
Consequences of In Utero Zika Virus Exposure and Adverse Pregnancy and Early Childhood Outcomes: A Prospective Cohort Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Criteria for Inclusion in Analysis
2.2. Cohort Follow-Up
2.3. Adverse Early Childhood Outcomes
- Abnormal auditory examination which included otoacoustic emissions or automated auditory evoked potential assessments;
- Abnormal ophthalmologic examination, which included RetCam wide-field retinal imaging (Shuttle, Clarity Medical Systems, Pleasanton, USA) for fundus imaging and abnormalities in vitreous, choroid, retina and optic disc; or visual impairment documented by visual screening test;
- Clinician-documented seizures, excluding febrile seizures;
- Body tone abnormalities, hypertonia or hypotonia, suspicion or diagnosis of cerebral palsy;
- Musculoskeletal or motor abnormalities, dyskinesia or dystonia, documented by the clinician;
- Swallowing abnormalities, documented by instrumented or non-instrumented evaluation;
- Post-natal onset microcephaly, defined as the two most recent head circumference measurements < 3rd percentile for age and sex based on the World Health Organization’s Child Growth Standards, or by a downwards trajectory of head circumference percentiles, with the most recent measurement < 3rd percentile;
- Possible neurodevelopmental delays, through administration of three pediatric neurodevelopment evaluation tools administered to a parent/legal guardian at the time of the 24-month pediatric consultation [13]: a 30-item parent-reported screening test, Ages and Stages Questionnaire-III (ASQ) [14], previously validated in France [15], to identify toddlers at risk for developmental delay; a 23-item parent-reported screening test, Modified Checklist for Autism on Toddlers (M-CHAT), to identify toddlers at risk for behavior disorder [16]; the French MacArthur-Bates Communicative Development Inventories (Inventaires français du développement communicative—IFDC) to assess French language acquisition [17].
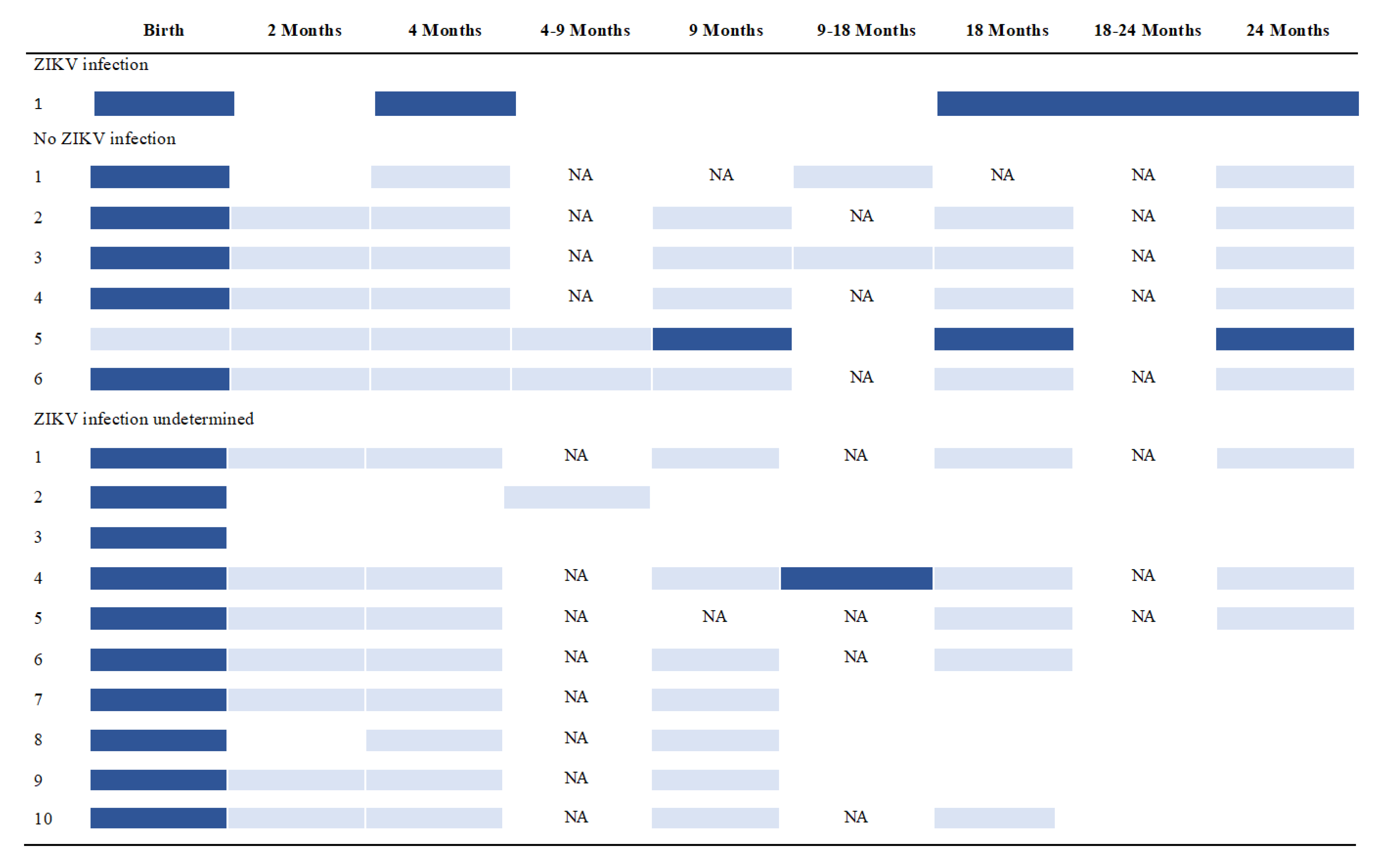
2.4. ZIKV Infection Status
2.5. Statistical Analysis
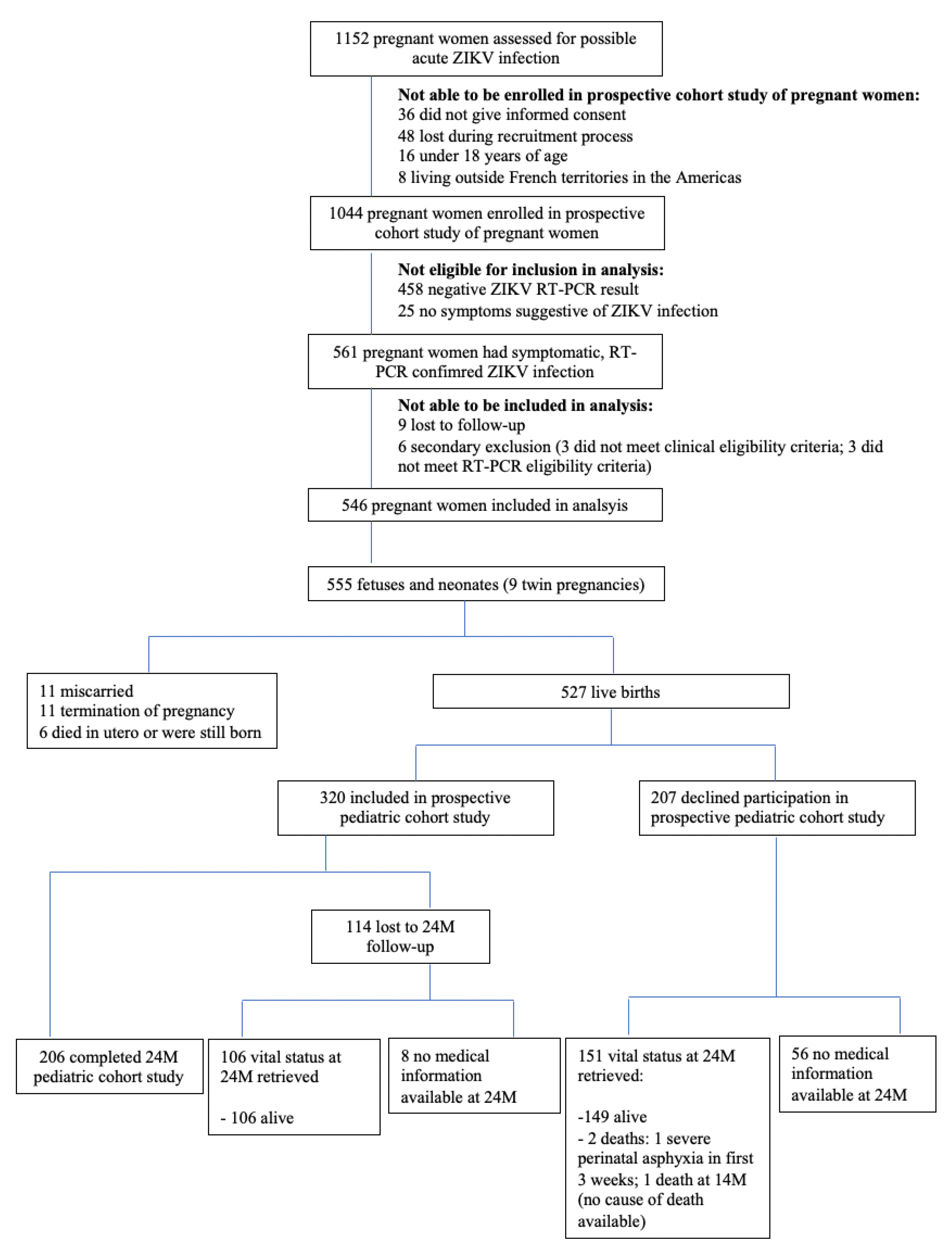
3. Results
3.1. Adverse Pregnancy Outcomes
3.2. ZIKV Infection Status
3.3. Adverse Early Childhood Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moore, C.A.; Staples, J.E.; Dobyns, W.B.; Pessoa, A.; Ventura, C.V.; Da Fonseca, E.B.; Ribeiro, E.M.; Ventura, L.O.; Neto, N.N.; Arena, J.F.; et al. Characterizing the Pattern of Anomalies in Congenital Zika Syndrome for Pediatric Clinicians. JAMA Pediatr. 2017, 171, 288–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wheeler, A.C.; Toth, D.; Ridenour, T.; Nóbrega, L.L.; Firmino, R.B.; Da Silva, C.M.; Carvalho, P.; Marques, D.; Okoniewski, K.; Ventura, L.O.; et al. Developmental Outcomes Among Young Children With Congenital Zika Syndrome in Brazil. JAMA Netw. Open 2020, 3, e204096. [Google Scholar] [CrossRef] [PubMed]
- Satterfield-Nash, A.; Kotzky, K.; Allen, J.; Bertolli, J.; Moore, C.A.; Pereira, I.O.; Pessoa, A.; Melo, F.; Santelli, A.C.F.E.S.; Boyle, C.A.; et al. Health and Development at Age 19–24 Months of 19 Children Who Were Born with Microcephaly and Laboratory Evidence of Congenital Zika Virus Infection During the 2015 Zika Virus Outbreak—Brazil, 2017. MMWR. Morb. Mortal. Wkly. Rep. 2017, 66, 1347–1351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frota, L.M.D.C.P.; Sampaio, R.F.; Miranda, J.L.; Brasil, R.M.C.; Gontijo, A.P.B.; de Melo Mambrini, J.V.; de Brito Brandão, M.; Mancini, M.C. Children with congenital Zika syndrome: Symptoms, comorbidities and gross motor development at 24 months of age. Heliyon 2020, 6, e04130. [Google Scholar] [CrossRef] [PubMed]
- Pessoa, A.; van der Linden, V.; Yeargin-Allsopp, M.; Carvalho, M.D.C.G.; Ribeiro, E.M.; Van Naarden Braun, K.; Durkin, M.S.; Pastula, D.M.; Moore, J.T.; Moore, C.A. Motor abnormalities and epilepsy in infants and children with evidence of congenital Zika virus infection. Pediatrics 2018, 141 (Suppl. S2), S167–S179. [Google Scholar] [CrossRef] [Green Version]
- Pereira, H.V.F.S.; Dos Santos, S.P.; Amâncio, A.P.R.L.; De Oliveira-Szejnfeld, P.S.; Flor, E.O.; de Sales Tavares, J.; Ferreira, R.V.B.; Tovar-Moll, F.; De Amorim, M.M.R.; Melo, A. Neurological outcomes of congenital Zika syndrome in toddlers and preschoolers: A case series. Lancet Child Adolesc. Health 2020, 4, 378–387. [Google Scholar] [CrossRef]
- Bertolli, J.; Attell, J.E.; Rose, C.; Moore, C.A.; Melo, F.; Staples, J.E.; Kotzky, K.; Krishna, N.; Satterfield-Nash, A.; Pereira, I.O.; et al. Functional Outcomes among a Cohort of Children in Northeastern Brazil Meeting Criteria for Follow-Up of Congenital Zika Virus Infection. Am. J. Trop. Med. Hyg. 2020, 102, 955–963. [Google Scholar] [CrossRef] [Green Version]
- Rice, M.E.; Galang, R.R.; Roth, N.M.; Ellington, S.R.; Moore, C.A.; Valencia-Prado, M.; Ellis, E.M.; Tufa, A.J.; Taulung, L.A.; Alfred, J.M.; et al. Vital signs: Zika-associated birth defects and neurodevelopmental abnormalities possibly associated with congenital Zika virus infection—US territories and freely associated states, 2018. Morb. Mortal. Wkly. Rep. 2018, 67, 858. [Google Scholar]
- Alves, L.V.; E Paredes, C.; Silva, G.C.; Mello, J.G.; Alves, J.G. Neurodevelopment of 24 children born in Brazil with congenital Zika syndrome in 2015: A case series study. BMJ Open 2018, 8, e021304. [Google Scholar] [CrossRef] [Green Version]
- Paixao, E.S.; Cardim, L.L.; Costa, M.C.; Brickley, E.B.; de Carvalho-Sauer, R.C.; Carmo, E.H.; Andrade, R.F.; Rodrigues, M.S.; Veiga, R.V.; Costa, L.C.; et al. Mortality from Congenital Zika Syndrome—Nationwide Cohort Study in Brazil. N. Engl. J. Med. 2022, 386, 757–767. [Google Scholar] [CrossRef]
- Hcini, N.; Kugbe, Y.; Rafalimanana ZH, L.; Lambert, V.; Mathieu, M.; Carles, G.; Baud, D.; Panchaud, A.; Pomar, L. Association between confirmed congenital Zika infection at birth and outcomes up to 3 years of life. Nat. Commun. 2021, 12, 3270. [Google Scholar] [CrossRef] [PubMed]
- Hoen, B.; Schaub, B.; Funk, A.L.; Ardillon, V.; Boullard, M.; Cabié, A.; Callier, C.; Carles, G.; Cassadou, S.; Césaire, R.; et al. Pregnancy outcomes after ZIKV infection in French territories in the Americas. N. Engl. J. Med. 2018, 378, 985–994. [Google Scholar] [CrossRef] [PubMed]
- Grant, R.; Fléchelles, O.; Tressières, B.; Dialo, M.; Elenga, N.; Mediamolle, N.; Mallard, A.; Hebert, J.-C.; Lachaume, N.; Couchy, E.; et al. In utero Zika virus exposure and neurodevelopment at 24 months in toddlers normocephalic at birth: A cohort study. BMC Med. 2021, 19, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Squires, J.; Bricker, D.D.; Twombly, E. (ASQ®-3): A Parent-Completed Child Monitoring System. In Ages & Stages Questionnaires®, 3rd ed.; Paul H. Brookes Publishing Co., Inc.: Baltimore, MD, USA, 2009; pp. 182–257. [Google Scholar]
- Flamant, C.; Branger, B.; Tich, S.N.T.; de La Rochebrochard, E.; Savagner, C.; Berlie, I.; Rozé, J.-C. Parent-Completed Developmental Screening in Premature Children: A Valid Tool for Follow-Up Programs. PLoS ONE 2011, 6, e20004. [Google Scholar] [CrossRef]
- Robins, D.L.; Fein, D.; Barton, M.L.; Green, J.A. The Modified Checklist for Autism in Toddlers: An Initial Study Investigating the Early Detection of Autism and Pervasive Developmental Disorders. J. Autism Dev. Disord. 2001, 31, 131–144. [Google Scholar] [CrossRef]
- Fenson, L.; Marchman, V.A.; Thal, D.J.; Dale, P.S.; Reznick, J.S.; Bates, E. Macarthur-Bates Communicative Development Inventories, 2nd ed.; Paul H. Brookes: Baltimore, MD, USA, 2007. [Google Scholar]
- Flamand, C.; Fritzell, C.; Matheus, S.; Dueymes, M.; Carles, G.; Favre, A.; Enfissi, A.; Adde, A.; Demar, M.; Kazanji, M.; et al. The proportion of asymptomatic infections and spectrum of disease among pregnant women infected by Zika virus: Systematic monitoring in French Guiana, 2016. Eurosurveillance 2017, 22, 17–00102. [Google Scholar] [CrossRef] [Green Version]
- De Alencar Ximenes, R.A.; de Barros Miranda-Filho, D.; Brickley, E.B.; de Araújo, T.V.B.; Montarroyos, U.R.; Abtibol-Bernardino, M.R.; Mussi-Pinhata, M.M.; Duarte, G.; Coutinho, C.M.; de Moura Negrini, C.F.B.; et al. Risk of adverse outcomes in offspring with RT-PCR confirmed prenatal Zika virus exposure: An individual participant data meta-analysis of 13 cohorts in the Zika Brazilian Cohorts Consortium. Lancet Reg. Health-Am. 2022, 100395. [Google Scholar] [CrossRef]
- Brasil, P.; Vasconcelos, Z.; Kerin, T.; Gabaglia, C.R.; Ribeiro, I.P.; Bonaldo, M.C.; Damasceno, L.; Pone, M.V.; Pone, S.; Zin, A.; et al. Zika virus vertical transmission in children with confirmed antenatal exposure. Nat. Commun. 2020, 11, 1–8. [Google Scholar] [CrossRef]
- Lopes Moreira, M.E.; Nielsen-Saines, K.; Brasil, P.; Kerin, T.; Damasceno, L.; Pone, M.; Carvalho, L.M.A.; Pone, S.M.; Vasconcelos, Z.; Ribeiro, I.P.; et al. Neurodevelopment in infants exposed to Zika virus in utero. N. Engl. J. Med. 2018, 379, 2377–2379. [Google Scholar] [CrossRef]
- Conners, E.E.; Lee, E.H.; Thompson, C.N.; McGibbon, E.; Rakeman, J.L.; Iwamoto, M.; Cooper, H.; Vora, N.M.; Limberger, R.J.; Fine, A.D.; et al. Zika Virus Infection Among Pregnant Women and Their Neonates in New York City, January 2016–June 2017. Obstet. Gynecol. 2018, 132, 487–495. [Google Scholar] [CrossRef]
- Pomar, L.; Vouga, M.; Lambert, V.; Pomar, C.; Hcini, N.; Jolivet, A.; Benoist, G.; Rousset, D.; Matheus, S.; Malinger, G.; et al. Maternal-fetal transmission and adverse perinatal outcomes in pregnant women infected with Zika virus: Prospective cohort study in French Guiana. BMJ 2018, 363, k4431. [Google Scholar] [CrossRef] [PubMed]
- Halstead, S.B. Observations related to pathogensis of dengue hemorrhagic fever. VI. Hypotheses and discussion. Yale J. Biol. Med. 1970, 42, 350–362. [Google Scholar] [PubMed]
- Katzelnick, L.C.; Gresh, L.; Halloran, M.E.; Mercado, J.C.; Kuan, G.; Gordon, A.; Balmaseda, A.; Harris, E. Antibody-dependent enhancement of severe dengue disease in humans. Science 2017, 358, 929–932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordon, A.; Gresh, L.; Ojeda, S.; Katzelnick, L.C.; Sanchez, N.; Mercado, J.C.; Chowell, G.; Lopez, B.; Elizondo, D.; Coloma, J.; et al. Prior dengue virus infection and risk of Zika: A pediatric cohort in Nicaragua. PLOS Med. 2019, 16, e1002726. [Google Scholar] [CrossRef]
- Pedroso, C.; Fischer, C.; Feldmann, M.; Sarno, M.; Luz, E.; Moreira-Soto, A.; Al., C.P.E.; Netto, E.M.; Brites, C.; Kümmerer, B.M.; et al. Cross-Protection of Dengue Virus Infection against Congenital Zika Syndrome, Northeastern Brazil. Emerg. Infect. Dis. 2019, 25, 1485–1493. [Google Scholar] [CrossRef] [Green Version]
- Castanha, P.M.S.; Nascimento, E.J.M.; Cynthia, B.; Cordeiro, M.T.; De Carvalho, O.V.; De Mendonça, L.R.; Azevedo, E.A.N.; França, R.F.O.; Rafael, D.; Marques, E.T.A. Dengue virus (DENV)-specific antibodies enhance Brazilian Zika virus (ZIKV) infection. J. Infect. Dis. 2017, 215, 781–785. [Google Scholar] [CrossRef] [Green Version]
- Bardina, S.V.; Bunduc, P.; Tripathi, S.; Duehr, J.; Frere, J.J.; Brown, J.A.; Nachbagauer, R.; Foster, G.A.; Krysztof, D.; Tortorella, D.; et al. Enhancement of Zika virus pathogenesis by preexisting antiflavivirus immunity. Science 2017, 356, 175–180. [Google Scholar] [CrossRef] [Green Version]
- Terzian AC, B.; Schanoski, A.S.; Mota MT, D.O.; Da Silva, R.A.; Estofolete, C.F.; Colombo, T.E.; Rahal, P.; Hanley, K.A.; Vasilakis, N.; Kalil, J.; et al. Viral load and cytokine response profile does not support antibody-dependent enhancement in dengue-primed Zika virus–infected patients. Clin. Infect. Dis. 2017, 65, 1260–1265. [Google Scholar] [CrossRef] [Green Version]
- Langerak, T.; Mumtaz, N.; Tolk, V.I.; Van Gorp, E.C.M.; Martina, B.E.; Rockx, B.; Koopmans, M.P.G. The possible role of cross-reactive dengue virus antibodies in Zika virus pathogenesis. PLOS Pathog. 2019, 15, e1007640. [Google Scholar] [CrossRef]
- L′Azou, M.; Jean-Marie, J.; Bessaud, M.; Cabié, A.; Césaire, R.; de Lamballerie, X.; Courbil, R.; Richard, P. Dengue Seroprevalence in the French West Indies: A Prospective Study in Adult Blood Donors. Am. J. Trop. Med. Hyg. 2015, 92, 1137–1140. [Google Scholar] [CrossRef] [Green Version]
- Bjarnadóttir, E.; Stokholm, J.; Chawes, B.; Thorsen, J.; Mora-Jensen, A.R.C.; Deleuran, M.; Bønnelykke, K.; Lauritzen, L.; Bisgaard, H. Determinants of neurodevelopment in early childhood–results from the Copenhagen prospective studies on asthma in childhood (COPSAC 2010) mother–child cohort. Acta Paediatr. 2019, 108, 1632–1641. [Google Scholar] [CrossRef] [PubMed]
- Koutra, K.; Chatzi, L.; Roumeliotaki, T.; Vassilaki, M.; Giannakopoulou, E.; Batsos, C.; Koutis, A.; Kogevinas, M. Socio-demographic determinants of infant neurodevelopment at 18 months of age: Mother–Child Cohort (Rhea Study) in Crete, Greece. Infant Behav. Dev. 2012, 35, 48–59. [Google Scholar] [CrossRef] [PubMed]
- Funk, A.L.; Hoen, B.; Vingdassalom, I.; Ryan, C.; Kadhel, P.; Schepers, K.; Gaete, S.; Tressières, B.; Fontanet, A. Reassessment of the risk of birth defects due to Zika virus in Guadeloupe, 2016. PLOS Neglected Trop. Dis. 2021, 15, e0009048. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| 1A. Maternal Characteristics | n = 546 |
|---|---|
| Age at time of pregnancy (years) | |
| Mean ± SD | 29.7 ± 6.2 |
| Interquartile range | 25.0–34.3 |
| Occupation—n (%) | |
| Student | 23 (4.2) |
| Self-employed/ business owner/ farmer | 31 (5.7) |
| Executive/ highly skilled worker | 55 (10.1) |
| Intermittent profession | 56 (10.3) |
| Salaried employee | 181 (33.2) |
| Not employed | 188 (34.4) |
| Unknown or declined to respond | 12 (2.2) |
| Educational attainment of mother—n (%) | |
| Primary | 18 (3.3) |
| Secondary | 38 (7.0) |
| Tertiary | 60 (11.0) |
| Unknown or declined to respond | 429 (78.7) |
| Educational attainment of father—n (%) | |
| Primary | 11 (2.0) |
| Secondary | 33 (6.0) |
| Tertiary | 27 (4.9) |
| Unknown or declined to respond | 475 (87.0) |
| Residence—n (%) | |
| Guadeloupe | 245 (44.9) |
| Martinique | 277 (50.7) |
| French Guiana | 24 (4.4) |
| Previous pregnancies—n (%) | |
| 0 | 131 (24.0) |
| 1 | 150 (27.5) |
| 2 | 128 (23.4) |
| 3+ | 137 (25.1) |
| Previous adverse pregnancy outcomes—n (%) | |
| Congenital abnormalities | 6 (1.1) |
| Stillbirth | 10 (1.8) |
| Medical termination of pregnancy | 10 (1.8) |
| Lifestyle practices during 2016–2017 pregnancy—n (%) | |
| Alcohol consumption | 2 (0.4) |
| Drug use | 6 (1.1) |
| Smoking | 23 (4.2) |
| Use of mosquito repellents | 445 (81.5) |
| Use of larvicides | 337 (61.7) |
| 1B. Infant Characteristics | n = 527 |
| Gestational age (weeks) | |
| Mean ± SD | 38.7 ± 1.9 |
| Delivery type—n (%) | |
| Cesarean | 95 (18.0) |
| Sex—n (%) | |
| Male | 266 (50.5) |
| Birth weight (g) | |
| Mean ± SD | 3112 ± 530 |
| Consultation at 2 M n = 262 (%) | Consultation at 4 M n = 261 (%) | Consultation at 9 M n = 235 (%) | Consultation at 18 M n = 208 (%) | Consultation at 24 M n = 206 (%) | Consultation at Any Time across 24 M n = 310 (%) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ZIKV Infection Status of Child | +ve n = 4 | −ve n = 134 | UD n = 124 | +ve n = 4 | −ve n = 138 | UD n = 119 | +ve n = 4 | −ve n = 128 | UD n = 103 | +ve n = 4 | −ve n = 130 | UD n = 74 | +ve n = 4 | −ve n = 144 | UD n = 58 | +ve n = 5 | −ve n = 162 | UD n = 143 |
| Hearing loss or deficiency * | 0 (0) | 4 (3.0) | 3 (2.4) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (1.0) | 1 (25.0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.7) | 1 (1.7) | 1 (20.0) | 5 (3.1) | 5 (3.5) |
| Visual impairment ** | 1 (25.0) | 8 (6.0) | 3 (2.4) | 0 (0) | 1 (0.7) | 2 (1.7) | 1 (25.0) | 0 (0) | 1 (1.0) | 1 (25.0) | 0 (0) | 1 (1.4) | 0 (0) | 2 (1.4) | 1 (1.7) | 2 (40.0) | 11 (6.8) | 8 (5.6) |
| Seizures, excluding febrile seizures | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) | 1 (1.4) | 0 (0) | 1 (0.7) | 2 (3.4) | 0 (0) | 1 (0.6) | 2 (1.4) |
| Body tone, musculoskeletal or motor abnormalities | 0 (0) | 3 (2.2) | 1 (0.8) | 1 (25.0) | 5 (3.6) | 3 (2.5) | 1 (25.0) | 2 (1.6) | 1 (1.0) | 1 (25.0) | 2 (1.5) | 1 (1.4) | 1 (25.0) | 1 (0.7) | 3 (5.2) | 2 (40.0) | 9 (5.6) | 6 (4.2) |
| Swallowing abnormalities | 0 (0) | 12 (9.0) | 6 (4.8) | 0 (0) | 0 (0) | 1 (0.8) | - | - | - | - | - | - | - | - | - | 0 (0) | 12 (7.4) | 7 (4.9) |
| Post-natal microcephaly | 0 (0) | 0 (0) | 0 (0) | 1 (25.0) | 0 (0) | 0 (0) | 0 (0) | 1 (0.8) | 0 (0) | 1 (25.0) | 1 (0.8) | 0 (0) | 1 (25.0) | 1 (0.7) | 0 (0) | 1 (20.0) | 1 (0.6) | 0 (0) |
| Any selected abnormality *** | 1 (25.0) | 23 (17.2) | 12 (9.7) | 1 (25.0) | 6 (4.3) | 5 (4.2) | 1 (25.0) | 3 (2.3) | 2 (1.9) | 1 (25.0) | 4 (3.1) | 3 (4.0) | 1 (25.0) | 6 (4.2) | 5 (8.6) | 3 (60.0) | 36 (22.2) | 24 (16.7) |
| Imaging abnormality + | 2 (50.0) | 11 (8.2) | 10 (8.1) | 0 (0) | 1 (0.7) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | - | - | - | - | - | - | 2 (40.0) | 12 (7.4) | 10 (7.0) |
| Any selected abnormality, including imaging | 3 (75.0) | 34 (25.4) | 21 (16.9) | 1 (25.0) | 7 (5.1) | 5 (4.2) | 1 (25.0) | 3 (2.3) | 2 (1.9) | 1 (25.0) | 4 (3.1) | 3 (4.1) | 1 (25.0) | 6 (4.2) | 5 (8.6) | 3 (60.0) | 43 (26.5) | 33 (23.1) |
| 3A | Trimester of Maternal ZIKV Infection | All n = 555 (%) | ||
|---|---|---|---|---|
| Severity of Adverse Pregnancy and Early Childhood Outcomes | 1 n = 158 (%) | 2 n = 257 (%) | 3 n = 140 (%) | |
| Severe sequelae or fatality | 24 (15.2) | 11 (4.3) | 2 (1.4) | 37 (6.7) |
| Major abnormalities | 7 (4.4) | 9 (3.5) | 8 (5.7) | 24 (4.3) |
| Mild abnormalities | 23 (14.6) | 38 (14.8) | 23 (16.4) | 84 (15.1) |
| No abnormality reported | 90 (57.0) | 171 (66.5) | 95 (64.1) | 356 (64.1) |
| Unknown | 14 (8.9) | 28 (10.9) | 12 (8.6) | 54 (9.7) |
| 3B | Trimester of Maternal ZIKV Infection | All n = 555 (%) | ||
| Severity of Adverse Pregnancy and Early Childhood Outcomes Related to Maternal ZIKV Infection ** | 1 n = 158 (%) | 2 n = 257 (%) | 3 n = 140 (%) | |
| Severe sequelae or fatality | 11 (7.0) | 7 (2.7) | 2 (1.4) | 20 (3.6) |
| Major abnormalities | 3 (1.9) | 8 (3.1) | 4 (2.9) | 15 (2.7) |
| Mild abnormalities | 15 (9.5) | 19 (7.4) | 18 (12.9) | 52 (9.4) |
| No abnormality reported | 103 (65.2) | 195 (75.9) | 104 (74.3) | 402 (72.4) |
| Unknown | 26 (16.5) | 28 (10.9) | 12 (8.6) | 66 (11.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grant, R.; Flechelles, O.; Elenga, N.; Tressières, B.; Gaete, S.; Hebert, J.-C.; Schaub, B.; Djossou, F.; Mallard, A.; Delver, L.; et al. Consequences of In Utero Zika Virus Exposure and Adverse Pregnancy and Early Childhood Outcomes: A Prospective Cohort Study. Viruses 2022, 14, 2755. https://doi.org/10.3390/v14122755
Grant R, Flechelles O, Elenga N, Tressières B, Gaete S, Hebert J-C, Schaub B, Djossou F, Mallard A, Delver L, et al. Consequences of In Utero Zika Virus Exposure and Adverse Pregnancy and Early Childhood Outcomes: A Prospective Cohort Study. Viruses. 2022; 14(12):2755. https://doi.org/10.3390/v14122755
Chicago/Turabian StyleGrant, Rebecca, Olivier Flechelles, Narcisse Elenga, Benoît Tressières, Stanie Gaete, Jean-Christophe Hebert, Bruno Schaub, Felix Djossou, Adeline Mallard, Lucetta Delver, and et al. 2022. "Consequences of In Utero Zika Virus Exposure and Adverse Pregnancy and Early Childhood Outcomes: A Prospective Cohort Study" Viruses 14, no. 12: 2755. https://doi.org/10.3390/v14122755