
Antibiotic Recommendations for Treatment of Canine Stromal Corneal Ulcers
by

Milan Joksimovic
1, 
Bradley A. Ford
2,
Tatjana Lazic
1,3,
Ivan Soldatovic
4,
Sergey Luzetsky
3 and
Sinisa Grozdanic
1,3,* 1
Animal Eye Consultants of Iowa, 698 Boyson Road, Hiawatha, IA 52233, USA
2
Department of Pathology, Roy J. and Lucille A. Carver College of Medicine, University of Iowa, Iowa City, IA 52242, USA
3
Oculus–Ophthalmology Specialty Hospital, 11000 Belgrade, Serbia
4
Department of Biostatistics, College of Medicine, University of Belgrade, 11000 Belgrade, Serbia
*
Author to whom correspondence should be addressed.
Vet. Sci. 2023, 10(2), 66; https://doi.org/10.3390/vetsci10020066
Submission received: 28 November 2022
/
Revised: 10 January 2023
/
Accepted: 12 January 2023
/
Published: 17 January 2023
(This article belongs to the Special Issue Antimicrobial Use in Companion Animals)
Abstract
:Simple Summary
Infection of the cornea is among the most frequent causes for the loss of vision in dogs. The purpose of this study was to determine which particular antibiotics can be used immediately at the time of infection to eliminate bacteria from the infected region and prevent the loss of the eye. This study showed that combinations of antibiotics (amikacin and neopolybac or ofloxacin and neopolybac) are potentially the best first choice of treatment to eliminate the majority of commonly isolated bacteria from corneal infections in dogs.
Abstract
The aim of the study was to identify the aerobic bacterial isolates and determine corresponding antibiotic susceptibility profiles in vitro in canine clinical specimens with stromal corneal ulcers, with the goal of providing recommendations for first-line treatment with antibiotics. A total of 198 canine corneal stromal ulcer samples were studied between 2018 and 2021. A corneal swab was collected and cultured under aerobic conditions. Bacterial organisms were identified at the species level by MALDI-TOF mass spectrometry. Antibiotic susceptibility testing for commonly used topical and systemic antibiotics was performed by disk diffusion. Bacterial growth was obtained from 80% of samples. A variety of bacterial species were identified wherein the most common specimens were represented by Staphylococcus pseudintermedius (22%), Staphylococcus epidermidis (12%), Staphylococcus capitis (11%), and Pseudomonas aeruginosa (10%). Based on the overall antibiotic susceptibility data, neopolybac alone (96%) or a combination of neopolybac with either ofloxacin or amikacin (each 99%) showed the best coverage for commonly isolated bacterial organisms from canine corneal stromal ulcers. Results of this study support the use of the combined antibiotics as the first-line response for the treatment of canine corneal stromal ulcers. A statically significant increase in acquired bacterial resistance was detected during the longitudinal data observation.
1. Introduction
The ocular surface is constantly exposed to a variety of environmental stimuli and contains different mechanisms which function as a first level of eye defense against possible pathogens. Bacteria often invade the damaged corneal surface, which in turn may lead to the acceleration of corneal tissue loss, resulting in structural integrity defects and potential loss of the eye [1,2]. The consequences could be vision-threatening and devastating for eye globe integrity if the corneal infection process is not immediately and aggressively treated or the causative bacterial organism is resistant to empiric antibiotic treatment [3]. The first step in treating corneal bacterial infections is empiric therapy based on epidemiological data and use of suggested antimicrobials [4]. While large epidemiological and corneal pathogen surveillance studies have been reported in humans, similar datasets are relatively sparsely reported in veterinary medicine, so the initial selection of the antibiotic treatment is frequently chosen based on personal preference and in-hospital ophthalmic drug availability [4,5,6,7,8,9,10].
A number of studies have evaluated a microbial community in canine corneal ulcers [5,6,7,8,9,10,11,12,13,14,15]. The most frequent bacterial groups identified are Gram-positive staphylococci and streptococci in addition to Gram-negative Pseudomonas aeruginosa [3,5,7,8,9,11,12,13,14,16,17].
The primary purpose of this manuscript was to perform in depth analysis of antimicrobial activity for commonly identified bacteria from canine corneal stromal ulcers and provide general guidelines for the immediate initiation of empiric antibiotic therapy, which may have the highest chance of being effective while waiting for the results of laboratory microbial identification and antibiotic susceptibility. Furthermore, we intended to evaluate trends in the antibiotic resistance development over a four-year period with a goal of providing predictive data for future topical antibiotic use for canine corneal stromal ulcers.
2. Materials and Methods
Canine corneal ulcer samples were harvested using a flocked swab kit and placed in the provided transport media (BD ESwabTM Collection Kit, COPAN ITALIA SpA, Brescia, Italy). All samples were collected 30 s after applying topical anesthetic on the ocular surface by gently rolling over the corneal surface for 10 s (Propracaine 0.05%, Akorn Pharmaceuticals, Lake Forest, IL, USA). The samples were then kept on ice packs until submitted to the laboratory or refrigerated at 4 °C and subsequently cultured after 1 to 5 days of collection.
Bacterial swabs were collected in the period from December 2018 to April 2021 from canine patients with corneal stromal ulcers presented to Animal Eye Consultants of Iowa in the state of Iowa, USA. All patients had a complete eye examination. The inclusion criteria for corneal stromal ulcers were presence of the corneal defect affecting at least 10% of the corneal stromal thickness with the clinical signs of cellular neutrophilic infiltrates with or without evidence of corneal melting. Half of each ESwab tube solution with a collected sample (approximately 0.5 mL) was cultured onto MacConkey agar (Hardy Diagnostics, Santa Maria, CA, USA), while the other half of the sample was cultured onto Chocolate agar (Hardy Diagnostics Hardy Diagnostics, Santa Maria, CA, USA). The plates were incubated at 37 °C in 5% CO2 and examined at 24, 48, and 96 h after plating for bacterial colonies.
Antibiotic susceptibility testing was performed by Kirby–Bauer disc diffusion method in all isolates following Clinical and Laboratory Standards Institute (CLSI) guidelines (https://clsi.org/media/3481/m100ed30_sample.pdf, accessed on 10 January 2023 and https://clsi.org/media/2321/vet08ed4_sample.pdf, accessed on 10 January 2023). An ophthalmology antibiotic panel was developed based on the most frequently used and commercially available topical ophthalmic antibiotics in the midwestern US. Additionally, amoxicillin/clavulanic acid was added to the panel as this antimicrobial is frequently used as a systemic antibiotic after different ophthalmic surgeries. The topical antibiotic set included amikacin (30 µg), bacitracin (10 U), cefazolin (30 µg), cefoxitin (30 µg), gentamicin (10 µg), neomycin (30 µg), ofloxacin (5 µg), oxacillin (1 µg; used instead of cefoxitin in the case of Staphylococcus pseudintermedius and Staphylococcus schleiferi per CLSI guidelines; https://clsi.org/media/2321/vet08ed4_sample.pdf, accessed on 10 January 2023), polymyxin B (300 U), tetracycline (30 µg), and tobramycin (10 µg). The systemic antibiotic set included amoxicillin/clavulanic acid (20/10 µg), cephalexin (30 µg), ciprofloxacin (5 µg), clindamycin (2 µg), doxycycline (30 µg), enrofloxacin (5 µg), marbofloxacin (5 µg), penicillin G (10 U), and sulfamethoxazole/trimethoprim (1.25/23.75 µg). Escherichia coli ATCC 25922 and Staphylococcus aureus ATCC 25923 were the quality control organisms. All antibiotic discs and control cultures were provided by Hardy Diagnostics (Santa Maria, CA, USA) and Microbiologics INC (St Cloud, MN, USA), respectively.
Bacteria were identified to the species level by matrix-assisted laser desorption/ionization-time of flight (MALDI-TOF) analysis following manufacturer’s instructions (Bruker, Madison, WI, USA). Briefly, a single colony no older than 5 days was taken from the culture plate with a toothpick. On the target plate, a thin bacterial layer was smeared onto a single spot and then the same specimen was placed onto the next spot to achieve a thinner bacterial layer. Each sample was covered with 1 µL of 100% formic acid and air dried and then 1 µL of HCCA matrix was added to each spot as instructed by manufacturer. Bacterial Test Standard, Escherichia coli ATCC 25922, Enterococcus faecalis ATCC 29212, and Candida albicans ATCC 10231 were used as quality controls (Microbiologics, INC; St Cloud, MN, USA). MALDI-TOF analysis was performed in a CLIA-certified diagnostic laboratory (Clinical Microbiology Laboratory, University of Iowa Hospitals & Clinics, Iowa City, IA, USA) using the Bruker BioTyper RUO Database which included continuously updated versions of the Compass reference library (in which veterinary isolates are well represented) as well as the optional mycobacterial and fungal libraries.
WHONET database software (World Health Organization) was used with 2022 CLSI breakpoints for dogs. If breakpoints were not available for dogs, other CLSI animal breakpoints were used followed by human CLSI breakpoints if no other animal breakpoints were available. These breakpoints were based on CLSI M100 Performance Standards for Antimicrobial Susceptibility Testing (https://clsi.org/media/3481/m100ed30_sample.pdf, accessed on 10 January 2023), CLSI VET08 Performance Standards for Antimicrobial Disk and Dilution Susceptibility Tests for Bacteria Isolated From Animals (https://clsi.org/media/2321/vet08ed4_sample.pdf, accessed on 10 January 2023), and Hardy Diagnostics Disk Diffusion Zone Diameter Chart (https://www.keyscientific.com/files/Other%20Manufacturers/Hardy%20Diagnostics/AST%20Discs/Hardy%20AST%20Disc%20Insert.pdf, accessed on 10 January 2023). WHONET database software was also used to manage and analyze microbiology laboratory data and antibiotic susceptibility test results. Hardy Diagnostics Disk Diffusion Zone Diameter Chart https://www.keyscientific.com/files/Other%20Manufacturers/Hardy%20Diagnostics/AST%20Discs/Hardy%20AST%20Disc%20Insert.pdf, accessed on 10 January 2023) was also used for polymyxin B breakpoints in Pseudomonas aeruginosa isolates (Resistant ≤ 11; Susceptible ≤ 12).
The AlereTM PBP2A SA Culture Colony Test was performed to detect penicillin-binding protein 2A (PBP2A) in staphylococcal isolates according to manufacturer’s instructions (Alere Scarborough, Inc., 10 Southgate Road, Scarborough, ME 04074, USA). In the case of Staphylococcus pseudintermedius and Staphylococcus schleiferi the methicillin resistance was confirmed with oxacillin disks per CLSI VET08 guidelines (https://clsi.org/media/2321/vet08ed4_sample.pdf, accessed on 10 January 2023).
All bacterial isolates were separated into susceptible and resistant categories according to the interpretive criteria above. Susceptible and intermediate levels of response were assigned to the susceptible class for the purposes of antibiogram creation [5,6,10].
Each antibiotic was classified into the antibiotic categories of aminoglycosides (amikacin, gentamicin, neomycin, and tobramycin), polypeptides/polymyxins (bacitracin, polymyxin B), anti-staphylococcal β-lactams (cephamycins, oxacillin, cefoxitin), tetracyclines (tetracycline), non-extended spectrum cephalosporins (1st and 2nd generation cephalosporins, cefazolin), penicillin and β-lactamase inhibitors (amoxicillin/clavulanic acid), and fluoroquinolones (ofloxacin). Each clinical isolate was classified by group based upon its susceptibility data according to resistance pattern as not multidrug-resistant (Not MDR), multidrug-resistant (MDR), or possible extensively multidrug-resistant (possible XDR). The MDR group was defined as resistance to at least one antibiotic in three or more antibiotic categories. XDR was defined as resistant to at least one antibiotic in all but two or fewer antibiotic categories (i.e., bacterial isolates remain susceptible to only one or two categories) as previously proposed [18,19]. Additionally, intrinsic resistance of an isolate to a particular antibiotic was excluded from this analysis as previously suggested [20].
Statistical analyses were performed using a paired t-test and contingency table analyses (chi-square and Fisher’s exact tests) for the indicated observed parameters with commercial software as described in the manuscript (Prism, version 5.0; GraphPad, San Diego, CA, USA).
3. Results
3.1. Bacterial Growth from Patient Samples
A total of 187 dogs (198 eyes) with corneal stromal ulcers were subjected to sample collection and a total of 198 samples were plated; 159/198 (80.3%) of plated samples demonstrated bacterial growth, while 39/198 (19.7%) yielded no growth. A total of 167 isolates were collected. Regarding prior antibiotic exposure, 134/198 (67.7%) samples were collected from patients having previous antibiotic treatment, while 64/198 (32.3%) samples were collected from patients with no previous antibiotic treatment; 101 of 134 (75.4%) plated samples resulted in the growth of isolates, while 33/134 (24.6%) yielded no growth in the group of patients with previous antibiotic treatment. Regarding patients with no previous antibiotic treatment, 54/64 (84.4%) plated samples returned growth of isolates while 10/64 (15.6%) resulted in no isolate growth.
3.2. Distribution of Bacterial Species in Patients Diagnosed with Corneal Stromal Ulcers
The most common bacterial species identified in the corneal stromal samples was Staphylococcus pseudintermedius present in 22% of samples. Staphylococcus epidermidis, Staphylococcus capitis, and Pseudomonas aeruginosa were present in 12%, 11%, and 10% of samples, respectively. Enteric Gram-negative rods, coagulase negative staphylococci, and Streptococcus canis were present in 7%, 5%, and 5% of samples, respectively (Table 1).
3.3. Antibiotic Susceptibility Pattern of Bacteria Isolated from Corneal Stromal Ulcers
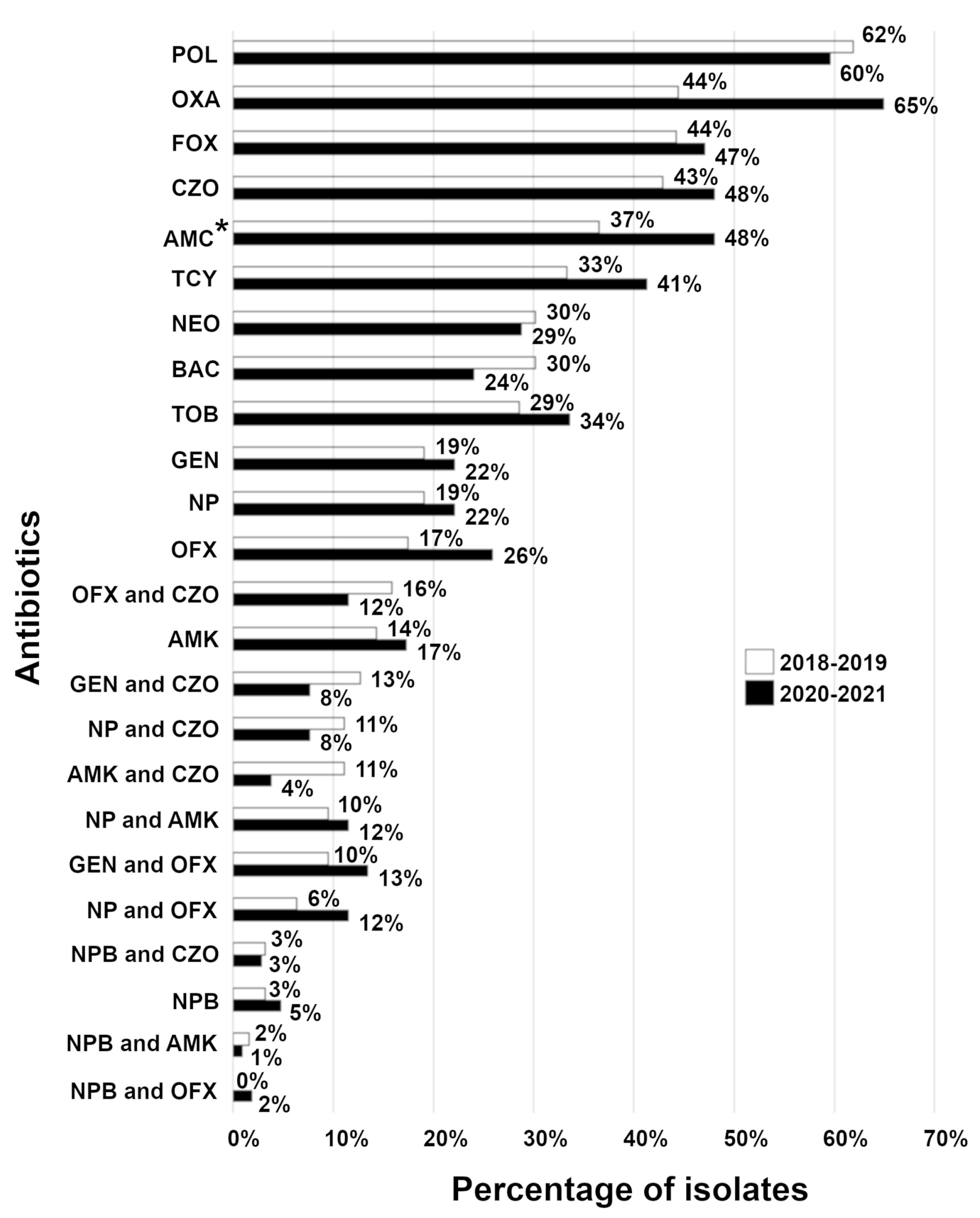
To gain insight into which antibiotics to use in treating current canine corneal stromal ulcers, we analyzed resistance profiles of isolates relative to a single or combination antibiotic between two time points, 2018–2019 and 2020–2021. Based on overall antibiotic susceptibility data, neopolybac alone (96%) or a combination of neopolybac with either ofloxacin or amikacin (each 99%) showed the best antibiotic coverage for commonly isolated bacterial organisms from canine corneal stromal ulcers (Figure 1). No statistically significant difference (p = 0.1637, paired t-test) was observed in bacterial resistance to a single or combination antibiotic between these two time points (Figure 1). For all samples tested with topical antibiotics, bacterial species were most frequently resistant to polymyxin B, oxacillin, cefoxitin, and cefazolin. The least resistance was detected against amikacin, gentamicin, and ofloxacin (Table 2). When acquired resistance was analyzed, a similar trend of resistance was observed (Table 2).
For all samples tested with systemic antibiotics, bacterial species were predominantly resistant to penicillin G (74%), cephalexin (65%), clindamycin (59%), amoxicillin/clavulanic acid (44%), ciprofloxacin (41%), sulfamethoxazole/trimethoprim (41%), and doxycycline (34%), while the least resistance was seen against enrofloxacin (21%), and marbofloxacin (15%).
3.4. Increase in Acquired Resistance in Isolates from Corneal Stromal Ulcers
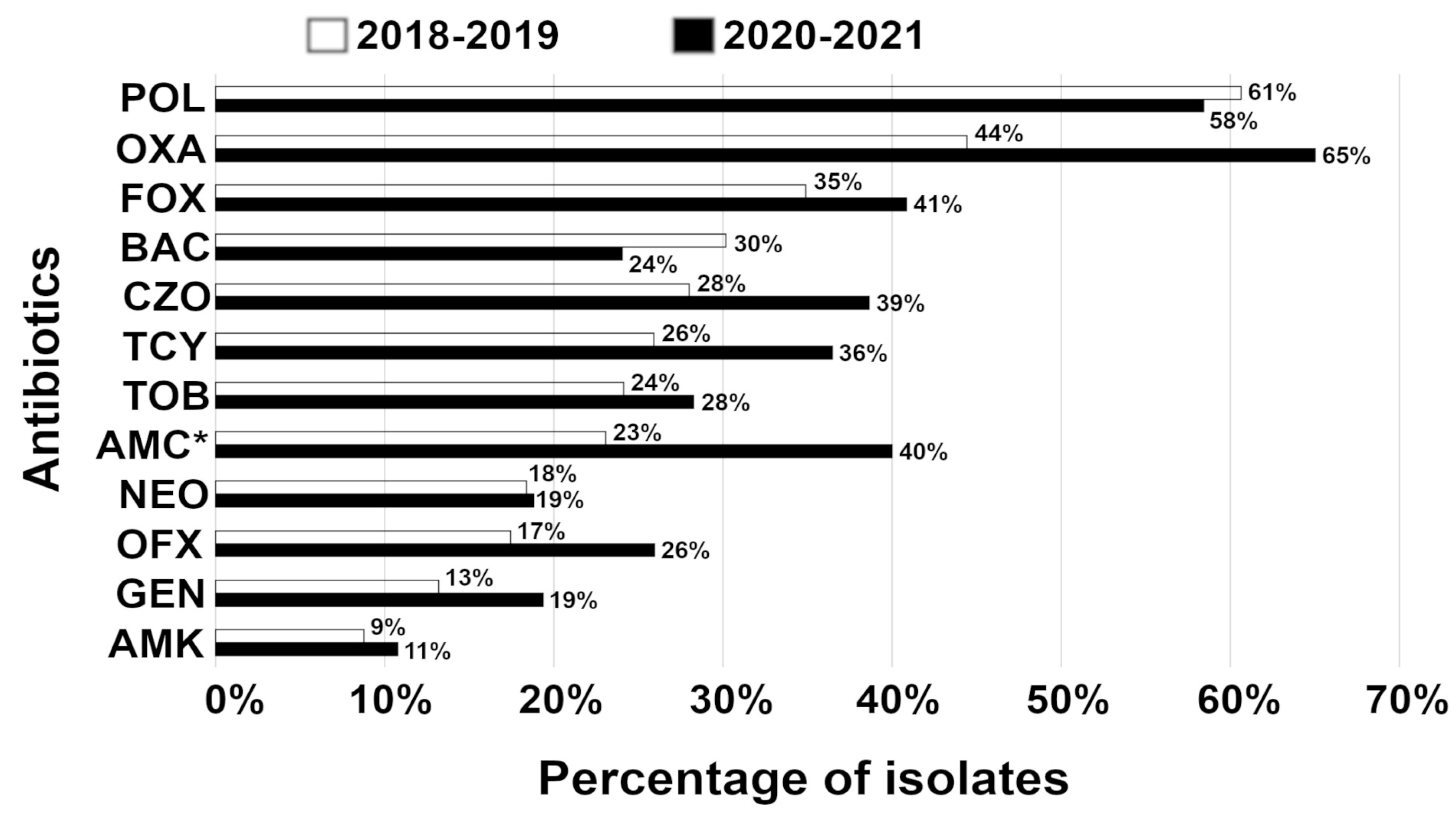
To gain insight into the temporal dynamics of acquired resistance, we analyzed isolates between two time points, 2018–2019 and 2020–2021. In the period 2018–2019, the highest percentage of isolates was resistant to polymyxin B, oxacillin, and cefoxitin with a similar trend in the period 2020–2021 (Figure 2). The lowest percentage of isolates was resistant to amikacin, gentamicin, ofloxacin, and neomycin in the period 2018–2019 with a comparable tendency in the period 2020–2021. Strikingly, a temporal increase in acquired resistance was statistically significant (p = 0.0025, paired t-test) from 2018–2019 to 2020–2021 (Figure 2).
3.5. Distribution of Bacterial Species in Patients Diagnosed with Corneal Stromal Ulcers Relative to Previous Patient’s Antibiotic Treatment
The most common bacterial species identified in the corneal stromal samples relative to the patient’s previous antibiotic treatments were Staphylococcus pseudintermedius, Staphylococcus epidermidis, Staphylococcus capitis, and Pseudomonas aeruginosa (Table 3). When compared to the overall data in Table 1, most of isolates were present in comparable percentages. Accordingly, no statistically significant difference (p = 0.3367, paired t-test) was observed in the distribution of bacterial species relative to the patient’s previous antibiotic treatments.
3.6. Susceptibility Profile of Isolates from Corneal Stromal Ulcers Relative to Patient’s Previous Antibiotic Treatments
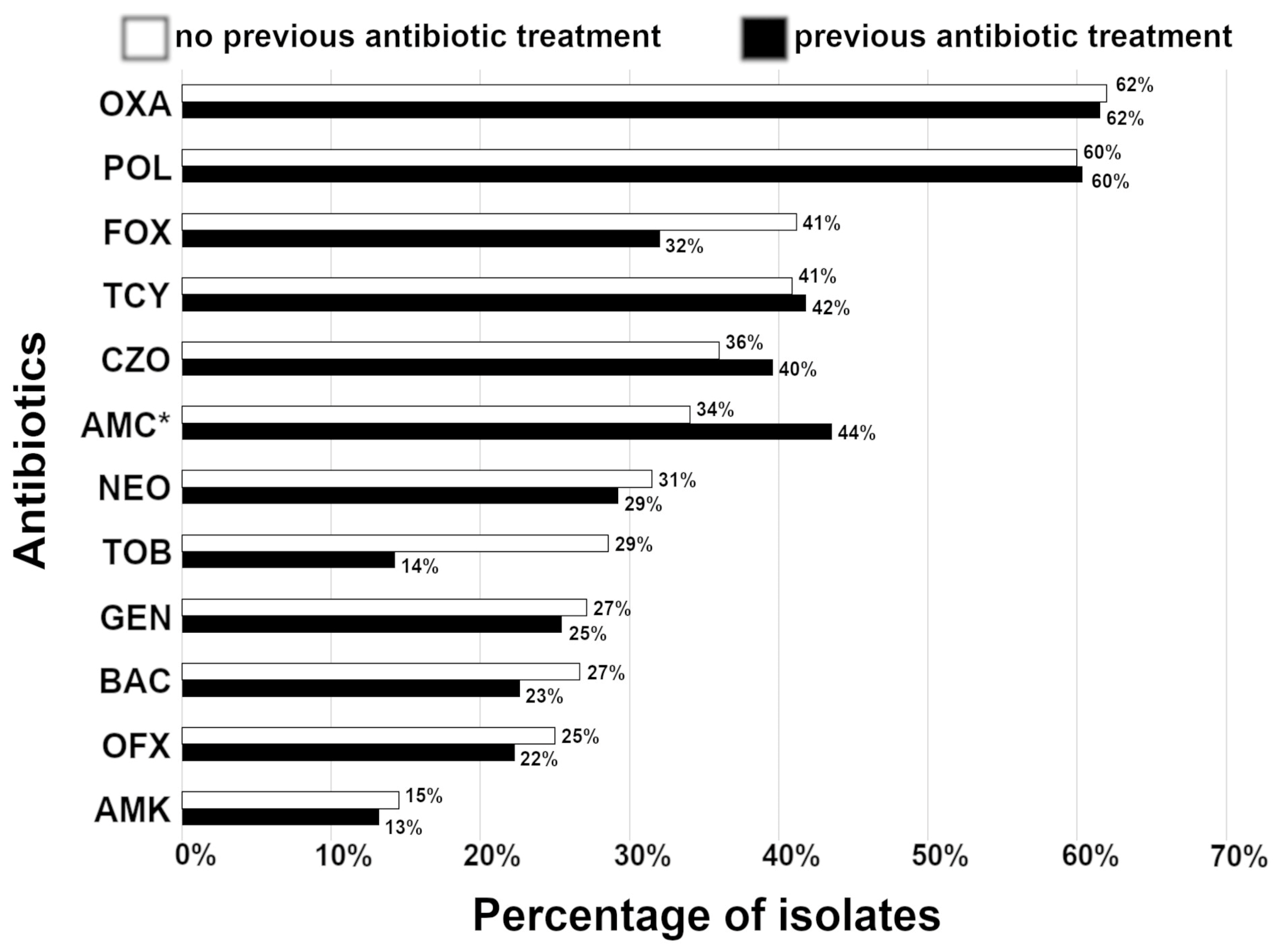
To examine a trend of acquired resistance relative to previous the patient’s antibiotic treatments, we analyzed isolates within an approximately three-year period from 2018 to 2021. In the group with no previous exposure to antibiotics, the highest percentage of isolates was resistant to oxacillin, polymyxin B, cefoxitin, and tetracycline with a similar trend in the group previously treated with antibiotics (Figure 3). The lowest percentage of isolates was resistant to amikacin and ofloxacin in both groups. Furthermore, no statistically significant changes (p = 0.0977, paired t-test) in acquired resistance were observed relative to the patient’s previous antibiotic treatments within the examined three-year period (Figure 3). Furthermore, we analyzed total isolate resistance against the most commonly prescribed antibiotics by local non-specialty veterinary practices, ofloxacin and tobramycin, relative to the patient’s previous antibiotic treatments. In either case, no statistically significant changes in resistance were observed relative to previous patient’s antibiotic treatments (ofloxacin; odds ratio = 1.744; CI= 0.3717–8.647, p = 0.7163; tobramycin (odds ratio = 0.2857; CI = 0.05942–1.240, p = 0.1919; contingency table analyses (chi-square and Fisher’s exact tests)).
3.7. Resistance Profile Based on the Percentage of Isolates Resistant to Multiple Antibiotics in Canine Corneal Stromal Ulcers
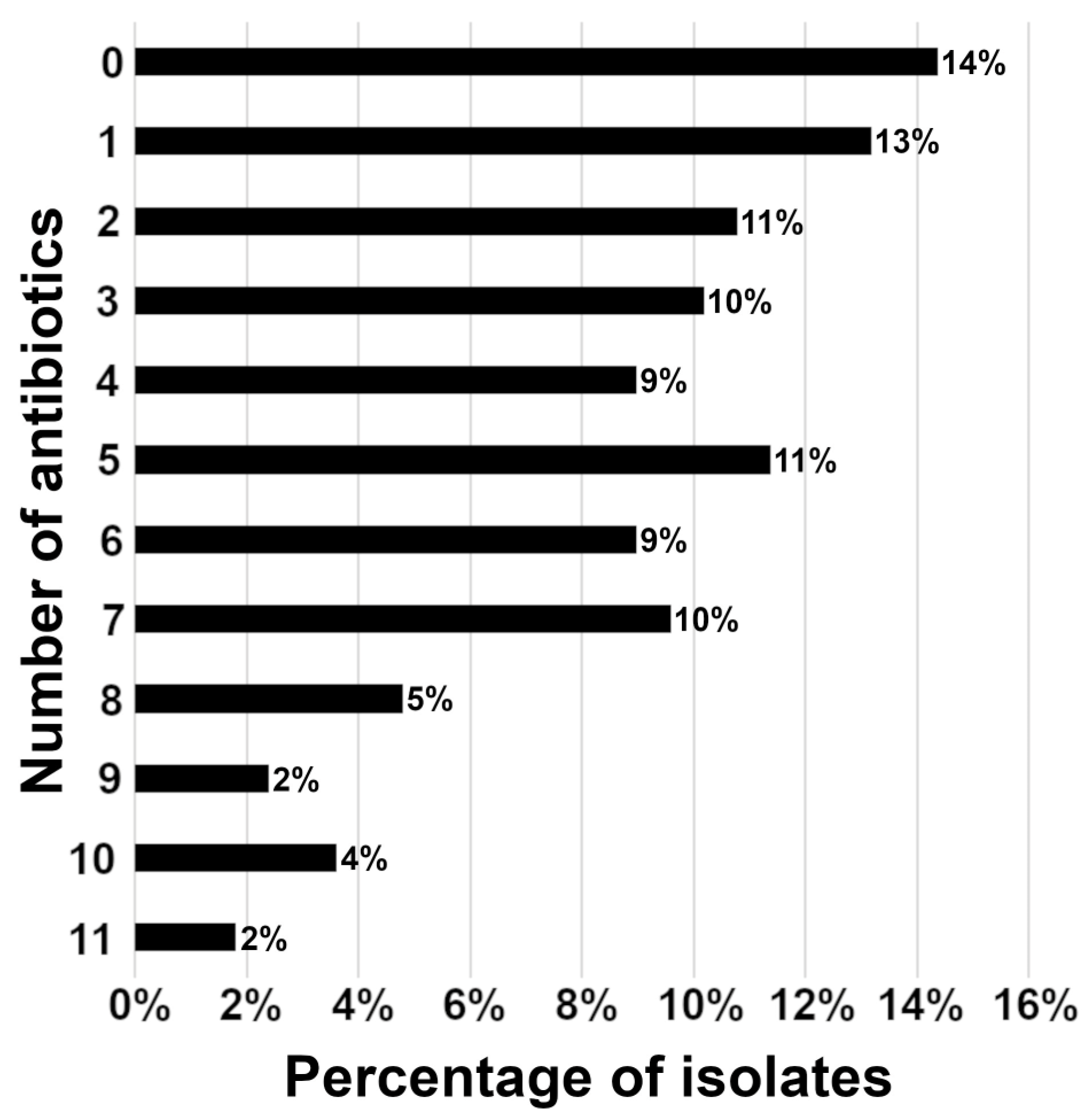
The highest percentage of bacteria was not resistant to any tested antibiotic (24/167; 14%) followed by bacteria resistant to one antibiotic (22/167; 13%), while the vast majority of isolates (73%) were resistant to two or more tested antibiotics (Figure 4). Furthermore, no statistically significant difference (p = 0.1855, paired t-test) was observed in the percentage of isolates resistant to multiple antibiotics relative to the patient’s previous antibiotic treatments. Some highly aggressive isolates showed antibiotic resistance to nine or more tested antibiotics (Figure 4), such as a particular case of Staphylococcus pseudintermedius (Figure 5).
3.8. Distribution of Multidrug-Resistant (MDR) Bacteria in Clinical Corneal Ulcers
Overall, in the corneal stromal ulcer samples, 62% (103/167) were not MDR isolates, 20% (33/167) were MDR isolates, while 18% (31/167) were possible XDR isolates from 2018–2021. Regarding the patient’s previous antibiotic treatments, no statistically significant difference (p = 0.4325, paired t-test) was observed in the distribution of multidrug-resistant bacteria. In the period 2018–2019, 67% (42/63) were not MDR isolates and 19% (12/63) were MDR isolates, while 14% (9/63) were possible XDR isolates. In the period 2020–2021, 59% (61/104) were not MDR isolates and 20% (21/104) were MDR isolates, while 21% (22/104) were possible XDR isolates. Moreover, no statistically significant difference (p = 0.2777, paired t-test) was observed in multidrug resistance between these two time points.
3.9. Methicillin-Resistant Staphylococcus spp.
To assess methicillin resistance in Staphylococcus species, the isolates were tested with cefoxitin disks [21]. A few species were also tested with the penicillin-binding protein 2A (PBP2A) antibody test. Overall, in the 2018–2021 period, 49% (40/81) of isolates were methicillin-resistant. Relative to the patient’s previous antibiotic treatments, similar percentages of resistance were detected. In the group with no previous antibiotic treatment, 54% (15/28) of isolates were methicillin resistant. In the group with previous antibiotic treatment 47% (25/53) of isolates were methicillin resistant. Over time, a substantial increase in the number of methicillin-resistant Staphylococcus species were detected from 2018–2019 (39%; 11/28) to 2020–2021 (55%; 29/53).
4. Discussion
In this study, the overall bacterial growth from patients with corneal stromal ulcers (80.3%) was generally higher than previously reported rates (57–71%) [5,7,8,10,13,22,23]. The higher positive culture rate in our study may reflect the use of improved elution swabs (BD ESwabTM Collection Kit) and possibly be due to increased yield of plating half of the volume of each collection swab onto a culture plate rather than a subset of the total volume adsorbed onto the swab.
The most common bacterial isolates from the stromal corneal ulcers in our study were Staphylococcus spp. accounting for 50% of all bacterial species, consistent with or slightly above levels reported in previous studies that were performed in various geographical locations (Table 4) [5,6,8,9,11,13,15,22,24,25,26]. In contrast, studies from Australia and UK reported Pseudomonas aeruginosa and Streptococcus spp. as the most commonly isolated bacteria from canine ulcers (Table 4) [7,10]. This discrepancy could be potentially explained by regional differences of bacterial species in various geographical locations due to local climate factors [4,9], wherein weather conditions in the midwestern US are not as warm and humid as in the southeastern US, Brazil, or Australia (Table 4).
Based on the overall antibiotic susceptibility data, neopolybac alone (96%) or a combination of neopolybac with either ofloxacin or amikacin showed the best coverage for commonly isolated bacterial organisms from canine corneal stromal ulcers in line with a previous report [15]. Considering that canine stromal corneal ulcers may be extremely aggressive, an immediate and aggressive initiation of antibiotic therapy with commercially available ophthalmic antibiotics (neopolybac and ofloxacin) may be the prudent strategy while waiting for the results of the microbial identification and susceptibility from the affected patient.
Data from this study described a trend of increased resistance to polymyxin B and ofloxacin when compared to previous studies [5,10,12]. However, a comparison of data from this study to the recent report [15], both performed at the same general geographical location (midwestern US), revealed substantial differences in topical susceptibility profiles for polymyxin B, bacitracin, and cefazolin (Table 5). This discrepancy can be partly explained by different methods used in these two studies (Kirby–Bauer disc diffusion method vs. minimum inhibitory concentration (MIC) susceptibility testing). Since the reliability of bacterial resistance to polymyxin B assessed by the Kirby–Bauer disc diffusion method is still questionable [27,28], reported polymyxin B data should be carefully scrutinized when making the clinical judgement on the choice of antibiotic. The same logic can be applied for bacitracin as this antibiotic, together with polymyxin B, belongs to the same antibiotic group of polypeptides. The trend of increased resistance to ofloxacin may reflect the acquisition of mutations through mobile genetic elements as reported in the case of Pseudomonas aeruginosa [29].
In our study, a patient’s previous antibiotic treatments do not affect isolate resistance to tobramycin in general. However, resistance to tobramycin appears to be increased between two time points, in line with a previous report performed at the same general geographical location [15] (Table 5; midwestern US). In contrast, the other study performed in the southeastern US demonstrated a substantially higher increase in and the percentage of resistant isolates to tobramycin [6]. As previously discussed, this inconsistency could be due to local climate factors in conjunction with the regional variation of bacterial species [4,9].
In the cases where severe corneal neovascularization is present or conjunctival pedicle graft surgery was performed so iatrogenic blood supply can be provided to the corneal ulcer region, treatments with topical medications can be complemented by systemic antibiotics. Based on data reported in this study, a systemic fluoroquinolone antibiotic (marbofloxacin, enrofloxacin) should be the first choice for treatment of corneal stromal ulcers, which is in line with a recently published report from the US Midwest on corneal ulcers [15]. In comparison to the earlier report from the southeastern US [6], in this study there was a tendency of increased resistance to enrofloxacin and ciprofloxacin, although this difference may be caused by regional differences in a distribution of bacterial species at different geographical locations and local climate factors [4,9].
In this study, we report a statistically significant increase in acquired resistance in isolates from 2018–2019 to 2020–2021. Our data not only point to this alarming trend but also indicate a presence of detectable deteriorating changes in antimicrobial susceptibility within a relatively short three-year period. However, the presence or absence of previous antibiotic treatments does not appear to influence an overall status of acquired bacterial resistance.
In our study, we detected 8% of isolates which showed antibiotic resistance to nine or more tested antibiotics. This pattern is of particular concern and qualifies corresponding isolates as potentially very aggressive pathogens causing corneal pathology poorly responsive to medical and surgical treatments.
The surge in antibiotic resistance is an alarming concern not only in global health care but also in animal ophthalmology [30]. In this study, over a third of isolates from clinical corneal stromal ulcers belong to the MDR group. However, none of Pseudomonas aeruginosa specimens belong to the MDR class, consistent with a previous report [15]. This study did not detect a statistically significant MDR increase between two time points 2018–2019 and 2020–2021 in contrast to the previous report, suggesting an MDR increase over time period of 2016–2020 [15].
Methicillin resistance of Staphylococcus spp. isolates is a serious concern in human and veterinary medicine due to the cross-species infectious behavior of these bacteria [31,32]. In this study, a half of Staphylococcus spp. isolates were methicillin resistant, which is in line with a previous report [33] with some isolates showing extremely aggressive clinical behavior (Figure 5).
In conclusion, the current study reports four important findings directly relevant to antibiotic treatments of canine corneal stromal ulcers: (1) clinical corneal stromal isolates showed increased acquired resistance within a three-year period; (2) many isolates were resistant to a large number of antibiotics; (3) over a third of analyzed specimens belong to the multidrug resistance group; and (4) some clinical isolates showed resistance to a combination of up to four antibiotics. Similar data have been recently reported in the ARMOR study from human corneal isolates; however, analysis of the resistance trend did not show gradual progression over a period of 10 years [4].
Analogous to earlier studies of antibiotic susceptibility in animals, key limitations of this study are the fact that CLSI interpretive criteria and breakpoints for particular bacterial species and antibiotic combinations are based on systemic minimum inhibitory concentration of antibiotics, since specific standards for corneal infections were never developed in human or veterinary medicine. Consequently, complete reliability of the Kirby–Bauer disc diffusion system as a method to assess corneal infections can be fully evaluated when these standards are developed. Until specific ophthalmology antibiotic standards become available, this study may provide a general guideline when initially choosing empirical therapies for treating canine corneal stromal ulcers while waiting for the patient-specific antibiotic susceptibility profile.
5. Conclusions
The results of this study support the use of the combined antibiotics as the first-line response for the treatment of canine corneal stromal ulcers. Neopolybac alone or a combination of neopolybac with either ofloxacin or amikacin is recommended as the initial antibiotic treatment while waiting for the patient-specific antibiotic susceptibility profile.
Author Contributions
Conceptualization: M.J. and S.G. Methodology: M.J., B.A.F., I.S., S.L. and S.G. Validation: M.J., B.A.F., T.L., I.S., S.L. and S.G. Formal analysis: M.J., I.S. and S.G. Investigation: M.J., T.L. and S.G. Resources: B.A.F., T.L., I.S. and S.G. Writing—original draft preparation: M.J. and S.G. Writing—review and editing: M.J., B.A.F., T.L., I.S., S.L. and S.G. Visualization: M.J., I.S. and S.G. Supervision: S.G. Project administration: M.J. and S.G. Funding acquisition: T.L. and S.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Animal Eye Consultants of Iowa Hospital Board. The study is performed as a retrospective study with analysis of database data without client animal identifiers, so IACUC protocol was not required.
Informed Consent Statement
An informed consent was provided to the owners prior to collecting samples.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy concerns (client identification information).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rogers, C.M.; Scott, E.M.; Sarawichitr, B.; Arnold, C.; Suchodolski, J.S. Evaluation of the bacterial ocular surface microbiome in ophthalmologically normal dogs prior to and following treatment with topical neomycin-polymyxin-bacitracin. PLoS ONE 2020, 15, e0234313. [Google Scholar] [CrossRef]
- Leis, M.L.; Costa, M.O. Initial description of the core ocular surface microbiome in dogs: Bacterial community diversity and composition in a defined canine population. Vet. Ophthalmol. 2019, 22, 337–344. [Google Scholar] [CrossRef]
- Ledbetter, E.C.; Franklin-Guild, R.J.; Edelmann, M.L. Capnocytophaga keratitis in dogs: Clinical, histopathologic, and microbiologic features of seven cases. Vet. Ophthalmol. 2018, 21, 638–645. [Google Scholar] [CrossRef]
- Asbell, P.A.; Sanfilippo, C.M.; Sahm, D.F.; DeCory, H.H. Trends in Antibiotic Resistance Among Ocular Microorganisms in the United States From 2009 to 2018. JAMA Ophthalmol. 2020, 138, 439–450. [Google Scholar] [CrossRef] [Green Version]
- McKeever, J.M.; Ward, D.A.; Hendrix, D.V.H. Comparison of antimicrobial resistance patterns in dogs with bacterial keratitis presented to a veterinary teaching hospital over two multi-year time periods (1993–2003 and 2013–2019) in the Southeastern United States. Vet. Ophthalmol. 2021, 24, 653–658. [Google Scholar] [CrossRef]
- Tolar, E.L.; Hendrix, D.V.; Rohrbach, B.W.; Plummer, C.E.; Brooks, D.E.; Gelatt, K.N. Evaluation of clinical characteristics and bacterial isolates in dogs with bacterial keratitis: 97 cases (1993–2003). J. Am. Vet. Med. Assoc. 2006, 228, 80–85. [Google Scholar] [CrossRef]
- Hindley, K.E.; Groth, A.D.; King, M.; Graham, K.; Billson, F.M. Bacterial isolates, antimicrobial susceptibility, and clinical characteristics of bacterial keratitis in dogs presenting to referral practice in Australia. Vet. Ophthalmol. 2016, 19, 418–426. [Google Scholar] [CrossRef]
- Suter, A.; Voelter, K.; Hartnack, S.; Spiess, B.M.; Pot, S.A. Septic keratitis in dogs, cats, and horses in Switzerland: Associated bacteria and antibiotic susceptibility. Vet. Ophthalmol. 2018, 21, 66–75. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Pan, Q.; Zhang, L.; Xue, Q.; Cui, J.; Qi, C. Investigation of bacterial microorganisms in the conjunctival sac of clinically normal dogs and dogs with ulcerative keratitis in Beijing, China. Vet. Ophthalmol. 2008, 11, 145–149. [Google Scholar] [CrossRef]
- Tsvetanova, A.; Powell, R.M.; Tsvetanov, K.A.; Smith, K.M.; Gould, D.J. Melting corneal ulcers (keratomalacia) in dogs: A 5-year clinical and microbiological study (2014–2018). Vet. Ophthalmol. 2021, 24, 265–278. [Google Scholar] [CrossRef]
- Ekapopphan, D.; Srisutthakarn, A.; Moonarmart, W.; Buddhirongawatr, R.; Bangphoomi, N. Identification and antimicrobial susceptibility of microorganisms isolated from severe corneal ulcers of dogs in Thailand. J. Vet. Med. Sci. 2018, 80, 1259–1265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jinks, M.R.; Miller, E.J.; Diaz-Campos, D.; Mollenkopf, D.F.; Newbold, G.; Gemensky-Metzler, A.; Chandler, H.L. Using minimum inhibitory concentration values of common topical antibiotics to investigate emerging antibiotic resistance: A retrospective study of 134 dogs and 20 horses with ulcerative keratitis. Vet. Ophthalmol. 2020, 23, 806–813. [Google Scholar] [CrossRef] [PubMed]
- Ledbetter, E.C.; Hendricks, L.M.; Riis, R.C.; Scarlett, J.M. In vitro fluoroquinolone susceptibility of Pseudomonas aeruginosa isolates from dogs with ulcerative keratitis. Am. J. Vet. Res. 2007, 68, 638–642. [Google Scholar] [CrossRef] [PubMed]
- LoPinto, A.J.; Mohammed, H.O.; Ledbetter, E.C. Prevalence and risk factors for isolation of methicillin-resistant Staphylococcus in dogs with keratitis. Vet. Ophthalmol. 2015, 18, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, J.S.; Allbaugh, R.A.; Kenne, D.E.; Sebbag, L. Prevalence and Antibiotic Susceptibility of Bacterial Isolates From Dogs With Ulcerative Keratitis in Midwestern United States. Front. Vet. Sci. 2020, 7, 583965. [Google Scholar] [CrossRef]
- Ledbetter, E.C.; Mun, J.J.; Kowbel, D.; Fleiszig, S.M. Pathogenic phenotype and genotype of Pseudomonas aeruginosa isolates from spontaneous canine ocular infections. Investig. Ophthalmol. Vis. Sci. 2009, 50, 729–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leigue, L.; Montiani-Ferreira, F.; Moore, B.A. Antimicrobial susceptibility and minimal inhibitory concentration of Pseudomonas aeruginosa isolated from septic ocular surface disease in different animal species. Open Vet. J. 2016, 6, 215–222. [Google Scholar] [CrossRef] [Green Version]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2012, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, S.; Silley, P.; Simjee, S.; Woodford, N.; van Duijkeren, E.; Johnson, A.P.; Gaastra, W. Editorial: Assessing the antimicrobial susceptibility of bacteria obtained from animals. J. Antimicrob. Chemother. 2010, 65, 601–604. [Google Scholar] [CrossRef]
- Sweeney, M.T.; Lubbers, B.V.; Schwarz, S.; Watts, J.L. Applying definitions for multidrug resistance, extensive drug resistance and pandrug resistance to clinically significant livestock and companion animal bacterial pathogens. J. Antimicrob. Chemother. 2018, 73, 1460–1463. [Google Scholar] [CrossRef]
- Bonjean, M.; Hodille, E.; Dumitrescu, O.; Dupieux, C.; Nkoud Mongo, C.; Allam, C.; Beghin, M.; Paris, M.; Borrel, O.; Chardon, H.; et al. Disk Diffusion Testing for Detection of Methicillin-Resistant Staphylococci: Does Moxalactam Improve upon Cefoxitin? J. Clin. Microbiol. 2016, 54, 2905–2909. [Google Scholar] [CrossRef] [Green Version]
- Auten, C.R.; Urbanz, J.L.; Dees, D.D. Comparison of bacterial culture results collected via direct corneal ulcer vs conjunctival fornix sampling in canine eyes with presumed bacterial ulcerative keratitis. Vet. Ophthalmol. 2020, 23, 135–140. [Google Scholar] [CrossRef]
- Gerding, P.A., Jr.; McLaughlin, S.A.; Troop, M.W. Pathogenic bacteria and fungi associated with external ocular diseases in dogs: 131 cases (1981–1986). J. Am. Vet. Med. Assoc. 1988, 193, 242–244. [Google Scholar]
- Prado, M.R.; Rocha, M.F.; Brito, E.H.; Girão, M.D.; Monteiro, A.J.; Teixeira, M.F.; Sidrim, J.J. Survey of bacterial microorganisms in the conjunctival sac of clinically normal dogs and dogs with ulcerative keratitis in Fortaleza, Ceará, Brazil. Vet. Ophthalmol. 2005, 8, 33–37. [Google Scholar] [CrossRef]
- Lin, C.T.; Petersen-Jones, S.M. Antibiotic susceptibility of bacterial isolates from corneal ulcers of dogs in Taiwan. J. Small Anim. Pract. 2007, 48, 271–274. [Google Scholar] [CrossRef]
- Varges, R.; Penna, B.; Martins, G.; Martins, R.; Lilenbaum, W. Antimicrobial susceptibility of Staphylococci isolated from naturally occurring canine external ocular diseases. Vet. Ophthalmol. 2009, 12, 216–220. [Google Scholar] [CrossRef]
- Behera, B.; Mathur, P.; Das, A.; Kapil, A.; Gupta, B.; Bhoi, S.; Farooque, K.; Sharma, V.; Misra, M.C. Evaluation of susceptibility testing methods for polymyxin. Int. J. Infect. Dis. 2010, 14, e596–e601. [Google Scholar] [CrossRef] [Green Version]
- Jerke, K.H.; Lee, M.J.; Humphries, R.M. Polymyxin Susceptibility Testing: A Cold Case Reopened. Clin. Microbiol. Newsl. 2016, 38, 69–77. [Google Scholar] [CrossRef]
- Khan, M.; Summers, S.; Rice, S.A.; Stapleton, F.; Willcox, M.D.P.; Subedi, D. Acquired fluoroquinolone resistance genes in corneal isolates of Pseudomonas aeruginosa. Infect. Genet. Evol. J. Mol. Epidemiol. Evol. Genet. Infect. Dis. 2020, 85, 104574. [Google Scholar] [CrossRef]
- Soimala, T.; Lubke-Becker, A.; Hanke, D.; Eichhorn, I.; Fessler, A.T.; Schwarz, S.; Eule, J.C. Molecular and phenotypic characterization of methicillin-resistant Staphylococcus pseudintermedius from ocular surfaces of dogs and cats suffering from ophthalmological diseases. Vet. Microbiol. 2020, 244, 108687. [Google Scholar] [CrossRef]
- Rich, M. Staphylococci in animals: Prevalence, identification and antimicrobial susceptibility, with an emphasis on methicillin-resistant Staphylococcus aureus. Br. J. Biomed. Sci. 2005, 62, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Malik, S.; Peng, H.; Barton, M.D. Antibiotic resistance in staphylococci associated with cats and dogs. J. Appl. Microbiol. 2005, 99, 1283–1293. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.D.; Kania, S.A.; Rohrbach, B.W.; Frank, L.A.; Bemis, D.A. Prevalence of oxacillin- and multidrug-resistant staphylococci in clinical samples from dogs: 1,772 samples (2001–2005). J. Am. Vet. Med. Assoc. 2007, 230, 221–227. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Percentage of total resistant isolates to a single or combination antibiotics from 2018–2019 and 2020–2021. Percentage (%) of overall resistant bacterial species isolated from patients with corneal stromal ulcers (combined intrinsic and acquired resistance). For the period 2018–2019, the number of isolates is 63 for each antibiotic/antibiotic combination except for oxacillin, which numbered 9. For the period 2020–2021, the number of isolates is 104 for each antibiotic/antibiotic combination except for oxacillin, which numbered 20. * = although amoxicillin/clavulanic acid is not used topically, data for this antibiotic are presented here since it is often used postoperatively as a systemic antibiotic. Abbreviations: AMC, amoxicillin/clavulanic acid; AMK, amikacin; BAC, bacitracin; CZO, cefazolin; FOX, cefoxitin; GEN, gentamicin; NEO, neomycin; NP, neomycin and polymyxin B; NPB, neomycin, polymyxin B, and bacitracin; OFX, ofloxacin; OXA, oxacillin; POL, polymyxin B; TCY, tetracycline; TOB, tobramycin.
Figure 1.
Percentage of total resistant isolates to a single or combination antibiotics from 2018–2019 and 2020–2021. Percentage (%) of overall resistant bacterial species isolated from patients with corneal stromal ulcers (combined intrinsic and acquired resistance). For the period 2018–2019, the number of isolates is 63 for each antibiotic/antibiotic combination except for oxacillin, which numbered 9. For the period 2020–2021, the number of isolates is 104 for each antibiotic/antibiotic combination except for oxacillin, which numbered 20. * = although amoxicillin/clavulanic acid is not used topically, data for this antibiotic are presented here since it is often used postoperatively as a systemic antibiotic. Abbreviations: AMC, amoxicillin/clavulanic acid; AMK, amikacin; BAC, bacitracin; CZO, cefazolin; FOX, cefoxitin; GEN, gentamicin; NEO, neomycin; NP, neomycin and polymyxin B; NPB, neomycin, polymyxin B, and bacitracin; OFX, ofloxacin; OXA, oxacillin; POL, polymyxin B; TCY, tetracycline; TOB, tobramycin.

Figure 2.
Increase in acquired resistance in isolates from corneal stromal ulcers between 2018–2019 and 2020–2021. Percentage (%) of resistant bacterial species from patient samples excluding intrinsic resistance of isolates. The number of isolates ranges from 9 to 63 for the period 2018–2019 and from 20 to 104 for the period 2020–2021. * = although amoxicillin/clavulanic acid is not used topically, data for this antibiotic are presented here since it is often used postoperatively as a systemic antibiotic. Abbreviations: AMC, amoxicillin/clavulanic acid; AMK, amikacin; BAC, bacitracin; CZO, cefazolin; FOX, cefoxitin; GEN, gentamicin; NEO, neomycin; OFX, ofloxacin; OXA, oxacillin; POL, polymyxin B; TCY, tetracycline; TOB, tobramycin.
Figure 2.
Increase in acquired resistance in isolates from corneal stromal ulcers between 2018–2019 and 2020–2021. Percentage (%) of resistant bacterial species from patient samples excluding intrinsic resistance of isolates. The number of isolates ranges from 9 to 63 for the period 2018–2019 and from 20 to 104 for the period 2020–2021. * = although amoxicillin/clavulanic acid is not used topically, data for this antibiotic are presented here since it is often used postoperatively as a systemic antibiotic. Abbreviations: AMC, amoxicillin/clavulanic acid; AMK, amikacin; BAC, bacitracin; CZO, cefazolin; FOX, cefoxitin; GEN, gentamicin; NEO, neomycin; OFX, ofloxacin; OXA, oxacillin; POL, polymyxin B; TCY, tetracycline; TOB, tobramycin.

Figure 3.
Acquired resistance in isolates from corneal stromal ulcers regarding the patient’s previous antibiotic treatments. Percentage (%) of resistant bacterial species against antibiotics excluding intrinsic resistance of isolates. The number of isolates range from 16 to 60 for the patients without previous antibiotic treatments and from 13 to 106 for the patients with previous antibiotic treatments. * = although amoxicillin/clavulanic acid is not used topically, data for this antibiotic are presented here since it is often used postoperatively as a systemic antibiotic. Abbreviations: AMC, amoxicillin/clavulanic acid; AMK, amikacin; BAC, bacitracin; CZO, cefazolin; FOX, cefoxitin; GEN, gentamicin; NEO, neomycin; OFX, ofloxacin; OXA, oxacillin; POL, polymyxin B; TCY, tetracycline; TOB, tobramycin.
Figure 3.
Acquired resistance in isolates from corneal stromal ulcers regarding the patient’s previous antibiotic treatments. Percentage (%) of resistant bacterial species against antibiotics excluding intrinsic resistance of isolates. The number of isolates range from 16 to 60 for the patients without previous antibiotic treatments and from 13 to 106 for the patients with previous antibiotic treatments. * = although amoxicillin/clavulanic acid is not used topically, data for this antibiotic are presented here since it is often used postoperatively as a systemic antibiotic. Abbreviations: AMC, amoxicillin/clavulanic acid; AMK, amikacin; BAC, bacitracin; CZO, cefazolin; FOX, cefoxitin; GEN, gentamicin; NEO, neomycin; OFX, ofloxacin; OXA, oxacillin; POL, polymyxin B; TCY, tetracycline; TOB, tobramycin.

Figure 4.
Distribution of resistant isolates against multiple antibiotics. Percentage of the isolates that are resistant to the corresponding number of antibiotics. Bacterial samples were isolated from canine corneal stromal ulcers (number of isolates = 167).
Figure 4.
Distribution of resistant isolates against multiple antibiotics. Percentage of the isolates that are resistant to the corresponding number of antibiotics. Bacterial samples were isolated from canine corneal stromal ulcers (number of isolates = 167).

Figure 5.
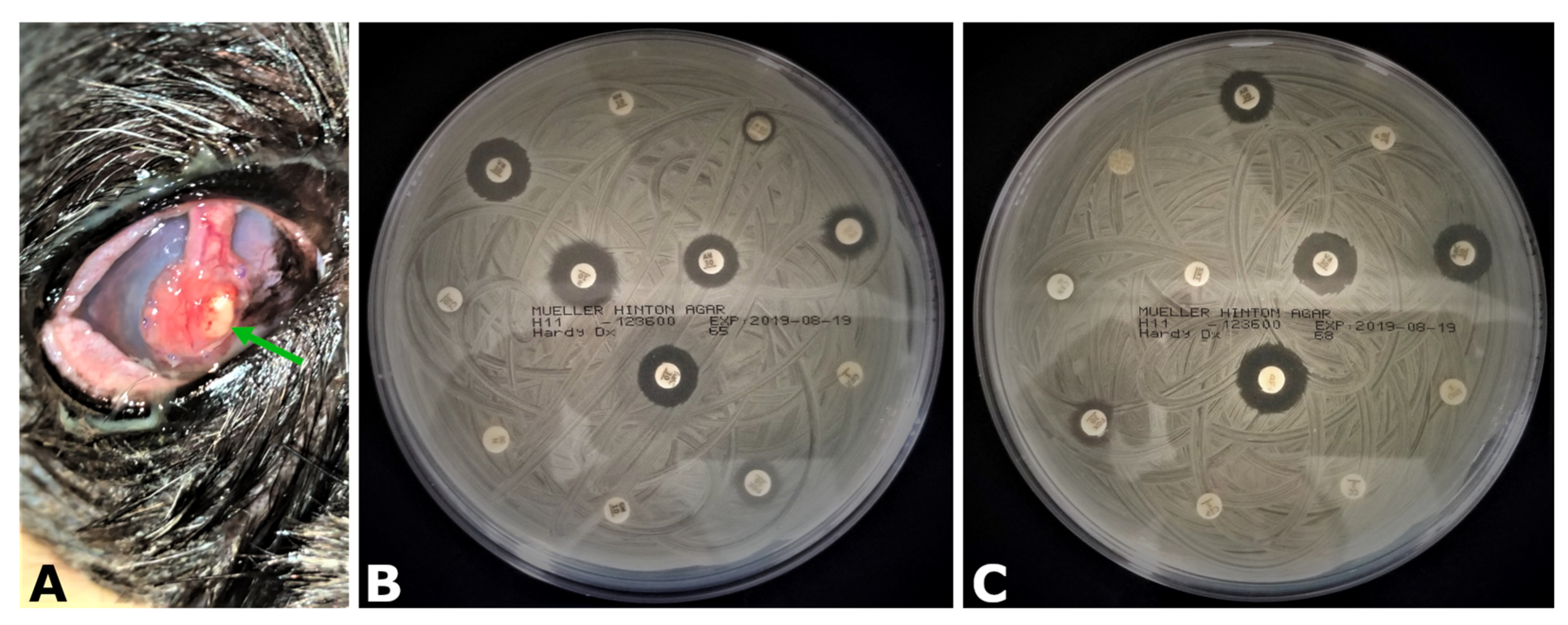
Aggressive corneal infection by Staphylococcus pseudintermedius. (A) Patient cornea was severely affected with a focal zone of conjunctival graft destruction at 4 o’clock position in the paracentral graft region (green arrow). Patient was treated with topical ofloxacin and cefazolin and systemic amoxicillin/clavulanic acid immediately after surgery. (B,C) Antibiotic susceptibility testing performed for topical (A) and systemic antibiotic sets (B). The isolate was resistant to the multiple topical (amikacin, cefazolin, cefoxitin, gentamicin, neomycin, ofloxacin, polymyxin B, tetracycline, and tobramycin) and systemic antibiotics (amoxicillin/clavulanic acid, cephalexin, ciprofloxacin, clindamycin, doxycycline, enrofloxacin, marbofloxacin, penicillin G, and sulfamethoxazole/trimethoprim). The isolate was also penicillin-binding protein 2A–positive and susceptible only to topical bacitracin.
Figure 5.
Aggressive corneal infection by Staphylococcus pseudintermedius. (A) Patient cornea was severely affected with a focal zone of conjunctival graft destruction at 4 o’clock position in the paracentral graft region (green arrow). Patient was treated with topical ofloxacin and cefazolin and systemic amoxicillin/clavulanic acid immediately after surgery. (B,C) Antibiotic susceptibility testing performed for topical (A) and systemic antibiotic sets (B). The isolate was resistant to the multiple topical (amikacin, cefazolin, cefoxitin, gentamicin, neomycin, ofloxacin, polymyxin B, tetracycline, and tobramycin) and systemic antibiotics (amoxicillin/clavulanic acid, cephalexin, ciprofloxacin, clindamycin, doxycycline, enrofloxacin, marbofloxacin, penicillin G, and sulfamethoxazole/trimethoprim). The isolate was also penicillin-binding protein 2A–positive and susceptible only to topical bacitracin.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Bacterial species distribution from corneal stromal ulcer samples. Distribution of incidence of the specific microorganism detection in canine patients. Data are presented as a percentage of total isolates (n = 167). a Citrobacter freundii, Enterobacter cloacae, Escherichia coli, and Serratia marcescens; b Staphylococcus spp. (S. auricularis, S. hominis, S. saprophyticus, S. simulans, S. warneri, and S. xylosus) excluding S. pseudintermedius, S. capitis, S. epidermidis, Staphylococcus intermedius and S. aureus. c Gram-positive and Gram-negative bacteria (this group was identified by Gram labeling since MALDI-TOF analysis yielded no identification) and unknown (this group was also not identified by MALDI-TOF analysis). These two groups likely represent multiple bacterial species on the target plate spot or no hit in the MALDI-TOF data base. d Presence of each isolate of 1% or less represented by Acinetobacter johnsonii, Actinomyces sp., Bacillus pumilus, Bacillus sp., Exiguobacterium sp., Klebsiella oxytoca, Kocuria sp., Microbacterium sp. Micrococcus luteus, Moraxella canis, Pasteurella canis, Pseudomonas sp., Psychrobacter sp., Staphylococcus aureus, Streptococcus lutetiensis, and Streptococcus salivarius.
Table 1.
Bacterial species distribution from corneal stromal ulcer samples. Distribution of incidence of the specific microorganism detection in canine patients. Data are presented as a percentage of total isolates (n = 167). a Citrobacter freundii, Enterobacter cloacae, Escherichia coli, and Serratia marcescens; b Staphylococcus spp. (S. auricularis, S. hominis, S. saprophyticus, S. simulans, S. warneri, and S. xylosus) excluding S. pseudintermedius, S. capitis, S. epidermidis, Staphylococcus intermedius and S. aureus. c Gram-positive and Gram-negative bacteria (this group was identified by Gram labeling since MALDI-TOF analysis yielded no identification) and unknown (this group was also not identified by MALDI-TOF analysis). These two groups likely represent multiple bacterial species on the target plate spot or no hit in the MALDI-TOF data base. d Presence of each isolate of 1% or less represented by Acinetobacter johnsonii, Actinomyces sp., Bacillus pumilus, Bacillus sp., Exiguobacterium sp., Klebsiella oxytoca, Kocuria sp., Microbacterium sp. Micrococcus luteus, Moraxella canis, Pasteurella canis, Pseudomonas sp., Psychrobacter sp., Staphylococcus aureus, Streptococcus lutetiensis, and Streptococcus salivarius.
| Organism | (n = 167) |
|---|---|
| Staphylococcus pseudintermedius | 22% |
| Staphylococcus epidermidis | 12% |
| Staphylococcus capitis | 11% |
| Pseudomonas aeruginosa | 10% |
| enteric Gram-negative rods a | 7% |
| coagulase negative staphylococci b | 5% |
| Streptococcus canis | 5% |
| Corynebacterium sp. | 2% |
| Enterococcus faecalis | 2% |
| Streptococcus sp. | 2% |
| Rothia sp. | 2% |
| Enterococcus faecium | 1% |
| Staphylococcus aureus | 1% |
| Staphylococcus intermedius | 1% |
| Other c | 5% |
| Other d | 10% |
Table 2.
Resistance profile of isolates from corneal stromal ulcer samples from 2018–2021. Percentage (%) of resistant bacterial species from patient samples presented as combined resistance (TOTAL; intrinsic and acquired resistance together), intrinsic resistance only (INTRINSIC), or acquired resistance only (ACQUIRED). The number of isolates is 167 for each antibiotic in the TOTAL column exceptfor oxacillin, which numbered 29. * = although amoxicillin/clavulanic acid is not used topically, data for this antibiotic are presented here since it is often used postoperatively as a systemic antibiotic.
Table 2.
Resistance profile of isolates from corneal stromal ulcer samples from 2018–2021. Percentage (%) of resistant bacterial species from patient samples presented as combined resistance (TOTAL; intrinsic and acquired resistance together), intrinsic resistance only (INTRINSIC), or acquired resistance only (ACQUIRED). The number of isolates is 167 for each antibiotic in the TOTAL column exceptfor oxacillin, which numbered 29. * = although amoxicillin/clavulanic acid is not used topically, data for this antibiotic are presented here since it is often used postoperatively as a systemic antibiotic.
| Antibiotic | Total | Intrinsic | Acquired |
|---|---|---|---|
| polymyxin B | 60% | 1% | 59% |
| oxacillin | 59% | 0% | 59% |
| cefoxitin | 46% | 7% | 39% |
| cefazolin | 46% | 11% | 35% |
| amoxicillin/clavulanic acid * | 44% | 10% | 34% |
| tetracycline | 38% | 5% | 33% |
| tobramycin | 32% | 5% | 27% |
| neomycin | 29% | 10% | 19% |
| bacitracin | 26% | 0% | 26% |
| ofloxacin | 23% | 0% | 23% |
| gentamicin | 21% | 4% | 17% |
| amikacin | 16% | 6% | 10% |
Table 3.
Bacterial species distribution from corneal stromal ulcer samples relative to the patient’s previous antibiotic treatments. Distribution of isolates in canine patients. Data are presented as a percentage of total isolates (n = 61 and n = 106). a Citrobacter freundii, Enterobacter cloacae, Escherichia coli, and Serratia marcescens; b Staphylococcus spp. (S. auricularis, S. hominis, S. saprophyticus, S. simulans, S. warneri, and S. xylosus) excluding S. pseudintermedius, S. capitis, S. epidermidis, Staphylococcus intermedius and S. aureus. c Gram-positive and Gram-negative bacteria (this group was identified by Gram labeling since MALDI-TOF analysis yielded no identification) and unknown (this group was also not identified by MALDI-TOF analysis). These two groups likely represent multiple bacterial species on the target plate spot or no hit in the MALDI-TOF data base. d Presence of each isolate of 1% or less represented by Acinetobacter johnsonii, Actinomyces sp., Bacillus pumilus, Bacillus sp., Exiguobacterium sp., Klebsiella oxytoca, Kocuria sp., Microbacterium sp. Micrococcus luteus, Moraxella canis, Pasteurella canis, Pseudomonas sp., Psychrobacter sp., Streptococcus lutetiensis, and Streptococcus salivarius.
Table 3.
Bacterial species distribution from corneal stromal ulcer samples relative to the patient’s previous antibiotic treatments. Distribution of isolates in canine patients. Data are presented as a percentage of total isolates (n = 61 and n = 106). a Citrobacter freundii, Enterobacter cloacae, Escherichia coli, and Serratia marcescens; b Staphylococcus spp. (S. auricularis, S. hominis, S. saprophyticus, S. simulans, S. warneri, and S. xylosus) excluding S. pseudintermedius, S. capitis, S. epidermidis, Staphylococcus intermedius and S. aureus. c Gram-positive and Gram-negative bacteria (this group was identified by Gram labeling since MALDI-TOF analysis yielded no identification) and unknown (this group was also not identified by MALDI-TOF analysis). These two groups likely represent multiple bacterial species on the target plate spot or no hit in the MALDI-TOF data base. d Presence of each isolate of 1% or less represented by Acinetobacter johnsonii, Actinomyces sp., Bacillus pumilus, Bacillus sp., Exiguobacterium sp., Klebsiella oxytoca, Kocuria sp., Microbacterium sp. Micrococcus luteus, Moraxella canis, Pasteurella canis, Pseudomonas sp., Psychrobacter sp., Streptococcus lutetiensis, and Streptococcus salivarius.
| Organism | No Previous Antibiotic Treatment (n = 61) | Previous Antibiotic Treatment (n = 106) |
|---|---|---|
| Staphylococcus pseudintermedius | 34% | 15% |
| Staphylococcus epidermidis | 2% | 18% |
| Staphylococcus capitis | 8% | 13% |
| Pseudomonas aeruginosa | 15% | 8% |
| enteric Gram-negative rodsa | 7% | 7% |
| coagulase negative staphylococcib | 7% | 5% |
| Streptococcus canis | 5% | 6% |
| Corynebacterium sp. | 0% | 3% |
| Enterococcus faecalis | 2% | 2% |
| Streptococcus sp. | 3% | 1% |
| Rothia sp. | 2% | 3% |
| Enterococcus faecium | 0% | 2% |
| Staphylococcus aureus | 0% | 2% |
| Staphylococcus intermedius | 3% | 0% |
| Otherc | 3% | 7% |
| Otherd | 10% | 10% |
Table 4.
Distribution of the most common bacterial species from canine corneal ulcers across various geographical locations.
Table 4.
Distribution of the most common bacterial species from canine corneal ulcers across various geographical locations.
| Location | Author, Year | Staphylococcus spp. | Pseudomonas aeruginosa | Streptococcus spp. |
|---|---|---|---|---|
| Australia | Hindley et al., 2015 [7] | 18% | 31% | 31% |
| Taiwan | Lin et al., 2007 [25] | 49% | 8% | 7% |
| Thailand | Ekapopphan et al., 2018 [11] | 46% | 21% | 8% |
| UK | Tsvetanova et al., 2020 [10] | 14% | 40% | 28% |
| Switzerland | Suter et al., 2018 [8] | 41% | 11% | 26% |
| Brazil | Prado et al., 2005 [24] | 57% | 5% | 11% |
| Brazil | Varges et al., 2009 [26] | 59% | - | - |
| Southeast US | Tolar et al., 2006 [6] | 33% | 21% | 17% |
| Southeast US | McKeever, 2021 [5] | 34% | 18% | 28% |
| Midwest US | Jinks et al., 2020 [12] | 36% | 10% | 34% |
| Midwest US | Hewitt et al., 2020 [15] | 32% | 12% | 19% |
| Midwest US | this study, 2022 | 50% | 10% | 7% |
Table 5.
Comparison of susceptibility profiles of isolates in the midwestern US between Hewitt et al. and this study.
Table 5.
Comparison of susceptibility profiles of isolates in the midwestern US between Hewitt et al. and this study.
| Topical Antibiotic Susceptibility | ||
| Antibiotic | Hewitt et al. | This Study |
| amikacin | 77% | 84% |
| amikacin and cefazolin | 79% | 93% |
| bacitracin | 7% | 74% |
| cefazolin | 8% | 54% |
| gentamicin | 74% | 79% |
| gentamicin and cefazolin | 76% | 90% |
| gentamicin and ofloxacin | 87% | 88% |
| neomycin | 76% | 71% |
| neopoly | 76% | 79% |
| neopolybac | 77% | 96% |
| ofloxacin | 53% | 77% |
| ofloxacin and cefazolin | 55% | 87% |
| polymyxin B | 0% | 40% |
| tobramycin | 57% | 68% |
| Systemic Antibiotic Susceptibility | ||
| amoxicillin/clavulanic acid | 78% | 56% |
| cephalexin | 23% | 35% |
| clindamycin | 61% | 41% |
| doxycycline | 56% | 66% |
| enrofloxacin | 64% | 79% |
| marbofloxacin | 75% | 85% |
| penicillin | 35% | 26% |
| trimethoprim/sulfamethoxazole | 53% | 59% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Joksimovic, M.; Ford, B.A.; Lazic, T.; Soldatovic, I.; Luzetsky, S.; Grozdanic, S. Antibiotic Recommendations for Treatment of Canine Stromal Corneal Ulcers. Vet. Sci. 2023, 10, 66. https://doi.org/10.3390/vetsci10020066
AMA Style
Joksimovic M, Ford BA, Lazic T, Soldatovic I, Luzetsky S, Grozdanic S. Antibiotic Recommendations for Treatment of Canine Stromal Corneal Ulcers. Veterinary Sciences. 2023; 10(2):66. https://doi.org/10.3390/vetsci10020066
Chicago/Turabian StyleJoksimovic, Milan, Bradley A. Ford, Tatjana Lazic, Ivan Soldatovic, Sergey Luzetsky, and Sinisa Grozdanic. 2023. "Antibiotic Recommendations for Treatment of Canine Stromal Corneal Ulcers" Veterinary Sciences 10, no. 2: 66. https://doi.org/10.3390/vetsci10020066
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.