
Laboratory Indicators for Identifying Hand, Foot, and Mouth Disease Severity: A Systematic Review and Meta-Analysis
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Diagnosis and Group Classification
2.2. Literature Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction and Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Study Inclusion and Characteristics
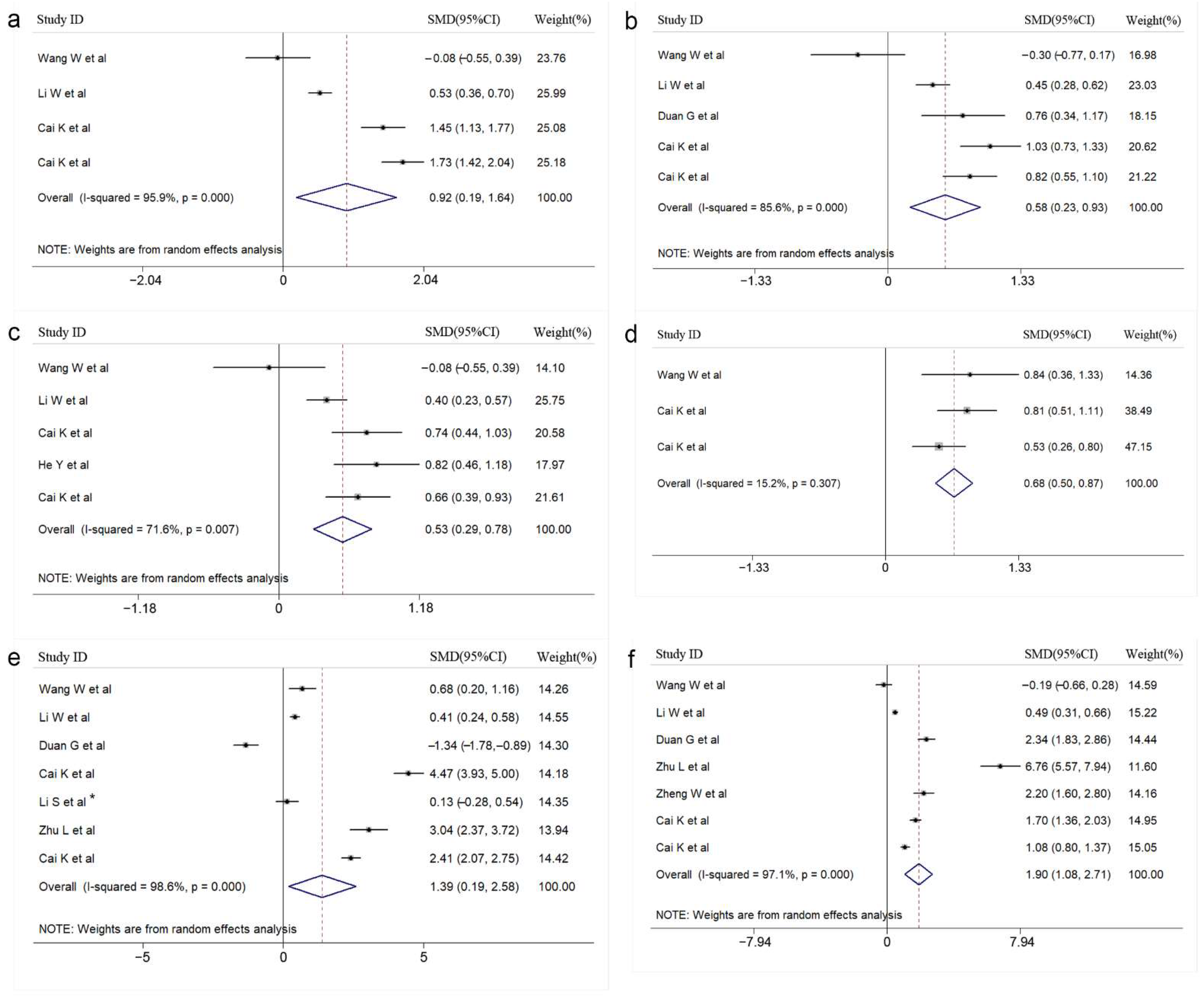
3.2. Results of the Meta-Analysis
3.3. Subgroup Analysis
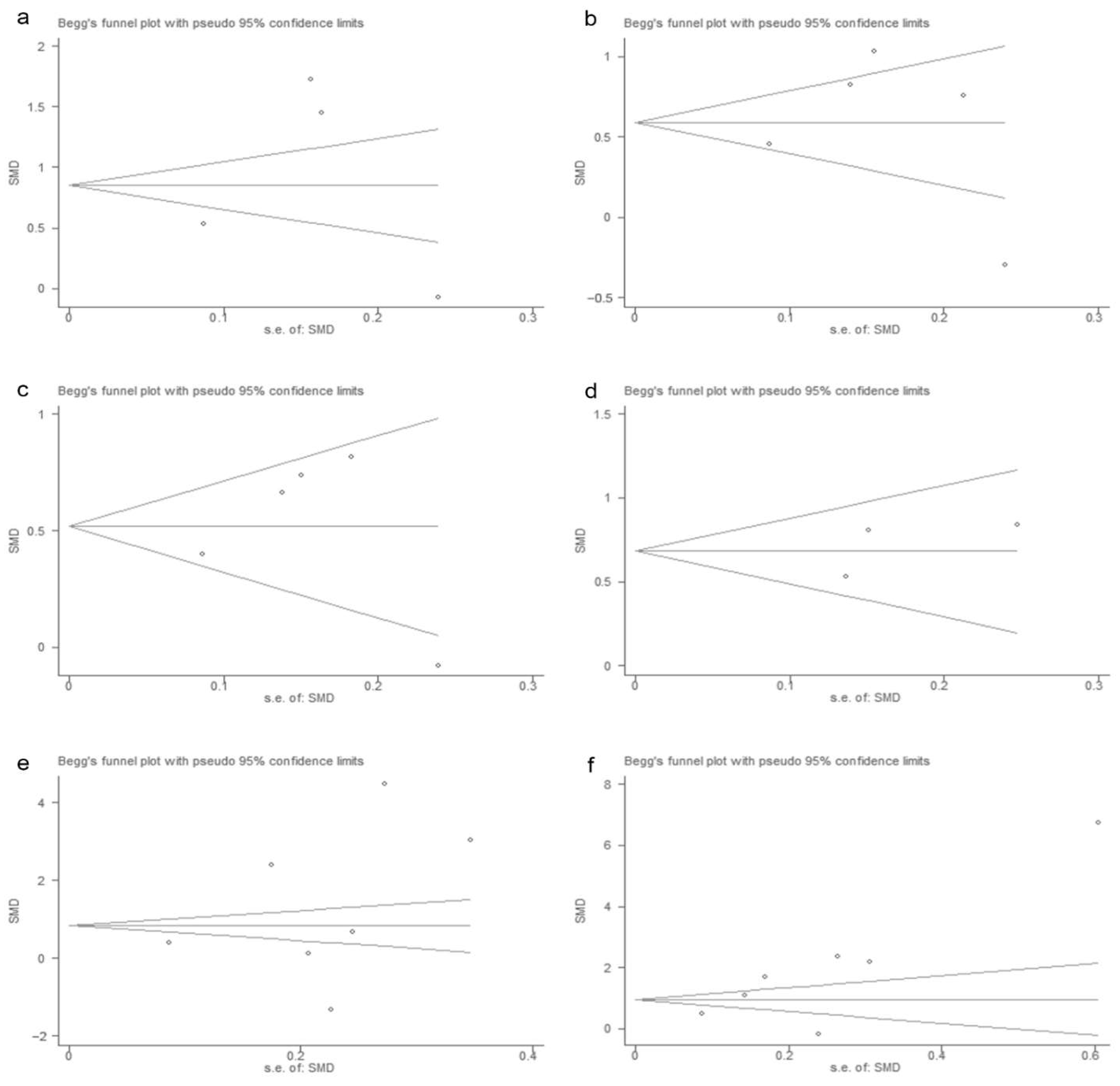
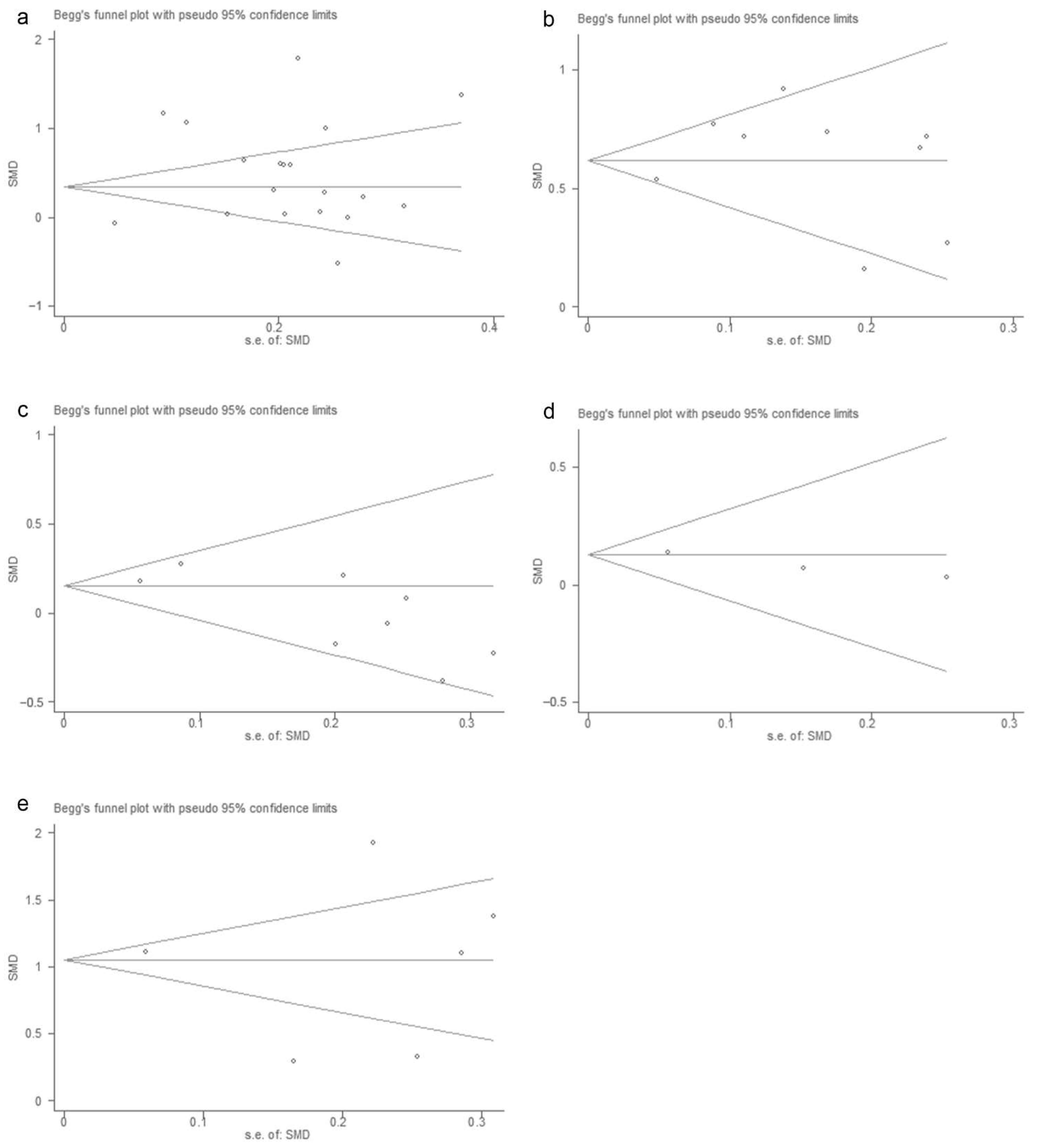
3.4. Publication Bias
3.5. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bian, L.; Gao, F.; Mao, Q.; Sun, S.; Wu, X.; Liu, S.; Yang, X.; Liang, Z. Hand, foot, and mouth disease associated with coxsackievirus A10: More serious than it seems. Expert Rev. Anti-Infect. Ther. 2019, 17, 233–242. [Google Scholar] [CrossRef]
- Long, L.; Gao, L.-D.; Hu, S.-X.; Luo, K.-W.; Chen, Z.-H.; Ronsmans, C.; Zhou, D.L.; Lan, Y.J. Risk factors for death in children with severe hand, foot, and mouth disease in Hunan. China. Infect. Dis. 2016, 48, 744–748. [Google Scholar] [CrossRef]
- Esposito, S.; Principi, N. Hand, foot and mouth disease: Current knowledge on clinical manifestations, epidemiology, aetiology and prevention. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 391–398. [Google Scholar] [CrossRef]
- Sarma, N. Hand, foot, and mouth disease: Current scenario and Indian perspective. Indian J. Derm. Venereol. Leprol. 2013, 79, 165–175. [Google Scholar] [CrossRef]
- Aswathyraj, S.; Arunkumar, G.; Alidjinou, E.K.; Hober, D. Hand, foot and mouth disease (HFMD): Emerging epidemiology and the need for a vaccine strategy. Med. Microbiol. Immunol. 2016, 205, 397–407. [Google Scholar] [CrossRef]
- Michos, A.G.; Syriopoulou, V.P.; Hadjichristodoulou, C.; Daikos, G.L.; Lagona, E.; Douridas, P.; Mostrou, G.; Theodoridou, M. Aseptic meningitis in children: Analysis of 506 cases. PLoS ONE 2007, 2, e674. [Google Scholar] [CrossRef]
- Shi, C.; Liu, J.; Shi, P.; Ji, H.; Shen, Y.; Qian, Y.H. Epidemiological characteristics and influential factors of hand, foot, and mouth disease reinfection in Wuxi, China, 2008–2016. BMC Infect. Dis. 2018, 18, 472. [Google Scholar] [CrossRef] [Green Version]
- Tyring, S.K. Hand foot and mouth disease: Enteroviral load and disease severity. EBioMedicine 2020, 62, 103115. [Google Scholar] [CrossRef]
- Liu, Y.; Fu, C.; Wu, S.; Chen, X.; Shi, Y.; Zhou, B.; Zhang, L.; Zhang, F.; Wang, Z.; Zhang, Y.; et al. A novel finding for enterovirus virulence from the capsid protein VP1 of EV71 circulating in mainland China. Virus Genes 2014, 48, 260–272. [Google Scholar] [CrossRef]
- Huang, S.W.; Cheng, H.L.; Hsieh, H.Y.; Chang, C.L.; Tsai, H.P.; Kuo, P.H.; Wang, S.M.; Liu, C.C.; Su, I.J.; Wang, J.R. Mutations in the non-structural protein region contribute to intra-genotypic evolution of enterovirus 71. J. Biomed. Sci. 2014, 21, 33. [Google Scholar] [CrossRef]
- Yu, G.; Li, Y.; Cai, J.; Yu, D.; Tang, J.; Zhai, W.; Wei, Y.; Chen, S.; Chen, Q.; Qin, J. Short-term effects of meteorological factors and air pollution on childhood hand-foot-mouth disease in Guilin, China. Sci. Total. Environ. 2019, 646, 460–470. [Google Scholar] [CrossRef]
- Wang, S.M.; Liu, C.C.; Tseng, H.W.; Wang, J.R.; Huang, C.C.; Chen, Y.J.; Yang, Y.J.; Lin, S.J.; Yeh, T.F. Clinical spectrum of enterovirus 71 infection in children in southern Taiwan, with an emphasis on neurological complications. Clin. Infect. Dis. 1999, 29, 184–190. [Google Scholar] [CrossRef]
- Yi, L.; Lu, J.; Kung, H.F.; He, M.L. The virology and developments toward control of human enterovirus 71. Crit. Rev. Microbiol. 2011, 37, 313–327. [Google Scholar] [CrossRef]
- Gonzalez, G.; Carr, M.J.; Kobayashi, M.; Hanaoka, N.; Fujimoto, T. Enterovirus-Associated Hand-Foot and Mouth Disease and Neurological Complications in Japan and the Rest of the World. Int. J. Mol. Sci. 2019, 20, 5021. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, N.T.; Pham, H.V.; Hoang, C.Q.; Nguyen, T.M.; Nguyen, L.T.; Phan, H.C.; Phan, L.T.; Vu, L.N.; Tran-Minh, N.N. Epidemiological and clinical characteristics of children who died from hand, foot and mouth disease in Vietnam, 2011. BMC Infect. Dis. 2014, 14, 341. [Google Scholar] [CrossRef] [Green Version]
- Puenpa, J.; Mauleekoonphairoj, J.; Linsuwanon, P.; Suwannakarn, K.; Chieochansin, T.; Korkong, S.; Theamboonlers, A.; Poovorawan, Y. Prevalence and characterization of enterovirus infections among pediatric patients with hand foot mouth disease, herpangina and influenza like illness in Thailand, 2012. PLoS ONE 2014, 9, e98888. [Google Scholar]
- NikNadia, N.; Sam, I.C.; Rampal, S.; WanNorAmalina, W.; NurAtifah, G.; Verasahib, K.; Ong, C.C.; MohdAdib, M.; Chan, Y.F. Cyclical Patterns of Hand, Foot and Mouth Disease Caused by Enterovirus A71 in Malaysia. PLoS Negl. Trop Dis. 2016, 10, e0004562. [Google Scholar] [CrossRef] [Green Version]
- Palani, S.; Nagarajan, M.; Biswas, A.K.; Maile, A.; Paluru, V. B1c genetic subtype of coxsackievirus A16 associated with hand, foot and mouth disease in Andaman Islands, India. Trans. R Soc. Trop. Med. Hyg. 2016, 110, 421–423. [Google Scholar] [CrossRef]
- Li, X.W.; Ni, X.; Qian, S.Y.; Wang, Q.; Jiang, R.M.; Xu, W.B.; Zhang, Y.C.; Yu, G.J.; Chen, Q.; Shang, Y.X.; et al. Chinese guidelines for the diagnosis and treatment of hand, foot and mouth disease (2018 edition). World J. Pediatrics 2018, 14, 437–447. [Google Scholar] [CrossRef]
- Shekhar, K.; Lye, M.S.; Norlijah, O.; Ong, F.; Looi, L.M.; Khuzaiah, R.; Marzuki, I.; Hussein, I.; Wong, S.L.; Mohan, J.; et al. Deaths in children during an outbreak of hand, foot and mouth disease in Peninsular Malaysia--clinical and pathological characteristics. Med. J. Malays. 2005, 60, 297–304. [Google Scholar]
- Zhang, Y.; Liu, H.; Wang, L.; Yang, F.; Hu, Y.; Ren, X.; Li, G.; Yang, Y.; Sun, S.; Li, Y.; et al. Comparative study of the cytokine/chemokine response in children with differing disease severity in enterovirus 71-induced hand, foot, and mouth disease. PLoS ONE 2013, 8, e67430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, T.Y.; Chang, L.Y.; Huang, Y.C.; Hsu, K.H.; Chiu, C.H.; Yang, K.D. Different proinflammatory reactions in fatal and non-fatal enterovirus 71 infections: Implications for early recognition and therapy. Acta Paediatr. 2002, 91, 632–635. [Google Scholar] [CrossRef] [PubMed]
- Kao, S.J.; Yang, F.L.; Hsu, Y.H.; Chen, H.I. Mechanism of fulminant pulmonary edema caused by enterovirus 71. Clin. Infect. Dis. 2004, 38, 1784–1788. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Cai, C.; Feng, J.; Li, X.; Wang, Y.; Yang, J.; Chen, Z. Peripheral T lymphocyte subset imbalances in children with enterovirus 71-induced hand, foot and mouth disease. Virus Res. 2014, 180, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Zhou, J.; Xie, G.; Zheng, S.; Lou, B.; Chen, Y.; Wu, Y. The Epidemiological and Clinical Characteristics of Hand, Foot, and Mouth Disease in Hangzhou, China, 2016 to 2018. Clin. Pediatr. 2020, 59, 656–662. [Google Scholar] [CrossRef]
- Liu, Y.X.; Xie, J.J.; He, Y.X.; Liu, W.L.; Zhang, M.X.; Le, X.H.; Fu, D.; Chen, X.C.; Yang, G.L.; Cao, D.Z.; et al. Study of the clinical and laboratory features of hand-foot-mouth disease. Chin. J. Exp. Clin. Virol. 2008, 22, 475–477. [Google Scholar]
- Lin, T.Y.; Hsia, S.H.; Huang, Y.C.; Wu, C.T.; Chang, L.Y. Proinflammatory cytokine reactions in enterovirus 71 infections of the central nervous system. Clin. Infect. Dis. 2003, 36, 269–274. [Google Scholar] [CrossRef] [Green Version]
- Chong, C.Y.; Chan, K.P.; Shah, V.A.; Ng, W.Y.; Lau, G.; Teo, T.E.; Lai, S.H.; Ling, A.E. Hand, foot and mouth disease in Singapore: A comparison of fatal and non-fatal cases. Acta Paediatr. 2003, 92, 1163–1169. [Google Scholar] [CrossRef]
- Wang, Q.; Zhang, W.; Zhang, Y.; Yan, L.; Wang, S.; Zhang, J.; Sun, J.; Chang, Z.; Wang, Z. Clinical features of severe cases of hand, foot and mouth disease with EV71 virus infection in China. Arch. Med. Sci. 2014, 10, 510–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, L.Y.; Lin, T.Y.; Hsu, K.H.; Huang, Y.C.; Lin, K.L.; Hsueh, C.; Shih, S.R.; Ning, H.C.; Hwang, M.S.; Wang, H.S.; et al. Clinical features and risk factors of pulmonary oedema after enterovirus-71-related hand, foot, and mouth disease. Lancet 1999, 354, 1682–1686. [Google Scholar] [CrossRef]
- Griffiths, M.J.; Ooi, M.H.; Wong, S.C.; Mohan, A.; Podin, Y.; Perera, D.; Chieng, C.H.; Tio, P.H.; Cardosa, M.J.; Solomon, T. In Enterovirus 71 Encephalitis with Cardio-Respiratory Compromise, Elevated Interleukin 1 beta, Interleukin 1 Receptor Antagonist, and Granulocyte Colony-Stimulating Factor Levels Are Markers of Poor Prognosis. J. Infect. Dis. 2012, 206, 881–892. [Google Scholar] [CrossRef] [PubMed]
- Shao, P.; Wu, X.; Li, H.; Wu, Z.; Yang, Z.; Yao, H. Clinical signifcance of inflammatory cytokine and chemokine expression in hand, foot and mouth disease. Mol. Med. Rep. 2017, 15, 2859–2866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, H.; Li, S.; Zheng, J.; Cai, C.; Ye, B.; Yang, J.; Chen, Z. Cerebrospinal fluid Th1/Th2 cytokine profiles in children with enterovirus 71-associated meningoencephalitis. Microbiol. Immunol. 2015, 59, 152–159. [Google Scholar] [CrossRef] [PubMed]
- McLoughlin, R.M.; Witowski, J.; Robson, R.L.; Wilkinson, T.S.; Hurst, S.M.; Williams, A.S.; Williams, J.D.; Rose-John, S.; Jones, S.A.; Topley, N. Interplay between IFN-gamma and IL-6 signaling governs neutrophil trafficking and apoptosis during acute inflammation. J. Clin. Investig. 2003, 112, 598–607. [Google Scholar] [CrossRef] [Green Version]
- Rosenbloom, A.J.; Linden, P.K.; Dorrance, A.; Penkosky, N.; Cohen-Melamed, M.H.; Pinsky, M.R. Effect of granulocyte-monocyte colony-stimulating factor therapy on leukocyte function and clearance of serious infection in nonneutropenic patients. Chest 2005, 127, 2139–2150. [Google Scholar] [CrossRef] [Green Version]
- Han, J.; Wang, Y.; Gan, X.; Song, J.; Sun, P.; Dong, X.P. Serum cytokine profiles of children with human enterovirus 71-associated hand, foot, and mouth disease. J. Med. Virol. 2014, 86, 1377–1385. [Google Scholar] [CrossRef]
- Shang, W.; Qian, S.; Fang, L.; Han, Y.; Zheng, C. Association study of inflammatory cytokine and chemokine expression in hand foot and mouth disease. Oncotarget 2017, 8, 79425–79432. [Google Scholar] [CrossRef] [Green Version]
- Zhao, M.Q.; Wang, L.H.; Lian, G.W.; Lin, Z.F.; Li, Y.H.; Guo, M.; Chen, Y.; Liu, X.M.; Zhu, B. Characterization of lymphocyte subsets in peripheral blood cells of children with EV71 infection. J. Microbiol. Immunol. Infect. 2020, 53, 705–714. [Google Scholar] [CrossRef]
- Chen, J.; Tong, J.; Liu, H.; Liu, Y.; Su, Z.; Wang, S.; Shi, Y.; Zheng, D.; Sandoghchian, S.; Geng, J.; et al. Increased frequency of Th17 cells in the peripheral blood of children infected with enterovirus 71. J. Med. Virol. 2012, 84, 763–767. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaki, G.; Umemura, M. Interleukin-17 as an effector molecule of innate and acquired immunity against infections. Microbiol. Immunol. 2007, 51, 1139–1147. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.M.; Lei, H.Y.; Huang, K.J.; Wu, J.M.; Wang, J.R.; Yu, C.K.; Su, I.J.; Liu, C.C. Pathogenesis of enterovirus 71 brainstem encephalitis in pediatric patients: Roles of cytokines and cellular immune activation in patients with pulmonary edema. J. Infect. Dis. 2003, 188, 564–570. [Google Scholar] [CrossRef] [PubMed]
- Fiorentino, D.F.; Bond, M.W.; Mosmann, T.R. Two types of mouse T helper cell. IV. Th2 clones secrete a factor that inhibits cytokine production by Th1 clones. J. Exp. Med. 1989, 170, 2081–2095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamanaka, M.; Kim, S.T.; Wan, Y.Y.; Sutterwala, F.S.; Lara-Tejero, M.; Galán, J.E.; Harhaj, E.; Flavell, R.A. Expression of interleukin-10 in intestinal lymphocytes detected by an interleukin-10 reporter knockin tiger mouse. Immunity 2006, 25, 941–952. [Google Scholar] [CrossRef] [Green Version]
- Moore, K.W.; de Waal Malefyt, R.; Coffman, R.L.; O’Garra, A. Interleukin-10 and the interleukin-10 receptor. Annu. Rev. Immunol. 2001, 19, 683–765. [Google Scholar] [CrossRef]
- Joss, A.; Akdis, M.; Faith, A.; Blaser, K.; Akdis, C.A. IL-10 directly acts on T cells by specifically altering the CD28 co-stimulation pathway. Eur. J. Immunol. 2000, 30, 1683–1690. [Google Scholar] [CrossRef]
- Abbas, A.K.; Murphy, K.M.; Sher, A. Functional diversity of helper T lymphocytes. Nature 1996, 383, 787–793. [Google Scholar] [CrossRef]
- Couper, K.N.; Blount, D.G.; Riley, E.M. IL-10: The master regulator of immunity to infection. J. Immunol. 2008, 180, 5771–5777. [Google Scholar] [CrossRef] [Green Version]
- Jun, J.C.; Jones, M.B.; Oswald, D.M.; Sim, E.S.; Jonnalagadda, A.R.; Kreisman, L.S.C.; Cobb, B.A. T cell-intrinsic TLR2 stimulation promotes IL-10 expression and suppressive activity by CD45RbHi T cells. PLoS ONE 2017, 12, e0180688. [Google Scholar] [CrossRef] [Green Version]
- Sun, G.; Yang, S.; Tao, J.; Zeng, H. Analysis of peripheral blood lymphocyte subpopulations in children with severe and critical hand, foot and mouse disease. Chin. J. Evid. Based Pediatrics 2010, 5, 251–255. [Google Scholar]
- Fan, J.H.; Xu, Z.Y.; Long, C.X.; Xiao, Z.H.; Zhou, X.; Lu, X.L.; Xiong, P.P.; Liu, F. Risk Factors Associated with Death of Childhood Severe Hand-Foot-and-Mouth Disease with Neurogenic Pulmonary Edema. J. Appl. Clin. Pediatrics 2011, 26, 1407–1409. [Google Scholar]
- Yi, Z.; Pei, S.; Suo, W.; Wang, X.; Huang, Z.; Yi, A.; Wang, B.; He, Z.; Wang, R.; Li, Y.; et al. Epidemiological characteristics, routine laboratory diagnosis, clinical signs and risk factors for hand, -foot -and -mouth disease: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0267716. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Literature Number | Author | Time Span | Sample Size | Sex Ratio | Average Age | Pathogen | NOS |
|---|---|---|---|---|---|---|---|
| 1 | Zhang A et al. | 2014.4–2015.3 | 83 | 1.19 | 2.23 | EVA71 | 6 |
| 2 | Zeng M et al. | 2010.7–2010.9 | 40 | 4 | 2.77 | EVA71 | 8 |
| 3 | Wang W et al. | 2012.5–2012.7 | 84 | 1.8 | 2.66 | EVA71 | 5 |
| 4 | Qiu J et al. | 2012.1–2014.12 | 362 | 1.74 | 1.75 | EVA71, CVA16 | 6 |
| 5 | Liu G et al. | 2012.3–2015.7 | 2532 | 2.1 | 2 | EVA71 | 7 |
| 6 | Liu C et al. | 2012.1–2015.12 | 717 | 1.73 | 2.5 | EVA71 | 5 |
| 7 | Li W et al. | 2012.3–2012.10 | 571 | 1.59 | 2.58 | EVA71 | 7 |
| 8 | Li Q et al. | 2018.1–2018.12 | 53 | 3.08 | 2.67 | EVA71 | 7 |
| 9 | Hua Y et al. | 2014–2015 | 52 | 1.6 | 2.8 | EVA71 | 6 |
| 10 | Duan G et al. | 2012.4–2012.11 | 102 | 1.55 | 1.93 | EVA71 | 7 |
| 11 | Dang HX et al. | 2015.6–2016.9 | 89 | NR | 2.32 | EVA71 | 8 |
| 12 | Cai K et al. | 2014.1–2016.12 | 190 | NR | NR | EVA71 | 6 |
| 13 | Cai K et al. | 2014.1–2016.12 | 234 | NR | NR | CVA16 | 6 |
| 14 | Dang H et al. | 2015.6–2018.3 | 111 | 1.27 | 2.5 | EVA71, CVA16 | 7 |
| 15 | He Y et al. | 2012–2014 | 132 | 1.93 | 2.85 | EVA71 | 7 |
| 16 | Li Q et al. | 2017.6–2018.6 | 58 | 3.46 | 2.63 | EVA71 | 7 |
| 17 | Pan J et al. | 2008–2009 | 369 | 1.88 | 4.17 | EVA71, CVA16 | 5 |
| 18 | Song CL et al. | 2010.5–2012.9 | 164 | 1.88 | NR | EVA71, CVA16 | 6 |
| 19 | Xu Y et al. | 2012.4–2013.9 | 107 | 1.49 | 2.33 | EVA71 | 5 |
| 20 | Yang X et al. | 2017.1–2017.12 | 261 | 1.43 | 1.69 | CVA6 | 6 |
| 21 | Zheng G et al. | 2009.1–2016.12 | 179 | 1.67 | 2.04 | EVA71 | 5 |
| 22 | Zhou H et al. | 2008.5–2011.11 | 2379 | 1.39 | 3.2 | EVA71, CVA16 | 6 |
| 23 | Shen Y et al. | 2017.8–2018.3 | 66 | 1.64 | 2.49 | EVA71 | 6 |
| 24 | Yang T et al. | 2010.1–2011.6 | 356 | 1.87 | 2.11 | EVA71 | 6 |
| 25 | Li S et al. | 2011.5–2011.8 | 95 | 1.32 | 2.02 | EVA71 | 6 |
| 26 | Zhu L et al. | 2013.1–2016.1 | 76 | 1.53 | 4.64 | EVA71 | 6 |
| 27 | Zheng W et al. | 2014.7–2015.7 | 70 | 0.79 | 2.18 | EVA71 | 6 |
| 28 | Zhu H et al. | 2018.3 | 39 | 1.29 | 2 | NR | 6 |
| 29 | Han F et al. | 2013.7–2015.7 | 300 | 1.38 | 2.7 | EVA71, CVA16 | 5 |
| 30 | Chen M et al. | 2013.1–2014.6 | 240 | 1.06 | 1.85 | EVA71 | 5 |
| 31 | Sui M et al. | 2013.4–2013.6 | 100 | 1.86 | 1.49 | NR | 6 |
| Clinical Indicators | Number of Literature | Begg’s Test (p Value) |
|---|---|---|
| IL-2 | 4 | 1.000 |
| IL-10 | 4 | 0.734 |
| IL-6 | 5 | 0.806 |
| IL-8 | 3 | 1.000 |
| IFN-γ | 7 | 0.368 |
| TNF-α | 7 | 0.072 |
| WBC | 19 | 0.576 |
| Blood glucose | 9 | 0.466 |
| Lymphocytes | 8 | 0.108 |
| Creatinine | 3 | 1.000 |
| CK-MB | 7 | 1.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xie, Y.; Hu, Q.; Jiang, W.; Ji, W.; Chen, S.; Jin, Y.; Duan, G. Laboratory Indicators for Identifying Hand, Foot, and Mouth Disease Severity: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 1829. https://doi.org/10.3390/vaccines10111829
Xie Y, Hu Q, Jiang W, Ji W, Chen S, Jin Y, Duan G. Laboratory Indicators for Identifying Hand, Foot, and Mouth Disease Severity: A Systematic Review and Meta-Analysis. Vaccines. 2022; 10(11):1829. https://doi.org/10.3390/vaccines10111829
Chicago/Turabian StyleXie, Yaqi, Quanman Hu, Wenjie Jiang, Wangquan Ji, Shuaiyin Chen, Yuefei Jin, and Guangcai Duan. 2022. "Laboratory Indicators for Identifying Hand, Foot, and Mouth Disease Severity: A Systematic Review and Meta-Analysis" Vaccines 10, no. 11: 1829. https://doi.org/10.3390/vaccines10111829