
Community-Based Screening for Hepatitis B and C Infectivity Using Two Quantitative Antigens to Identify Endemic Townships

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
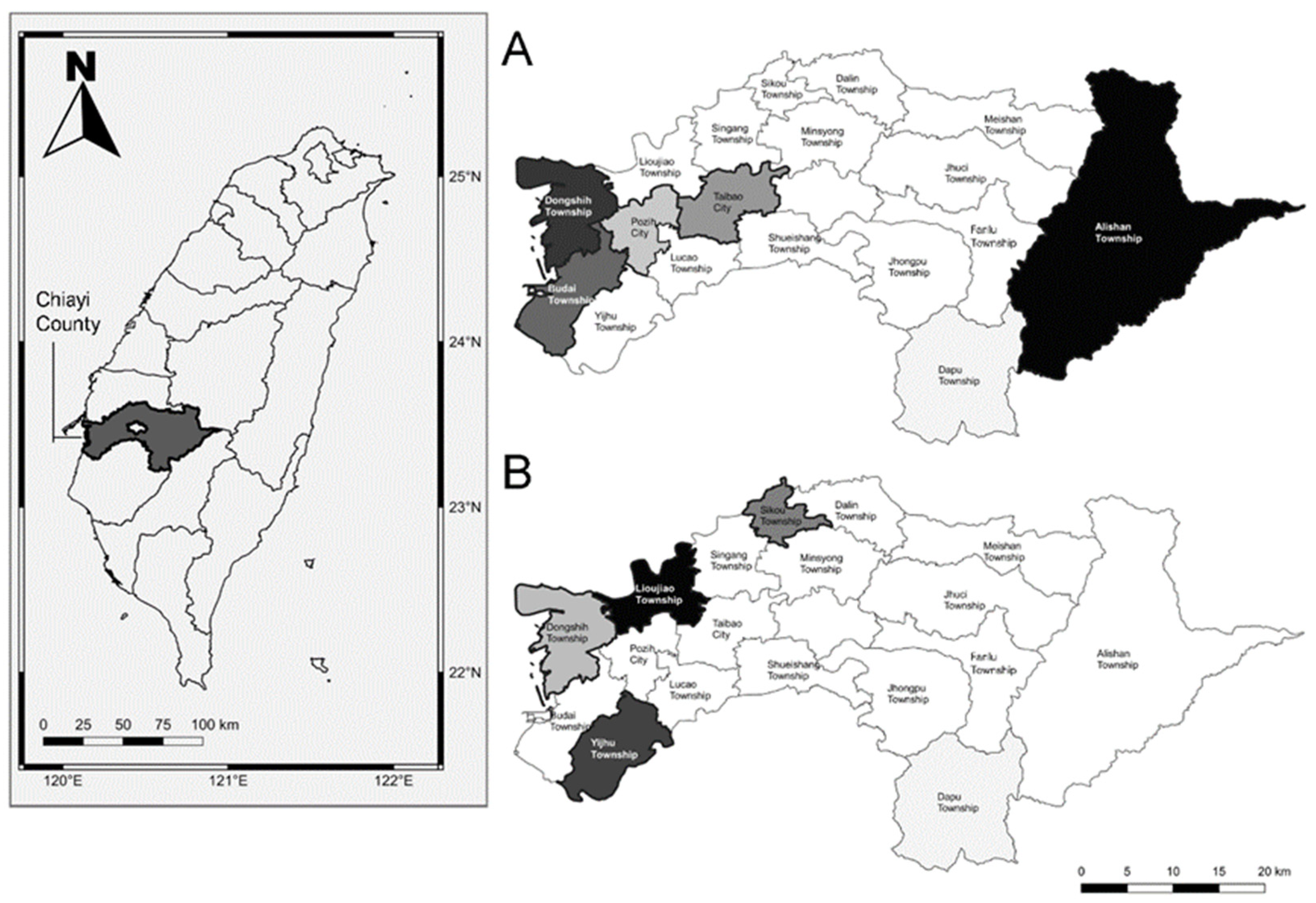
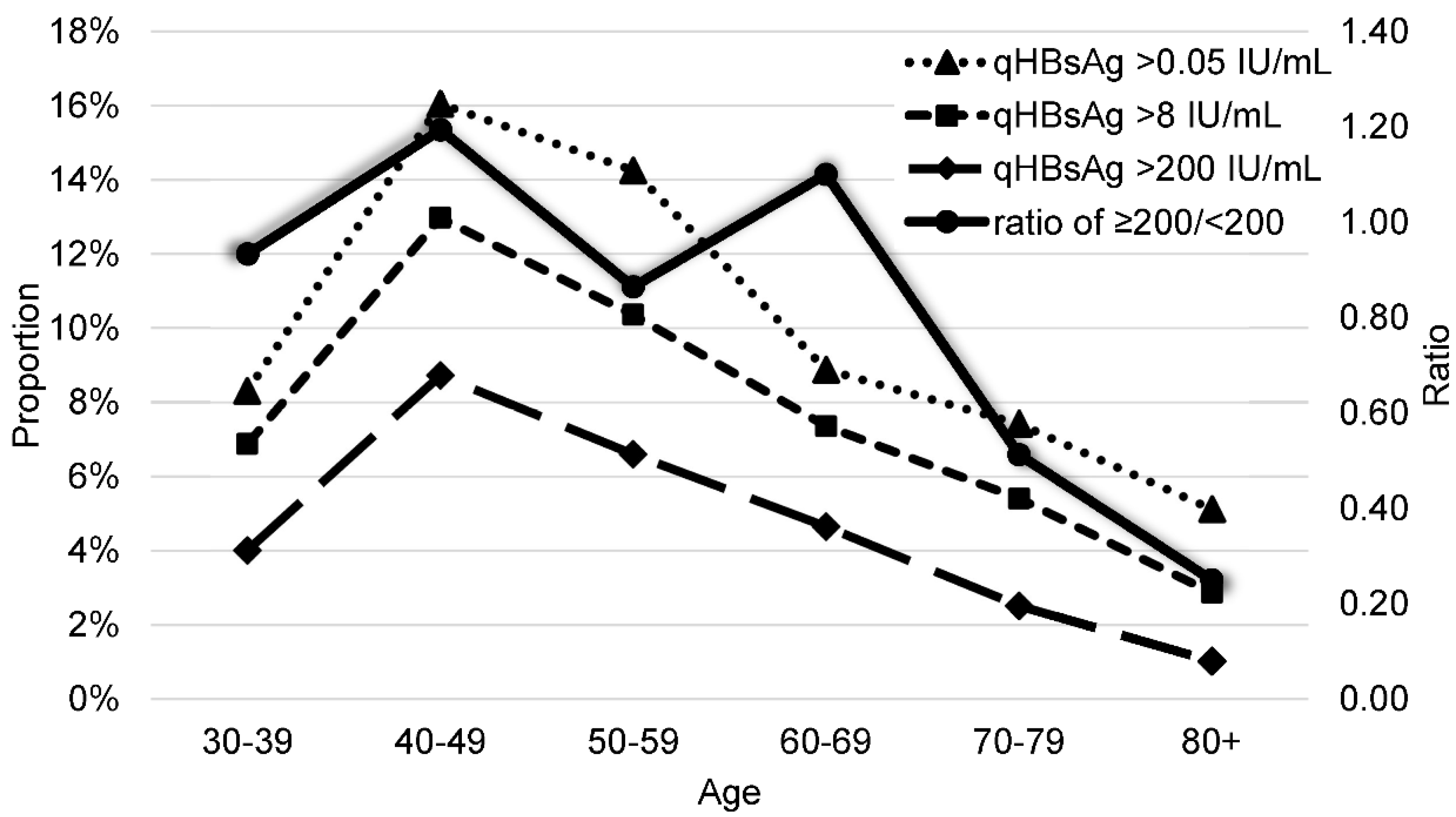
3.1. Distribution of qHBsAg in Chiayi County
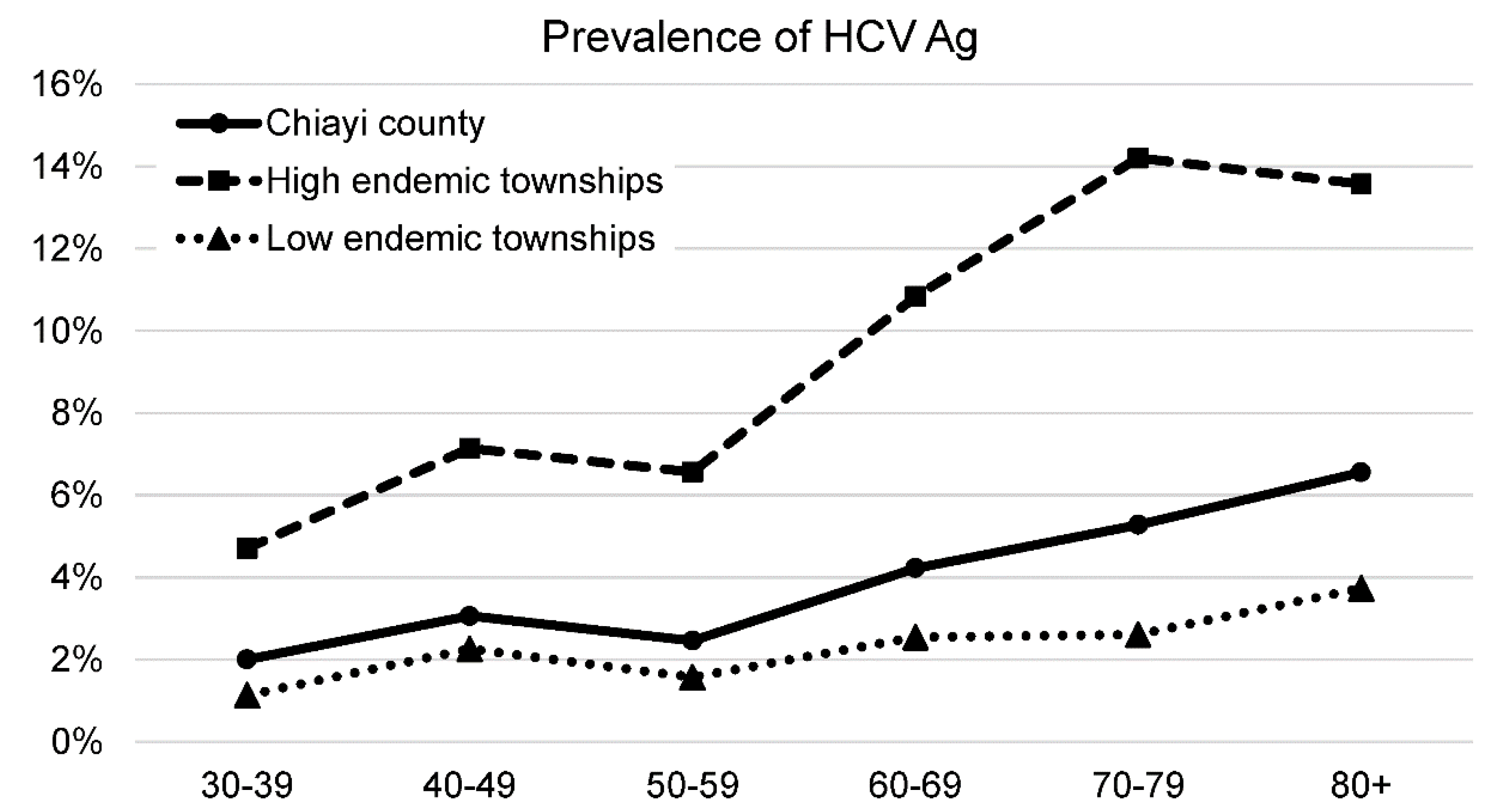
3.2. Distribution of HCV Ag in Chiayi County
3.3. Linkage to Care after HCV Ag Screening
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Oraganization Combating Hepatitis B and C to Reach Elimination by 2030. Available online: http://apps.who.int/iris/bitstream/handle/10665/206453/WHO_HIV_2016.04_eng.pdf;jsessionid=B3E035B3AC1755A1D6E0D2EC0349D78A?sequence=1 (accessed on 22 July 2021).
- Su, W.J.; Chen, S.F.; Yang, C.H.; Chuang, P.H.; Chang, H.F.; Chang, M.H. The Impact of Universal Infant Hepatitis B Immunization on Reducing the Hepatitis B Carrier Rate in Pregnant Women. J. Infect. Dis. 2019, 220, 1118–1126. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Yang, P.M.; Huang, G.T.; Lee, H.S.; Sung, J.L.; Sheu, J.C. Estimation of seroprevalence of hepatitis B virus and hepatitis C virus in Taiwan from a large-scale survey of free hepatitis screening participants. J. Formos. Med. Assoc. 2007, 106, 148–155. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health and Welfare Geographic Maps of Hepatitis C Virus Infection. Available online: https://www.mohw.gov.tw/cp-4464-52812-1.html (accessed on 22 July 2021).
- Chen, C.J.; Yang, H.I.; Su, J.; Jen, C.L.; You, S.L.; Lu, S.N.; Huang, G.T.; Iloeje, U.H. Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. J. Am. Med. Assoc. 2006, 295, 65–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.H.; Yang, H.I.; Lu, S.N.; Jen, C.L.; Yeh, S.H.; Liu, C.J.; Chen, P.J.; You, S.L.; Wang, L.Y.; Chen, W.J.; et al. Hepatitis C virus seromarkers and subsequent risk of hepatocellular carcinoma: Long-term predictors from a community-based cohort study. J. Clin. Oncol. 2010, 28, 4587–4593. [Google Scholar] [PubMed] [Green Version]
- Terrault, N.A.; Lok, A.S.F.; McMahon, B.J.; Chang, K.M.; Hwang, J.P.; Jonas, M.M.; Brown, R.S., Jr.; Bzowej, N.H.; Wong, J.B. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology 2018, 67, 1560–1599. [Google Scholar] [CrossRef]
- Pawlotsky, J.M.; Negro, F.; Aghemo, A.; Berenguer, M.; Dalgard, O.; Dusheiko, G. EASL recommendations on treatment of hepatitis C: Final update of the series. J. Hepatol. 2020, 73, 1170–1218. [Google Scholar] [CrossRef]
- Chen, C.H.; Lee, C.M.; Wang, J.H.; Tung, H.D.; Hung, C.H.; Lu, S.N. Correlation of quantitative assay of hepatitis B surface antigen and HBV DNA levels in asymptomatic hepatitis B virus carriers. Eur. J. Gastroenterol. Hepatol. 2004, 16, 1213–1218. [Google Scholar] [CrossRef]
- Kuo, Y.H.; Chang, K.C.; Wang, J.H.; Tsai, P.S.; Hung, S.F.; Hung, C.H.; Chen, C.H.; Lu, S.N. Is hepatitis C virus core antigen an adequate marker for community screening? J. Clin. Microbiol. 2012, 50, 1989–1993. [Google Scholar] [CrossRef] [Green Version]
- Chang, K.C.; Lee, C.Y.; Chang, T.S.; Hung, C.H.; Chen, W.M.; Chen, M.Y.; Huang, T.J.; Chiu, W.N.; Hu, J.H.; Lin, Y.C.; et al. Usefulness of quantitative hepatitis B surface antigen testing in hepatitis B community-based screening. J. Formos. Med. Assoc. 2021, 120, 847–853. [Google Scholar] [CrossRef]
- Liu, J.; Yang, H.I.; Lee, M.H.; Lu, S.N.; Jen, C.L.; Batrla-Utermann, R.; Wang, L.Y.; You, S.L.; Hsiao, C.K.; Chen, P.J.; et al. Spontaneous seroclearance of hepatitis B seromarkers and subsequent risk of hepatocellular carcinoma. Gut 2014, 63, 1648–1657. [Google Scholar] [CrossRef]
- Kuo, Y.H.; Chen, P.F.; Wang, J.H.; Chang, K.C.; Kee, K.M.; Tsai, M.C.; Lin, C.Y.; Lin, S.C.; Tsai, L.S.; Chen, S.C.; et al. Comparison Stratagems of Post-Screening Management of Anti-HCV-Positive Community Residents: Simple Notification, Active Referral, or Accessible Medical Care. PLoS ONE 2015, 10, e0126031. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.H.; Chen, C.H.; Chang, C.M.; Feng, W.C.; Lee, C.Y.; Lu, S.N. Hepatitis C virus core antigen is cost-effective in community-based screening of active hepatitis C infection in Taiwan. J. Formos. Med. Assoc. 2020, 119 Pt 3, 504–508. [Google Scholar] [CrossRef]
- Chen, W.M.; Lee, C.Y.; Hsu, N.T.; Huang, W.C.; Chen, M.Y.; Huang, T.J.; Lu, S.N. Feasibility of anti-HCV reflex HCV Ag screening strategy in an HCV endemic community. J. Formos. Med. Assoc. 2021, 120, 1237–1241. [Google Scholar] [CrossRef]
- Ministry of Health and Welfare Geographic Distribution of Cancer in Taiwan. Available online: https://dep.mohw.gov.tw/dos/cp-1861-41759-113.html (accessed on 23 July 2021).
- Lu, S.N.; Su, W.W.; Yang, S.S.; Chang, T.T.; Cheng, K.S.; Wu, J.C.; Lin, H.H.; Wu, S.S.; Lee, C.M.; Changchien, C.S.; et al. Secular trends and geographic variations of hepatitis B virus and hepatitis C virus-associated hepatocellular carcinoma in Taiwan. Int. J. Cancer 2006, 119, 1946–1952. [Google Scholar] [CrossRef]
- Ginzberg, D.; Wong, R.J.; Gish, R. Global HBV burden: Guesstimates and facts. Hepatol. Int. 2018, 12, 315–329. [Google Scholar] [CrossRef]
- Cuadros, D.F.; Branscum, A.J.; Miller, F.D.; Abu-Raddad, L.J. Spatial epidemiology of hepatitis C virus infection in Egypt: Analyses and implications. Hepatology 2014, 60, 1150–1159. [Google Scholar] [CrossRef] [Green Version]
- Tsai, M.C.; Kee, K.M.; Chen, Y.D.; Lin, L.C.; Tsai, L.S.; Chen, H.H.; Lu, S.N. Excess mortality of hepatocellular carcinoma and morbidity of liver cirrhosis and hepatitis in HCV-endemic areas in an HBV-endemic country: Geographic variations among 502 villages in southern Taiwan. J. Gastroenterol. Hepatol. 2007, 22, 92–98. [Google Scholar] [CrossRef]
- Sun, C.A.; Chen, H.C.; Lu, S.N.; Chen, C.J.; Lu, C.F.; You, S.L.; Lin, S.H. Persistent hyperendemicity of hepatitis C virus infection in Taiwan: The important role of iatrogenic risk factors. J. Med. Virol. 2001, 65, 30–34. [Google Scholar] [CrossRef]
- Calvaruso, V.; Bronte, F.; Ferraro, D.; Reina, G.; Conte, E.; Rini, F.; Magro, B.; Petta, S.; Di Marco, V.; Craxì, A. Point-of-care HCV RNA testing in the setting of DAA therapy: HCV-FiS (HEpatitis C Virus Fingerstick Study). Liver Int. 2019, 39, 2240–2243. [Google Scholar] [CrossRef]
- Bregenzer, A.; Warmann, N.; Ottiger, C.; Fux, C.A. Rapid point-of-care HCV RNA quantification in capillary whole blood for diagnosing chronic HCV infection, monitoring treatment and detecting reinfection. Swiss Med. Wkly. 2019, 149, w20137. [Google Scholar] [CrossRef]
- Pérez-García, A.; Aguinaga, A.; Navascués, A.; Castilla, J.; Ezpeleta, C. Hepatitis C core antigen: Diagnosis and monitoring of patients infected with hepatitis C virus. Int. J. Infect. Dis. 2019, 89, 131–136. [Google Scholar] [CrossRef] [Green Version]
- Van Tilborg, M.; Al Marzooqi, S.H.; Wong, W.W.L.; Maan, R.; Vermehren, J.; Maasoumy, B.; Mazzulli, T.; Bolotin, S.; Garber, G.; Guerra, F.; et al. HCV core antigen as an alternative to HCV RNA testing in the era of direct-acting antivirals: Retrospective screening and diagnostic cohort studies. Lancet Gastroenterol. Hepatol. 2018, 3, 856–864. [Google Scholar] [CrossRef]
- Chang, C.; Hung, C.H.; Wang, J.H.; Lu, S.N. Hepatitis C core antigen highly correlated to HCV RNA. Kaohsiung J. Med. Sci. 2018, 34, 684–688. [Google Scholar] [CrossRef]
- Lee, M.H.; Yang, H.I.; Liu, J.; Batrla-Utermann, R.; Jen, C.L.; Iloeje, U.H.; Lu, S.N.; You, S.L.; Wang, L.Y.; Chen, C.J. Prediction models of long-term cirrhosis and hepatocellular carcinoma risk in chronic hepatitis B patients: Risk scores integrating host and virus profiles. Hepatology 2013, 58, 546–554. [Google Scholar] [CrossRef]
- Cornberg, M.; Wong, V.W.; Locarnini, S.; Brunetto, M.; Janssen, H.L.A.; Chan, H.L. The role of quantitative hepatitis B surface antigen revisited. J. Hepatol. 2017, 66, 398–411. [Google Scholar] [CrossRef] [Green Version]
- Chiu, S.M.; Kuo, Y.H.; Wang, J.H.; Hung, C.H.; Hu, T.H.; Lu, S.N.; Chen, C.H. Associations of HBV Genotype B vs C Infection With Relapse After Cessation of Entecavir or Tenofovir Therapy. Clin. Gastroenterol. Hepatol. 2020, 18, 2989–2997.e3. [Google Scholar] [CrossRef]
- Chen, J.D.; Yang, H.I.; Iloeje, U.H.; You, S.L.; Lu, S.N.; Wang, L.Y.; Su, J.; Sun, C.A.; Liaw, Y.F.; Chen, C.J. Carriers of inactive hepatitis B virus are still at risk for hepatocellular carcinoma and liver-related death. Gastroenterology 2010, 138, 1747–1754. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| qHBsAg (n/%) | ||||
|---|---|---|---|---|
| Groups | N | >0.05 IU/mL | >8 IU/mL | >200 IU/mL |
| Total | 4010 | 396 (9.9%) | 303 (7.6%) | 182 (4.5%) |
| Sex | ||||
| Male | 1630 | 155 (9.5%) | 115 (7.1%) | 64 (3.9%) |
| Female | 2380 | 241 (10.1%) | 188 (7.9%) | 118 (5.0%) |
| Age (years) | ||||
| 30–39 | 349 | 29 (8.3%) | 24 (6.9%) | 14 (4.0%) |
| 40–49 | 424 | 68 (16.0%) | 55 (13.0%) | 37 (8.7%) |
| 50–59 | 772 | 110 (14.2%) | 80 (10.4%) | 51 (6.6%) |
| 60–69 | 1182 | 105 (8.9%) | 87 (7.4%) | 55 (4.7%) |
| 70–79 | 795 | 59 (7.4%) | 43 (5.4%) | 20 (2.5%) |
| 80+ | 488 | 25 (5.1%) | 14 (2.9%) | 5 (1.0%) |
| Township | ||||
| High prevalence (>17%) | ||||
| Alishan Township | 114 | 24 (21.1%) | 19 (16.7%) | 10 (8.8%) |
| Dongshih Township | 172 | 30 (17.4%) | 24 (14.0%) | 12 (7.0%) |
| Budai Township | 292 | 50 (17.1%) | 40 (13.7%) | 24 (8.2%) |
| Medium prevalence (10~13%) | ||||
| Taibao City | 198 | 25 (12.6%) | 22 (11.1%) | 16 (8.1%) |
| Pozi City | 285 | 29 (10.2%) | 22 (7.7%) | 18 (6.3%) |
| Low prevalence (<10%) | ||||
| Yijhu Township | 257 | 25 (9.7%) | 20 (7.8%) | 11 (4.3%) |
| Fanlu Township | 226 | 21 (9.3%) | 17 (7.5%) | 8 (3.5%) |
| Jhuci Township | 76 | 7 (9.2%) | 3 (3.9%) | 2 (2.6%) |
| Jhongpu Township | 282 | 25 (8.9%) | 18 (6.4%) | 10 (3.5%) |
| Shueishang Township | 316 | 27 (8.5%) | 19 (6.0%) | 11 (3.5%) |
| Singang Township | 324 | 27 (8.3%) | 20 (6.2%) | 14 (4.3%) |
| Meishan Township | 249 | 20 (8.0%) | 18 (7.2%) | 12 (4.8%) |
| Sikou Township | 152 | 12 (7.9%) | 9 (5.9%) | 7 (4.6%) |
| Lucao Township | 263 | 20 (7.6%) | 14 (5.3%) | 7 (2.7%) |
| Dalin Township | 197 | 14 (7.1%) | 10 (5.1%) | 6 (3.0%) |
| Lioujiao Township | 274 | 19 (6.9%) | 17 (6.2%) | 6 (2.2%) |
| Minsyong Township | 333 | 21 (6.3%) | 11 (3.3%) | 8 (2.4%) |
| Groups | N | HCV Ag (+) | log10 HCV Ag 1 | DAA Therapy |
|---|---|---|---|---|
| Total | 4010 | 163 (4.1%) | 3.32 ± 0.90 | 114/163 (69.9%) |
| Sex | ||||
| Male | 1630 | 69 (4.2%) | 3.25 ± 0.92 | 52/69 (75.4%) |
| Female | 2380 | 94 (3.9%) | 3.36 ± 0.90 | 62/94 (66.0%) |
| Age (years) | ||||
| 30–39 | 349 | 7 (2.0%) | 3.14 ± 1.02 | 6/7 (85.7%) |
| 40–49 | 424 | 13 (3.1%) | 2.64 ± 1.33 | 6/13 (46.2%) |
| 50–59 | 772 | 19 (2.5%) | 3.28 ± 0.91 | 17/19 (89.5%) |
| 60–69 | 1182 | 50 (4.2%) | 3.52 ± 0.81 | 39/50 (78.0%) |
| 70–79 | 795 | 42 (5.3%) | 3.24 ± 0.92 | 29/42 (69.0%) |
| 80+ | 488 | 32 (6.6%) | 3.43 ± 0.67 | 17/32 (53.1%) |
| Township | ||||
| High prevalence (>11%) | ||||
| Lioujiao Township | 274 | 40 (14.6%) | 3.65 ± 0.78 | 26/40 (65.0%) |
| Yijhu Township | 257 | 29 (11.3%) | 3.40 ± 0.81 | 23/29 (79.3%) |
| Medium prevalence (5~8%) | ||||
| Sikou Township | 152 | 11 (7.2%) | 3.41 ± 0.93 | 7/11 (63.6%) |
| Dongshih Township | 172 | 9 (5.2%) | 3.26 ± 0.84 | 8/9 (88.9%) |
| Low prevalence (<4%) | ||||
| Jhuci Township | 76 | 3 (3.9%) | 3.81 ± 0.25 | 3/3 (100.0%) |
| Singang Township | 324 | 12 (3.7%) | 3.35 ± 0.81 | 7/12 (58.3%) |
| Jhongpu Township | 282 | 9 (3.2%) | 3.31 ± 0.99 | 9/9 (100.0%) |
| Lucao Township | 263 | 8 (3.0%) | 2.75 ± 1.06 | 5/8 (62.5%) |
| Taibao City | 198 | 6 (3.0%) | 2.64 ± 1.10 | 2/6 (33.3%) |
| Fanlu Township | 226 | 6 (2.7%) | 3.35 ± 1.17 | 4/6 (66.7%) |
| Alishan Township | 114 | 3 (2.6%) | 2.77 ± 1.24 | 3/3 (100.0%) |
| Dalin Township | 197 | 5 (2.5%) | 2.87 ± 0.36 | 3/5 (60.0%) |
| Minsyong Township | 333 | 8 (2.4%) | 2.45 ± 1.18 | 2/8 (25.0%) |
| Pozi City | 285 | 6 (2.1%) | 3.44 ± 1.01 | 6/6 (100.0%) |
| Shueishang Township | 316 | 5 (1.6%) | 3.22 ± 0.84 | 3/5 (60.0%) |
| Meishan Township | 249 | 2 (0.8%) | 3.52 ± 0.24 | 2/2 (100.0%) |
| Budai Township | 292 | 1 (0.3%) | 3.35 | 1/1 (100.0%) |
| Total (n = 151) | DAA Treatment (n = 114, 75.4%) | Without DAA Treatment (n = 37, 24.5%) | p-Value | |
|---|---|---|---|---|
| Age | 67.6 ± 13.4 | 66.1 ± 12.7 | 72.4 ± 14.5 | 0.012 |
| <75 | 97 | 83 (85.6%) | 14 (14.4%) | <0.001 |
| ≥75 | 54 | 31 (57.4%) | 23 (42.6%) | |
| Sex | 0.089 | |||
| Male | 63 | 52 (82.5%) | 11 (17.5%) | |
| Female | 88 | 62 (70.5%) | 26 (29.5%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, W.-C.; Lin, Y.-C.; Chen, P.-J.; Hsu, N.-T.; Tu, C.-L.; Chang, T.-S.; Hung, C.-H.; Kee, K.-M.; Chao, W.-H.; Lu, S.-N. Community-Based Screening for Hepatitis B and C Infectivity Using Two Quantitative Antigens to Identify Endemic Townships. Viruses 2022, 14, 304. https://doi.org/10.3390/v14020304
Huang W-C, Lin Y-C, Chen P-J, Hsu N-T, Tu C-L, Chang T-S, Hung C-H, Kee K-M, Chao W-H, Lu S-N. Community-Based Screening for Hepatitis B and C Infectivity Using Two Quantitative Antigens to Identify Endemic Townships. Viruses. 2022; 14(2):304. https://doi.org/10.3390/v14020304
Chicago/Turabian StyleHuang, Wei-Cheng, Yu-Chen Lin, Po-Ju Chen, Nien-Tzu Hsu, Chia-Ling Tu, Te-Sheng Chang, Chao-Hung Hung, Kwong-Ming Kee, Wen-Hua Chao, and Sheng-Nan Lu. 2022. "Community-Based Screening for Hepatitis B and C Infectivity Using Two Quantitative Antigens to Identify Endemic Townships" Viruses 14, no. 2: 304. https://doi.org/10.3390/v14020304