiac, renal, and pulmonary diseases | Delta (B.1.617.2): 384 Alpha (B.1.1.7): 28) Kappa (B.1.617.1: 22 B.1.617.3: 2 B.1.36: 2 B.1.1.294: 1 B.1.36.16: 1 B.1.1.306: 1 Delta (AY.2): 2 | <30 | Fully vaccinated: hospitalized (53), Recovered (589), Death (3) |
| Kale et al., 2021 [27] | Cohort | 1639 (156) | India | Female: 86 Males: 70 | Median: 34 (IQR21–67) | >14 | ChAdOx1 nCoV-19/Covishield (SII) | Fever, muscle aches | Unknown | Delta (B.1.617.2): 32 Kappa (B.1.617.1):11 Alpha (B.1.1.7): 1 | 23.2 (IQR 0.0–33.1) | Recovery; Hospitalization (0.22%) |
| Schulte et al., 2021 [28] | Case report | 1 (1) | Germany | Male | 42 | 49 | BNT162b2 (Pfizer-BioNTech) | Asymptomatic | None | B.1.525 | 9.44 | Recovery |
| Malhotra et al., 2022 [29] | Retrospective cohort | 1079 (17) | India | Unknown | <25:72 (6.6%); 25–44: 660 (60.6%);≥ 45: 357 (32.8%) | >15 | BBV152/Covaxin (Bharat Biotech) | Symptomatic:-Fever, rhinorrhea, sore throat, cough, chest pain, wheezing, difficulty breathing, shortness of breath, anosmia, dysgeusia, fatigue, myalgia, headache, abdominal pain, nausea, diarrhea. Asymptomatic: 3 | Hypertension; chronic heart, lung, or kidney disease; cancer; hypothyroidism | Gamma (B.1.617.2) | Unknown | Recovery |
| Shastri et al., 2021 [30] | Case report | 1(1) b | India | Female | 61 | 28 | ChAdOx1 nCoV-19(Covishield) | 1st infection episode: Abdominal pain, fever, myalgia, fatigue 2nd infection episode: Body ache, fatigue, headache, cough, breathlessness, fever, rhinorrhea, vomiting | Prediabetes, bronchial asthma, hypertension | Alpha (B.1.1.7):1st Delta (B.1.617.2):2nd | 1st infection: 35.2 2nd infection: 20.4 | Recovery |
| Rovida et al., 2021 [31] | Cohort | 3702 (33) | Italy | Females:26 Males: 7 | Unknown | 47 (Range 7–90) | BNT162b2 (Pfizer-BioNTech) | Asymptomatic (48%), fever (6%), asthenia (6%), headache (6%), arthralgia (9%), pharyngodynia (3%), rhinitis (27%), cough (9%), cough (9%), anosmia (9%), ageusia (3%), nausea (9%), diarrhea (10%) | Unknown | Alpha (B.1.1.7) | Unknown | Recovery |
| Rumke et al., 2022 [32] | Cohort | 14 (14) | Netherlands | Female | 45 | 43 | BNT162b2 (Pfizer-BioNTech) | Anosmia, arthralgia, fever, headache, myalgia, peripheral neuropathy, rhinosinusitis | None | Alpha (B.1.1.7) | 18.5 | Recovery |
| 62 | 78 | Anosmia, rhinosinusitis | None | Alpha (B.1.1.7) | 23.7 | |||||||
| 27 | 64 | Rhinitis | None | Alpha (B.1.1.7) [A771V] | 23.5 | |||||||
| 52 | 61 | Cough, dyspnea, fever | Asthma | Alpha (B.1.1.7) | 19.6 | |||||||
| 35 | 74 | Anosmia, cough, rhinitis | None | Alpha (B.1.1.7) [H245Y] | 21.5 | |||||||
| 35 | 80 | Anosmia, rhinosinusitis | None | Alpha (B.1.1.7) [S494P] | 24.7 | |||||||
| Male | 58 | 80 | Asymptomatic | None | Alpha (B.1.1.7) | 31.9 | ||||||
| Female | 26 | 111 | Fever, rhinitis | None | Alpha (B.1.1.7) [V382L] | 19.8 | ||||||
| 38 | 38 | Ad26.COV2.S (Johnson & Johnson) | Cough, fever, pharyngitis, rhinosinusitis | None | Alpha (B.1.1.7) [D88V] | 18.9 | ||||||
| 57 | 37 | Cough, dyspnea | None | Alpha (B.1.1.7) [V483I, A706V] | 21.5 | |||||||
| 50 | 20 | Asymptomatic | None | Alpha (B.1.1.7) [S12F, D905N] | 23.6 | |||||||
| 54 | 45 | Cough, fever, headache, myalgia, otitis | Atopic dermatitis | Delta (B.617.2) | 31.3 | |||||||
| 38 | 18 | Asymptomatic | Hashimoto thyroiditis | Alpha (B.1.1.7) | 29.0 | |||||||
| 48 | 52 | Anosmia, fever, headache, myalgia, sinusitis | None | Delta (B.617.2) [G142D] | 29.2 | |||||||
| Yi et al., 2022 [33] | Cohort | 24 (24) | South Korea | Females:18 | 78.9 (Range 34–99) | Mean: 40 (Range, 80–117) | BNT162b2 (Pfizer-BioNTech) | Asymptomatic (48%) Symptomatic (48%) | Unknown | Delta (B.1.617.2):13 | 18.1 (symptomatic); 20 (asymptomatic) | Recovery (96%), Death (4%) |
| Robilotti et al., 202 [34] | Cohort | 12,046 (80: pre-Delta) | USA | Females: 60 Males: 20 | Median37 (Range:22–65) | Median: 56 (Range:1–100) | BNT162b2 (Pfizer-BioNTech): 91% mRNA-1273 (Moderna): 9% | Asymptomatic (20%) Headache (55%) Fatigue (45%) Body aches (28%) Fever (including subjective) (19%) Loss of smell/taste (28%) Chills (20%) Sore throat (21%) Rhinorrhea, nasal congestion, sneezing (53%) GI symptoms (nausea, vomiting, diarrhea or abdominal pain) (18%) Cough (31%) Shortness of breath (8%) | Unknown | Alpha (B.1.1.7) [E484K K417T/N S477N N501Y] | Unknown | Recovery |
| (179: post-Delta) | Females: 127 Males: 52 | Median 33 (Range 21–63) | Median: 185 (Range 8–235) | BNT162b2 (Pfizer-BioNTech): 79% mRNA-1273 (Moderna): 21% | Asymptomatic (8%) Headache (45%) Fatigue (55%) Body aches (37%) Fever (including subjective) (32%) Loss of smell/taste (28%) Chills (27%) Sore throat (44%) Rhinorrhea, nasal congestion, sneezing (52%) GI symptoms (nausea, vomiting, diarrhea or abdominal pain) (17%) Cough (53%) Shortness of breath (9%) | Unknown | Delta (B.1.617.2) [L452R T478K E484Q] | Unknown | Recovery | |||
| Vignier et al., 2021 [35] | Cohort | 25 (15) | French Guiana | Males: 15 | Median: 53.3 | >14 | BNT162b2 (Pfizer-BioNTech): 56.8% | Symptomatic: Fever, dyspnea (87%) | Hypertension, diabetes mellitus, obesity, cardiac insufficiency | Gamma (P.1) | 18–35 | Recovery |
| Tober-lau et al., 2021 [36] | Longitudinal | 20 (16) | Germany | Females: 12 Males: 4 | >65 years | 4–5 | BNT162b2 (Pfizer-BioNTech) | Asymptomatic mostly. Diarrhea, fatigue, cough or shortness of breath (31.25%) | Hypertension, Type 2 diabetes mellitus, chronic kidney disease dementia | Alpha (B.1.1.7) | Unknown | Hospitalization (31.25%) Supplemental oxygen (6.3%) Death (12.5%) |
| Servellita et al., 2022 [37] | Cohort | 1373 (125) c | USA | Females: 68 Males: 57 | Mean: 49 (Range 22–97) | Median: 73.5 (range 15–140) | BNT162b2 (Pfizer-BioNTech): 51%, mRNA-1273 (Moderna): 31% Johnson & Johnson: 10% | Asymptomatic (26%) COVID-19 pneumonia (15.4%) | Immunocompromised (23%) | Delta (B.1.617.2:31%, Alpha (B.1.1.7): 18.3%, Gamma (P.1): 15.6%, Iota (B.1.526): 11.9%, Epsilon (B.1.427/B.1.429): 6.4%, Beta (B.1.351): 3.7%, Other: 12.8% [L452R/Q, E484K/Q and/or F490S] | 23.1 | Recovery (100%) ICU (2.6%), Hospitalizations (15.4%) |
| Singer et al., 2021 [38] | Prospective cohort | 343 (31) | Israel | Females: 17 Males: 14 | Median: 58 (21–87) | >7 | BNT162b2 (Pfizer-BioNTech) | Asymptomatic (05%) | Unknown | Beta (B.1.351) | Unknown | Recovery |
| Thangaraj et al., 2022 [39] | Prospective cohort | 113 (113) | India | Females: 44 Males:66 Others:3 | Median:54 (42–64) | >14 | Covaxin: 27.4% Covishield: 70.8% Unknown: 1.8% | Symptomatic (88.5%) | Unspecified comorbidities (46%) | Delta (B.1.617.2):74.3% B.1.617.1: 0.9% AY.1: 0.9% Alpha (B.1.1.7): 0.9% Beta (B.1.351): 0.9% | <30 | Recovery |
| Olsen et al., 2021 [40] | Cohort | 12,476 (207) | USA | Females: 53% Males: 47% d | Median: 52.5 d | >14 | BNT162b2 (Pfizer-BioNTech): 87% mRNA-1273 (Moderna): 13% | Unknown | BMI > 30 (42.7%) | Alpha (B.1.1.7): 126; Gamma (P.1): 5 Epsilon (B.1.429): 3 B.1526: 1 B.1526.1:1 Eta (B.1.525): 1 non-VOC: 70 | 23.9 | Hospitalization (34.8%) |
| Singh et al., 2022 [41] | Cohort | 63 (36) | India | Females: 13 Male: 23 | Median: 37 (21–92) | Unknown | AZD1222/Covishield (SII): 15.87% BBV152/Covaxin: 84.13% | High-grade unremitting fever, shortness of breath, headache | None | Delta (B.1.617.2): 63.9% B.1.617.1: 11.1% Alpha (B.1.1.7) 2.8% | Range: 11.3–31 | Recovery |
| Tay et al., 2022 [42] | Prospective case-control | 55 (55) | Singapore | Females: 19 Males: 36 | Median 46 (IQR 36.5–59.5) | 82 (IQR 51.5–99) | BNT162b2 (Pfizer-BioNTech) | Asymptomatic (21.8%) Mild symptoms (78.2%) | Chronic venous, asthma, other chronic lung diseases, rheumatologic disease, chronic liver disease, diabetes mellitus, chronic kidney disease, malignancies, or HIV (6) | Delta (B.1.617.2): 87.3% Unknown: 7.3% Non-Delta:5.5% | Unknown | Recovery |
| Sun et al., 2021 [43] | Retrospective cohort | 604,035 (22,917) | USA | Females: 13,040 Males: 9877 | Median: 51 (IQR 34–66) | 138 (85–178) | BNT162b2 (Pfizer-BioNTech) mRNA-1273 (Moderna) | Unknown | Immunocompromised (1451). | Delta (B.1.617.2) | Unknown | Recovery (93.5%); Hospitalization: 11.5% Severe outcomes (0.65%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gopinath, S.; Ishak, A.; Dhawan, N.; Poudel, S.; Shrestha, P.S.; Singh, P.; Xie, E.; Tahir, P.; Marzaban, S.; Michel, J.; et al. Characteristics of COVID-19 Breakthrough Infections among Vaccinated Individuals and Associated Risk Factors: A Systematic Review. Trop. Med. Infect. Dis. 2022, 7, 81. https://doi.org/10.3390/tropicalmed7050081
Gopinath S, Ishak A, Dhawan N, Poudel S, Shrestha PS, Singh P, Xie E, Tahir P, Marzaban S, Michel J, et al. Characteristics of COVID-19 Breakthrough Infections among Vaccinated Individuals and Associated Risk Factors: A Systematic Review. Tropical Medicine and Infectious Disease. 2022; 7(5):81. https://doi.org/10.3390/tropicalmed7050081
Chicago/Turabian StyleGopinath, Shilpa, Angela Ishak, Naveen Dhawan, Sujan Poudel, Prakriti Singh Shrestha, Prabhjeet Singh, Emily Xie, Peggy Tahir, Sima Marzaban, Jack Michel, and et al. 2022. "Characteristics of COVID-19 Breakthrough Infections among Vaccinated Individuals and Associated Risk Factors: A Systematic Review" Tropical Medicine and Infectious Disease 7, no. 5: 81. https://doi.org/10.3390/tropicalmed7050081