
COVID-19 Vaccine Hesitancy in Australian Patients with Solid Organ Cancers

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Study Procedures
2.2. Scales and Measures
- Oxford COVID-19 Vaccine Hesitancy Scale (OHS), a 7-item scale measuring intent to receive a COVID-19 vaccine and vaccine hesitancy [32].
- Oxford COVID-19 Vaccine Confidence and Complacency Scale (OCCS), a 14-item scale measuring attitudes around vaccine complacency and confidence. There are four identified factors: collective importance of a vaccine, belief that the vaccine will work, speed of vaccine development and side effects [32].
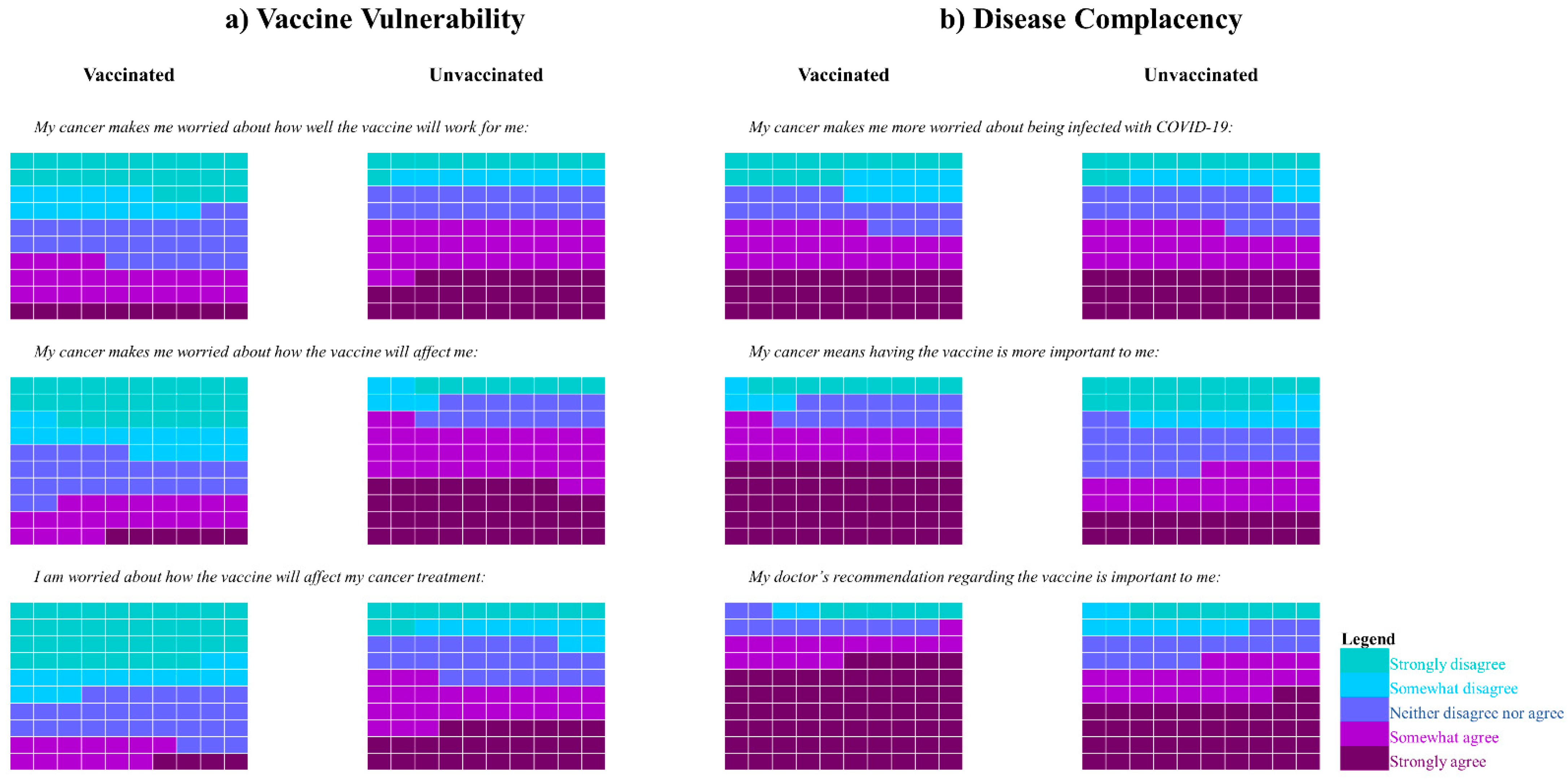
- Disease Influenced Vaccine Acceptance Scale-Six (DIVAS-6), a 6-item scale evaluating the impact of cancer on participants’ attitudes towards COVID-19 vaccination [33]. This scale was developed by the study team and validated in people with serious underlying medical conditions including cancer, diabetes, and multiple sclerosis. It consists of two subscales: the Disease Complacency subscale, which assesses the degree to which a participant’s disease affected their perceived risk of COVID-19 infection, and the Vaccine Vulnerability subscale, which assesses how the participant’s cancer diagnosis and treatment affected their perceived benefits and risks of the vaccine.
2.3. Statistical Analysis
3. Results
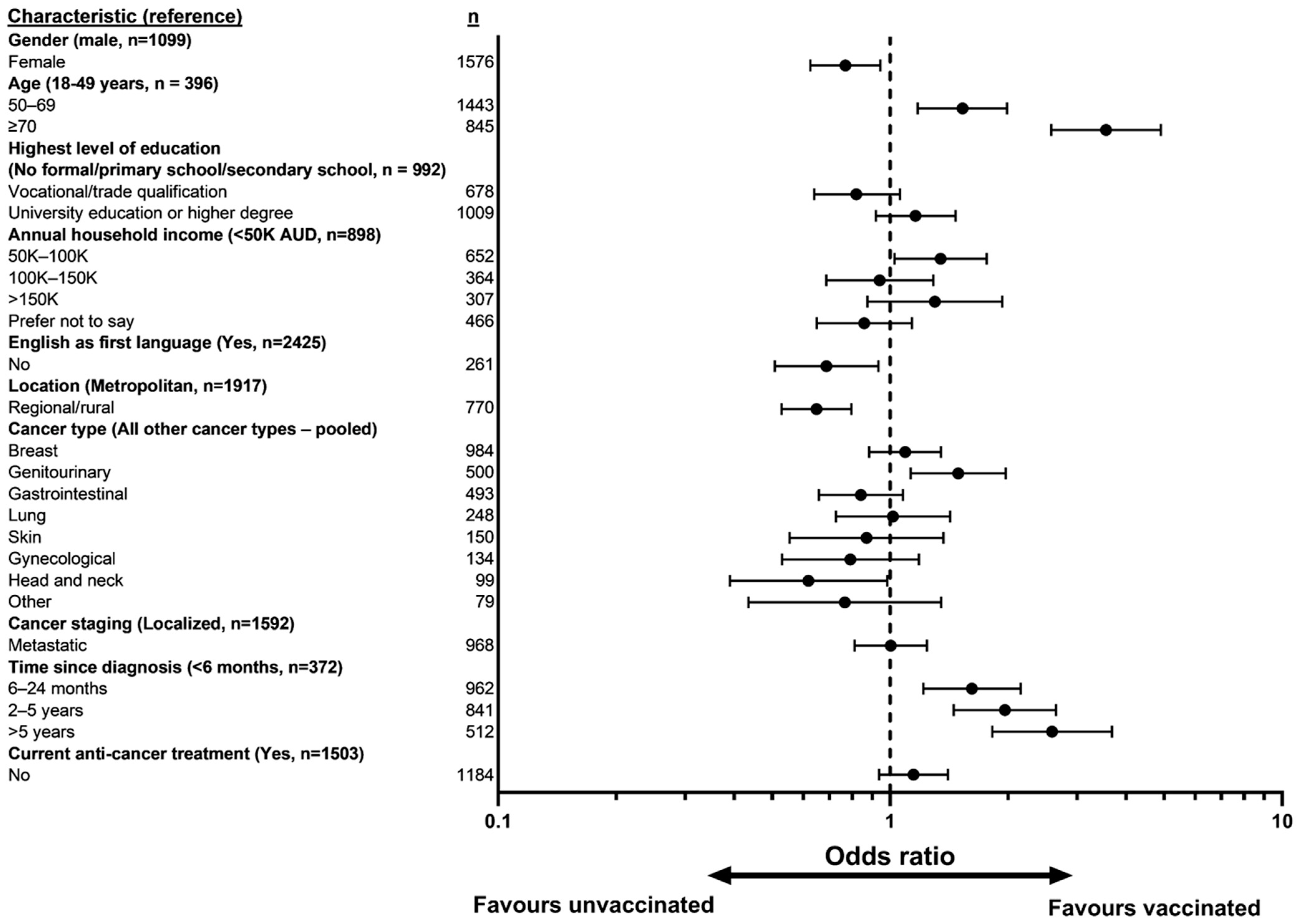
3.1. Patient Characteristics
3.2. COVID-19 Vaccine Uptake
3.3. Oxford COVID-19 Vaccine Hesitancy Scale
3.4. Oxford COVID-19 Vaccine Confidence and Complacency Scale
3.5. Disease Influenced Vaccine Acceptance Scale-6
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 95% CI | 95% confidence interval |
| ATAGI | Australian Technical Advisory Group on Immunization |
| AUD | Australian Dollars |
| AZ | Astra-Zeneca |
| BH | Bendigo Health |
| BMO | Border Medical Oncology |
| CANVACCS | CANcer patients’ perspectives on coronavirus VACCination Survey |
| CCH | Central Coast Hematology |
| CH | Campbelltown Hospital |
| DIVAS-6 | Disease Influenced Vaccine Acceptance Scale-6 |
| ICCH | Icon Cancer Center Hobart |
| K | 1000 |
| LRH | Latrobe Regional Hospital |
| MH | Monash Health |
| NSW | New South Wales |
| OHS | Oxford COVID-19 Vaccine Hesitancy Scale |
| OCCS | Oxford COVID-19 Vaccine Confidence and Complacency Scale |
| OR | Odds ratio |
| QLD | Queensland |
| SCHHS | Sunshine Coast Hospital and Health Service |
| SVHS | St Vincent’s Hospital Sydney |
| r | correlation coefficient. |
| TAS | Tasmania |
| TGA | Therapeutic Goods Administration |
| v. | Versus |
| VIC | Victoria |
| yrs | years |
References
- World Health Organization Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 29 March 2022).
- Liang, W.; Guan, W.; Chen, R.; Wang, W.; Li, J.; Xu, K.; Li, C.; Ai, Q.; Lu, W.; Liang, H.; et al. Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. Lancet Oncol. 2020, 213, 335–337. [Google Scholar] [CrossRef]
- Khoury, E.; Nevitt, S.; Madsen, W.R.; Turtle, L.; Davies, G.; Palmieri, C. Differences in Outcomes and Factors Associated with Mortality Among Patients with SARS-CoV-2 Infection and Cancer Compared with Those without Cancer: A Systematic Review and Meta-analysis. JAMA Netw. Open 2022, 5, e2210880. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Henry, D.A.; Jones, M.A.; Stehlik, P.; Glasziou, P.P. Effectiveness of COVID-19 vaccines: Findings from real world studies. Med. J. Aust. 2021, 215, 149. [Google Scholar] [CrossRef]
- Australian Government Department of Health. Priority Groups for COVID-19 Vaccination Program: Phase 1b. Available online: https://www.health.gov.au/sites/default/files/documents/2021/03/priority-groups-for-COVID-19-vaccination-program-phase-1b_1.pdf (accessed on 29 March 2022).
- Dooling, K.; Marin, M.; Wallace, M.; McClung, N.; Chamberland, M.; Lee, G.M.; Talbot, K.; Romero, J.R.; Bell, B.P.; Oliver, S.E. The Advisory Committee on Immunization Practices’ Updated Interim Recommendation for Allocation of COVID-19 Vaccine—United States, December 2020. MMWR 2021, 69, 1657–1660. [Google Scholar] [CrossRef]
- Government of the United Kingdom. COVID-19 Vaccination First Phase Priority Groups. Available online: https://www.gov.uk/government/publications/COVID-19-vaccination-care-home-and-healthcare-settings-posters/COVID-19-vaccination-first-phase-priority-groups (accessed on 6 March 2022).
- Cavanna, L.; Citterio, C.; Biasini, C.; Madaro, S.; Bacchetta, N.; Lis, A.; Cremona, G.; Muroni, M.; Bernuzzi, P.; Cascio, G.L.; et al. COVID-19 vaccines in adult cancer patients with solid tumours undergoing active treatment: Seropositivity and safety. A prospective observational study in Italy. Eur. J. Cancer 2021, 157, 441–449. [Google Scholar] [CrossRef]
- Naranbhai, V.; Pernat, C.A.; Gavralidis, A.; Denis, K.J.S.; Lam, E.C.; Spring, L.M.; Isakoff, S.J.; Farmer, J.R.; Zubiri, L.; Hobbs, G.; et al. Immunogenicity and Reactogenicity of SARS-CoV-2 Vaccines in Patients with Cancer: The CANVAX Cohort Study. J. Clin. Oncol. 2022, 40, 12–23. [Google Scholar] [CrossRef]
- So, A.; McGrath, H.; Ting, J.; Srikandarajah, K.; Germanou, S.; Moss, C.; Russell, B.; Monroy-Iglesias, M.; Dolly, S.; Irshad, S.; et al. COVID-19 Vaccine Safety in Cancer Patients: A Single Centre Experience. Cancers 2021, 13, 3573. [Google Scholar] [CrossRef]
- Nehal, K.R.; Steendam, L.M.; Ponce, M.C.; van der Hoeven, M.; Smit, G.S.A. Worldwide Vaccination Willingness for COVID-19: A Systematic Review and Meta-Analysis. Vaccines 2021, 9, 1071. [Google Scholar] [CrossRef] [PubMed]
- Tsai, R.; Hervey, J.; Hoffman, K.; Wood, J.; Johnson, J.; Deighton, D.; Clermont, D.; Loew, B.; Goldberg, S.L. COVID-19 vaccine hesitancy and acceptance among individuals with cancer, autoimmune diseases, and other serious comorbid conditions: A cross-sectional internet-based survey. JMIR Public Health Surveill. 2021, 8, e29872. [Google Scholar] [CrossRef] [PubMed]
- Bartley, N.; Havard, P.; Butow, P.; Shaw, J. COVID-19 Cancer Stakeholder Authorship Group. Experiences and perspectives of cancer stakeholders regarding COVID-19 vaccination. Asia Pacific J. Clin. Oncol. 2022. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; Reingold, A.; et al. Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- The Lancet Child & Adolescent Health. Vaccine hesitancy: A generation at risk. Lancet Child Adolesc Health 2019, 3, 281. [Google Scholar] [CrossRef]
- World Health Organization. Ten Health Issues WHO Will Tackle This Year. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 6 March 2022).
- Troiano, G.; Nardi, A. Vaccine hesitancy in the era of COVID-19. Public Health 2021, 194, 245–251. [Google Scholar] [CrossRef]
- Servidio, R.; Malvaso, A.; Vizza, D.; Valente, M.; Campagna, M.R.; Iacono, M.L.; Martin, L.R.; Bruno, F. The intention to get COVID-19 vaccine and vaccine uptake among cancer patients: An extension of the theory of planned behaviour (TPB). Support. Care Cancer 2022, 1–10. [Google Scholar] [CrossRef]
- Day, D.; Grech, L.; Nguyen, M.; Bain, N.; Kwok, A.; Harris, S.; Chau, H.; Chan, B.; Blennerhassett, R.; Nott, L.; et al. Serious Underlying Medical Conditions and COVID-19 Vaccine Hesitancy: A Large Cross-Sectional Analysis from Australia. Vaccines 2022, 10, 851. [Google Scholar] [CrossRef]
- Rodriguez, M.; López-Cepero, A.; Ortiz-Martínez, A.P.; Fernández-Repollet, E.; Pérez, C.M. Influence of Health Beliefs on COVID-19 Vaccination among Individuals with Cancer and Other Comorbidities in Puerto Rico. Vaccines 2021, 9, 994. [Google Scholar] [CrossRef]
- Dwyer, A.; Marosits, M.; Weltzien, E.; Garcia, R.; Davis, A. Landscape of COVID-19 vaccine uptake in the colorectal cancer community: Responding to community needs. J. Clin. Oncol. 2021, 39, e15577. [Google Scholar] [CrossRef]
- Brodziak, A.; Sigorski, D.; Osmola, M.; Wilk, M.; Gawlik-Urban, A.; Kiszka, J.; Machulska-Ciuraj, K.; Sobczuk, P. Attitudes of Patients with Cancer towards Vaccinations—Results of Online Survey with Special Focus on the Vaccination against COVID-19. Vaccines 2021, 9, 411. [Google Scholar] [CrossRef] [PubMed]
- Di Noia, V.; Renna, D.; Barberi, V.; Di Civita, M.; Riva, F.; Costantini, G.; Dell’Aquila, E.; Russillo, M.; Bracco, D.; La Malfa, A.M.; et al. The first report on coronavirus disease 2019 (COVID-19) vaccine refusal by patients with solid cancer in Italy: Early data from a single-institute survey. Eur. J. Cancer 2021, 153, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Mejri, N.; Berrazega, Y.; Ouertani, E.; Rachdi, H.; Bohli, M.; Kochbati, L.; Boussen, H. Understanding COVID-19 vaccine hesitancy and resistance: Another challenge in cancer patients. Support. Care Cancer 2022, 30, 289–293. [Google Scholar] [CrossRef]
- Barrière, J.; Gal, J.; Hoch, B.; Cassuto, O.; Leysalle, A.; Chamorey, E.; Borchiellini, D. Acceptance of SARS-CoV-2 vaccination among French patients with cancer: A cross-sectional survey. Ann. Oncol. 2021, 32, 673–674. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, M.; Bain, N.; Grech, L.; Choi, T.; Harris, S.; Chau, H.; Freeman, D.; Kwok, A.; Williams, J.; McCartney, A.; et al. COVID-19 vaccination rates, intent, and hesitancy in patients with solid organ and blood cancers: A multicenter study. Asia Pac. J. Clin. Oncol. 2022, 18, 13754. [Google Scholar] [CrossRef]
- Zhuang, W.; Zhang, J.; Wei, P.; Lan, Z.; Chen, R.; Zeng, C.; Shi, Q.; Qiao, G. Misconception contributed to COVID-19 vaccine hesitancy in patients with lung cancer or ground-glass opacity: A cross-sectional study of 324 Chinese patients. Hum. Vaccines Immunother. 2021, 17, 5016–5023. [Google Scholar] [CrossRef] [PubMed]
- Qualtrics, X.M. Available online: https://www.qualtrics.com/au/ (accessed on 22 June 2022).
- Freeman, D.; Loe, B.S.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Jenner, L.; Petit, A.; Lewandowsky, S.; Vanderslott, S.; et al. COVID-19 vaccine hesitancy in the UK: The Oxford coronavirus explanations, attitudes, and narratives survey (Oceans) II. Psychol. Med. 2020, 1–15. [Google Scholar] [CrossRef]
- Grech, L.; Loe, B.S.; Day, D.; Freeman, D.; Kwok, A.; Nguyen, M.; Bain, N.; Segelov, E. The Disease Influenced Vaccine Acceptance Scale-Six (DIVAS-6): Validation of a Measure to Assess Disease-Related COVID-19 Vaccine Attitudes and Concerns. Behav. Med. 2022, 1–10. [Google Scholar] [CrossRef]
- Freeman, D.; Lambe, S.; Yu, L.M.; Freeman, J.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Petit, A.; Vanderslott, S.; et al. Injection fears and COVID-19 vaccine hesitancy. Psychol. Med. 2021, 1–11. [Google Scholar] [CrossRef]
- Freeman, D.; Loe, B.S.; Yu, L.-M.; Freeman, J.; Chadwick, A.; Vaccari, C.; Shanyinde, M.; Harris, V.; Waite, F.; Rosebrock, L.; et al. Effects of different types of written vaccination information on COVID-19 vaccine hesitancy in the UK (OCEANS-III): A single-blind, parallel-group, randomised controlled trial. Lancet Public Health 2021, 6, e416–e427. [Google Scholar] [CrossRef]
- Australian Government Department of Health. COVID-19 Vaccine Roll-Out Update 06 October 2021. Available online: https://www.health.gov.au/sites/default/files/documents/2021/10/COVID-19-vaccine-rollout-update-6-october-2021.pdf (accessed on 6 April 2022).
- Kosmidis, P.A.; Lagogianni, C.; Kosmidis, T. Multifactorial analysis of cancer patients’ willingness for COVID-19 vaccination. J. Clin. Oncol. 2021, 39, 12062. [Google Scholar] [CrossRef]
- Chun, J.; Kim, S.; Park, E.; Park, S.-Y.; Koh, S.-J.; Cha, Y.; Yoo, H.; Joung, J.; Yoon, H.; Eom, B.; et al. Cancer Patients’ Willingness to Take COVID-19 Vaccination: A Nationwide Multicenter Survey in Korea. Cancers 2021, 13, 3883. [Google Scholar] [CrossRef] [PubMed]
- Denby, C. Vaccine Hesitancy Tracker. Melbourne Institute: Applied Economic & Social Research. 2022. Available online: https://melbourneinstitute.unimelb.edu.au/publications/research-insights/ttpn/vaccination-report (accessed on 10 April 2022).
- Shroff, R.T.; Chalasani, P.; Wei, R.; Pennington, D.; Quirk, G.; Schoenle, M.V.; Peyton, K.L.; Uhrlaub, J.L.; Ripperger, T.J.; Jergović, M.; et al. Immune responses to two and three doses of the BNT162b2 mRNA vaccine in adults with solid tumors. Nat. Med. 2021, 27, 2002–2011. [Google Scholar] [CrossRef] [PubMed]
- Rottenberg, Y.; Grinshpun, A.; Ben-Dov, I.Z.; Djian, E.D.; Wolf, D.G.; Kadouri, L. Assessment of Response to a Third Dose of the SARS-CoV-2 BNT162b2 mRNA Vaccine in Patients With Solid Tumors Undergoing Active Treatment. JAMA Oncol. 2022, 8, 300. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.R.Y.B.; Wong, S.Y.; Chai, L.Y.A.; Lee, S.C.; Lee, M.X.; Muthiah, M.D.; Tay, S.H.; Teo, C.B.; Tan, B.K.J.; Chan, Y.H.; et al. Efficacy of COVID-19 vaccines in immunocompromised patients: Systematic review and meta-analysis. BMJ 2022, 376, e068632. [Google Scholar] [CrossRef]
- Bottomley, A. Anxiety and the adult cancer patient. Eur. J. Cancer Care 1998, 7, 217–224. [Google Scholar] [CrossRef]
- Villarreal-Garza, C.; Vaca-Cartagena, B.F.; Becerril-Gaitan, A.; Ferrigno, A.S.; Mesa-Chavez, F.; Platas, A.; Platas, A. Attitudes and Factors Associated With COVID-19 Vaccine Hesitancy Among Patients With Breast Cancer. JAMA Oncol. 2021, 7, 1242. [Google Scholar] [CrossRef]
- Noronha, V.; Abraham, G.; Bondili, S.K.; Rajpurohit, A.; Menon, R.P.; Gattani, S.; Trikha, M.; Tudu, R.; Kota, K.K.; Singh, A.K.; et al. COVID-19 vaccine uptake and vaccine hesitancy in Indian patients with cancer: A questionnaire-based survey. Cancer Res. Stat. Treat. 2021, 4, 211–218. [Google Scholar]
- Kelkar, A.; Blake, J.; Cherabuddi, K.; Cornett, H.; McKee, B.; Cogle, C. Vaccine Enthusiasm and Hesitancy in Cancer Patients and the Impact of a Webinar. Healthcare 2021, 9, 351. [Google Scholar] [CrossRef]
- Vanderpool, R.C.; Gaysynsky, A.; Chou, W.-Y.S.; Tonorezos, E.S. Using Behavioral Science to Address COVID-19 Vaccine Hesitancy Among Cancer Survivors: Communication Strategies and Research Opportunities. J. Behav. Med. 2022, 1–11. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. COVID-19 Resources. NCCN. Available online: https://www.nccn.org/COVID-19 (accessed on 31 May 2022).
- European Society for Medical Oncology. ESMO Statements on Vaccination against COVID-19 in People with Cancer. Available online: https://www.esmo.org/COVID-19-and-cancer/COVID-19-vaccination (accessed on 31 May 2022).
- American Society of Clinical Oncology. COVID-19 Vaccines & Patients with Cancer. 2021. Available online: https://www.asco.org/COVID-resources/vaccines-patients-cancer (accessed on 31 May 2022).
- Kanjanapan, Y.; Blinman, P.; Underhill, C.; Karikios, D.; Segelov, E.; Yip, D. Medical Oncology Group of Australia position statement: COVID-19 vaccination in patients with solid tumours. Intern. Med. J. 2021, 51, 955–959. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, J.; Bagot, K.L.; Tuckerman, J.; Biezen, R.; Oliver, J.; Jos, C.; Ong, S.; Manski-Nankervis, J.-A.; Seala, H.; Sanci, L.; et al. Qualitative exploration of intentions, concerns and information needs of vaccine-hesitant adults initially prioritised to receive COVID-19 vaccines in Australia. Aust N. Z. J. Public Health 2022, 46, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Body, A.; Ahern, E.; Segelov, E. COVID-19 vaccinations for patients with cancer: Many remain unvaccinated despite having priority in the vaccine rollout. Intern. Med. J. 2021, 51, 1760. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.L.; Wiysonge, C. Social media and vaccine hesitancy. BMJ Glob. Health 2020, 5, e004206. [Google Scholar] [CrossRef] [PubMed]
- Sabahelzain, M.M.; Hartigan-Go, K.; Larson, H.J. The politics of COVID-19 vaccine confidence. Curr. Opin. Immunol. 2021, 71, 92–96. [Google Scholar] [CrossRef]
- Ullah, I.; Khan, K.S.; Tahir, M.J.; Ahmed, A.; Harapan, H. Myths and conspiracy theories on vaccines and COVID-19: Potential effect on global vaccine refusals. Vacunas 2021, 22, 93–97. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total n = 2691 (%) | Vaccinated n = 2143 (79.7%) | Unvaccinated n = 546 (20.3%) | |
|---|---|---|---|
| Male | 1101 (40.9) | 898 (81.7) | 201 (18.3) |
| Female * | 1578 (58.6) | 1235 (78.3) | 343 (21.7) |
| Age: mean (SD) | 62.5 (11.8) | 63.7 (11.5) | 58.0 (12.0) |
| Age (years) | |||
| 18–49 | 396 (14.7) | 270 (68.2) | 126 (31.8) |
| 50–69 | 1444 (53.8) | 1113 (77.1) | 331 (22.9) |
| ≥70 | 847 (31.5) | 757 (89.5) | 89 (10.5) |
| Highest level of education ** | |||
| No formal/primary school | 72 (2.7) | 52 (72.2) | 20 (27.8) |
| Secondary school | 921 (34.3) | 726 (78.8) | 195 (21.2) |
| Vocational/Trade | 679 (25.2) | 526 (77.5) | 153 (22.5) |
| University | 1009 (37.5) | 834 (82.7) | 175 (17.3) |
| Annual household income (AUD) | |||
| <50 K | 898 (33.4) | 694 (77.3) | 204 (22.7) |
| 50 K–100 K | 653 (24.3) | 543 (83.2) | 110 (16.8) |
| 100 K–150 K | 364 (13.5) | 286 (78.6) | 78 (21.4) |
| >150 K | 307 (11.4) | 269 (87.6) | 38 (12.4) |
| Prefer not to say | 467 (17.4) | 351 (75.2) | 116 (24.8) |
| Aboriginal/Torres Strait Islander *** | |||
| Yes | 38 (1.4) | 32 (84.2) | 6 (15.8) |
| English as dominant language | |||
| Yes | 2429 (90.3) | 1963 (80.9) | 464 (19.1) |
| No | 261 (9.7) | 180 (69.0) | 81 (31.0) |
| Location | |||
| Metropolitan | 1918 (71.3) | 1594 (83.1) | 324 (16.9) |
| Regional/rural | 773 (28.7) | 549 (71.2) | 222 (22.8) |
| Cancer type | |||
| Breast | 986 (36.6) | 807 (81.8) | 179 (18.2) |
| Genitourinary | 501 (18.6) | 424 (84.8) | 76 (15.2) |
| Gastrointestinal | 493 (18.3) | 375 (76.1) | 118 (23.9) |
| Lung | 248 (9.2) | 194 (78.2) | 54 (21.8) |
| Skin | 151 (5.6) | 123 (82.0) | 27 (18.0) |
| Gynecological | 134 (5.0) | 91 (67.9) | 43 (32.1) |
| Head and Neck | 99 (3.7) | 69 (69.1) | 30 (30.3) |
| Other | 79 (2.9) | 60 (75.9) | 19 (24.1) |
| Cancer stage | |||
| Localized | 1593 (59.2) | 1291 (81.1) | 301 (18.9) |
| Metastatic | 971 (36.1) | 770 (79.4) | 200 (20.6) |
| Unsure/Other | 127 (4.7) | 82 (64.6) | 45 (35.4) |
| Time since diagnosis | |||
| <6 months | 372 (13.8) | 251 (67.5) | 121 (32.5) |
| 6–24 months | 964 (35.8) | 755 (78.4) | 208 (21.6) |
| 2–5 years | 841 (31.3) | 695 (82.6) | 146 (17.4) |
| >5 years | 514 (19.1) | 442 (86.2) | 71 (13.8) |
| Current anti-cancer treatment | |||
| Yes | 1506 (56.0) | 1181 (78.5) | 323 (21.5) |
| No | 1185 (44.0) | 962 (81.2) | 223 (18.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bain, N.; Nguyen, M.; Grech, L.; Day, D.; McCartney, A.; Webber, K.; Kwok, A.; Harris, S.; Chau, H.; Chan, B.; et al. COVID-19 Vaccine Hesitancy in Australian Patients with Solid Organ Cancers. Vaccines 2022, 10, 1373. https://doi.org/10.3390/vaccines10091373
Bain N, Nguyen M, Grech L, Day D, McCartney A, Webber K, Kwok A, Harris S, Chau H, Chan B, et al. COVID-19 Vaccine Hesitancy in Australian Patients with Solid Organ Cancers. Vaccines. 2022; 10(9):1373. https://doi.org/10.3390/vaccines10091373
Chicago/Turabian StyleBain, Nathan, Mike Nguyen, Lisa Grech, Daphne Day, Amelia McCartney, Kate Webber, Alastair Kwok, Sam Harris, Hieu Chau, Bryan Chan, and et al. 2022. "COVID-19 Vaccine Hesitancy in Australian Patients with Solid Organ Cancers" Vaccines 10, no. 9: 1373. https://doi.org/10.3390/vaccines10091373