 |
Case Report
A case of type III selective intrauterine growth restriction in a monochorionic twin pregnancy with a myriad of Doppler changes of the umbilical and vitelline arteries
1 Intern at Tony Tan Women and Fetal Clinic, Mount Alvernia Hospital, Singapore
2 MBBS (Singapore), MMED (O&G, Singapore), MRANZCOG (Australia, New Zealand), FRCOG (UK), FAMS (Singapore), Consultant Obstetrician and Gynecologist, Tony Tan Women and Fetal Clinic, Mount Alvernia Hospital, Singapore
3 MBBS (Singapore), MMED (Paed) (Singapore), MRCP (Paed) (UK), Consultant Pediatrician and Neonatologist, Kinder Clinic, Mount Alvernia Hospital, Singapore
Address correspondence to:
Tan Tony Yew Teck
820 Thomson Road, Mount Alvernia Hospital, #07-66 Medical Centre D, Singapore 574623,
Singapore
Message to Corresponding Author
Article ID: 100144Z08DG2023
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Ghosh D, Tan TYT, Tan THM. A case of type III selective intrauterine growth restriction in a monochorionic twin pregnancy with a myriad of Doppler changes of the umbilical and vitelline arteries. J Case Rep Images Obstet Gynecol 2023;9(1):44–48.ABSTRACT
Monochorionic twins have higher mortality rates than dichorionic twins. Selective intrauterine growth restriction (sIUGR) is a common complication found in monochorionic twins. We report such a case of type III sIUGR monochorionic twins. There was positive end-diastolic flow of umbilical arteries, which corresponded to type I sIUGR at 15 weeks. Then, the umbilical arteries showed persistently absent end-diastolic flow at 17 weeks which corresponded to type II sIUGR. Finally, the umbilical artery showed intermittent absent/reversed end-diastolic flow which corresponded to type III sIUGR. This case demonstrated a unique myriad of Doppler changes during the pregnancy, indicating its significance in being reported. The twins were delivered by caesarean section at 32 weeks and were developing well. Placental examination showed unequal placental sharing and the presence of an arterio-arterial anastomosis. These are characteristic findings of a type III sIUGR. Type III sIUGR may not be obvious at the initial examination but may only be obvious at later examinations.
Keywords: Doppler changes, Monochorionic, sIUGR, Type III
Introduction
Twin pregnancies are already known to be precarious for the mother and children. Twins can either be dizygotic (i.e., come from two fertilized eggs) or monozygotic (i.e., may originate from the splitting of one fertilized egg). Depending upon the time of this split, monozygotic twins may be monochorionic or dichorionic [1]. Twins can be monochorionic or dichorionic, i.e., have one or two placentas respectively. Monochorionic placentas can be diamniotic or monoamniotic, i.e., have two or one amniotic sacs respectively. Monochorionic twins have significantly higher rates of mortality, about 12% from 10 to 24 weeks, compared to 2% among the more common dichorionic twins [2],[3]. The risk for perinatal complications among monochorionic diamniotic twins (one placenta and two amniotic sacs) is 3–6 fold higher than in dichorionic twins [4].
This can be attributed to the peculiar characteristics of monochorionic placentas. With regard to vascular anatomy, complications associated with unequal blood flow can arise from unbalanced flow via anastomoses, or connections between arteries (AAA), veins (VVA), or an artery and vein (AVA) [4]. If one twin was smaller, it is often due to unequal placental sharing which may be associated with velamentous or marginal cord insertions [5].
Selective intrauterine growth restriction (sIUGR) occurs in about 10–15% of monochorionic twins [6]. The smaller twin typically has a smaller share of the placenta with less blood flow and nutrients as a result of being supported by a smaller portion of the placenta. sIUGR can be classified into three types as suggested by Gratacós et al. based on the pattern of end-diastolic flow of the umbilical arteries of the smaller twin. Type I is diagnosed when there is persistently positive end-diastolic blood flow. Type II is when there is persistently absent or reverse end-diastolic flow while type III has an intermittent or sinusoidal pattern of absent and/or reverse end-diastolic flow [6].
In type I sIUGR, the smaller twin is generally fine, with an in-utero mortality rate of about 2–4% [7],[8]. This can be due to less discordant placental sharing and/or greater number of anastomoses [8]. The resulting higher bidirectional blood flow compensates for the unequal placental share for the smaller twin [8]. In type II sIUGR, there is 70–90% chance of fetal deterioration of the smaller twin prior to a gestational age of 30 weeks [8]. There is greater discordance in placental sharing and lack of anastomoses. This often leads to perinatal mortality (if managed expectantly) with neurological damage to the co-twin in type II sIUGR fetuses [8]. Type III sIUGR is typically characterized by a large arterio-arterial anastomosis, with the risk of demise of the IUGR twin being about 15–20% [8]. The mean gestational age at delivery is generally 35.4 weeks for type I, 30.7 weeks for type II, and 31.6 weeks for type III sIUGR twins [6]. Interestingly, intrauterine fetal death (IUFD) of the smaller twin occurs more frequently in a type III sIUGR (15%) than a type II sIUGR because IUFD in a type III tends to be more difficult to anticipate than that for a type II. This can result in a 20% risk of parenchymal brain lesion in the larger twin, potentially resulting in the death of the larger twin [9].
Case Report
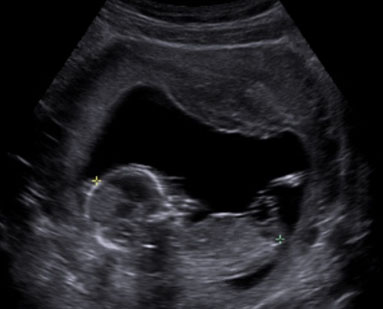
This was the first pregnancy of a 26-year old woman expecting monochorionic twins. She was first seen at 12 weeks and was followed up closely by a fetal medicine specialist with experience in the care of monochorionic twins at least fortnightly. It was obvious that Twin B’s estimated fetal weight was significantly larger than that of Twin A from 15 weeks, and this difference continued to increase as the pregnancy progressed (Figure 1). Discordances were seen in the abdominal circumferences and femur lengths. At 15 weeks gestation, the umbilical artery showed persistently positive end-diastolic flow in Twin A. This suggested that it was type I sIUGR. At 17 weeks, the Doppler studies showed persistently absent end-diastolic flow in the umbilical artery which corresponded to type II sIUGR (Figure 2). This raised concerns regarding the survival of Twin A as there was a 90% chance of deterioration of this fetus. Thus, we considered the following options for the twins: (1) expectant management with close monitoring of their arterial and venous Dopplers, (2) selective laser photocoagulation of the placental vascular, (3) cord occlusion of twin A, and (4) abortion of the whole pregnancy. With type II sIUGR diagnosis, cord occlusion of the umbilical cord of Twin A was considered to eliminate the risk of acute twin-to-twin transfusion from the bigger to the smaller twin if the smaller twin was to die in-utero. Three days later, a repeat scan, however, showed, intermittently absent and reverse end-diastolic flow of the umbilical artery (Figure 3). This changed the diagnosis to type III sIUGR. This case, thus, showed unique Doppler changes from a classification of type I to II to III sIUGR. The intermittent nature of the Doppler studies of the umbilical arteries could explain why it was first thought to be type I, then type II, and finally, type III sIUGR (Figure 4). At 32 weeks, head circumference for both Twins A and B were similar, whereas the abdominal circumferences and femur lengths for Twin A were significantly lower. The timing of the delivery was discussed with the couple and the neonatologist. As the estimated weight discordance was large at about 50% (2 and 1 kg for the Twins B and A, respectively), and the possibility of an unexpected death of the smaller twin with risk of death and morbidity to the other twin was significant, a joint decision was made to deliver the babies at 32 weeks. Corticosteroids were administered and caesarean section was performed. At delivery, the weights of Twins A and B were 1.8 and 1.2 kg, respectively, with birth weight discordance of 30%. The placenta was examined. The veins were injected with white dye and arteries injected with blue dye. Twin B’s bigger umbilical cord was centrally inserted, while that of Twin A was marginally inserted (Figure 5). The vascular equator is along the dotted line, where it shows that about 75% of the placenta belong to Twin B, while the other 25% belong to Twin A. The unequal placental sharing and the presence of an AAA (circled) validated the sIUGR type III diagnosis as these are known characteristics of this diagnosis (Figure 5). Both babies are developing well although there was mild respiratory distress syndrome (RDS) in the first few days that subsequently resolved.





Discussion
This case report demonstrates the possible variations in the initial presentation of a sIUGR type III case. Type III sIUGR cases do not tend to be predictable as they may often conceal themselves as type I or type II sIUGR cases [10],[11]. In another sIUGR monochorionic twin pregnancy case, the smaller fetus displayed positive end-diastolic flow, suggesting a type I diagnosis at 28 weeks [[3]. The smaller twin then displayed an end-diastolic flow pattern that was consistent to that of a type III sIUGR during the third consultation and a caesarean section was performed at 32 weeks [3]. The variations in the Doppler studies of the umbilical artery are due to the transmitted waveforms of a typical sinusoidal pattern of an arterio-arterial anastomosis (AAA). Without this anastomosis, the chance of survival of the smaller twin, with a significantly smaller portion of the placenta would have been very low. However, the presence of an arterio-arterial anastomosis (AAA) implies a high risk of hemodynamic (blood-related) or feto-fetal transfusion problems if one twin was to die inutero or suffer from an episode of hypotension [6]. Due to the AAA compensating for the lack of placental share, the larger twin helps to support the smaller twin through this anastomosis [6].
Conclusion
It is therefore recommended that all monochorionic twins especially those complicated by sIUGR be managed by fetal medicine specialists experienced in the care of monochorionic twins as the variations in initial presentations can be bewildering. While the rate of deterioration in type III cases is generally lower, compared to type II, there is still the risk of unexpected intrauterine fetal death of 15% for the smaller twin. As in our case, the sIUGR classification changed multiple times due to the variable Doppler ultrasound findings. When the diagnosis was type II sIUGR, we were even considering cord occlusion. When the diagnosis was correctly made, it allowed us to manage expectantly till 32 weeks. Thi demonstrates the importance of careful monitoring of the twins with frequent Doppler ultrasound examinations as this essentially enabled both twins to be delivered at an appropriate gestational age.
REFERENCES
1.
Al Riyami N, Al-Rusheidi A, Al-Khabori M. Perinatal outcome of monochorionic in comparison to dichorionic twin pregnancies. Oman Med J 2013;28(3):173–7. [CrossRef]
[Pubmed]

2.
Sebire NJ, Snijders RJ, Hughes K, Sepulveda W, Nicolaides KH. The hidden mortality of monochorionic twin pregnancies. Br J Obstet Gynaecol 1997;104(10):1203–7. [CrossRef]
[Pubmed]
3.
Bot M, Vladareanu R, Burnei A, Munteanu A, Calo I, Vladareanu S. Monochorionic vs dichorionic twins: Kanet test vs postnatal neurodevelopment. Maedica (Bucur) 2020;15(1):61–70. [CrossRef]
[Pubmed]
4.
Sierakowski A, Eapen V, Črnčec R, Smoleniec J. Developmental and behavioral outcomes of uncomplicated monochorionic diamniotic twins born in the third trimester. Neuropsychiatr Dis Treat 2017;13:1373–84. [CrossRef]
[Pubmed]
5.
Kalafat E, Thilaganathan B, Papageorghiou A, Bhide A, Khalil A. Significance of placental cord insertion site in twin pregnancy. Ultrasound Obstet Gynecol 2018;52(3):378–84. [CrossRef]
[Pubmed]
6.
Gratacós E, Antolin E, Lewi L, et al. Monochorionic twins with selective intrauterine growth restriction and intermittent absent or reversed end-diastolic flow (Type III): Feasibility and perinatal outcome of fetoscopic placental laser coagulation. Ultrasound Obstet Gynecol 2008;31(6):669–75. [CrossRef]
[Pubmed]
7.
Yang J, Wei Y, Qi H, et al. Neonatal hair profiling reveals a metabolic phenotype of monochorionic twins with selective intrauterine growth restriction and abnormal umbilical artery flow. Mol Med 2020;26(1):37. [CrossRef]
[Pubmed]
8.
Bennasar M, Eixarch E, Martinez JM, Gratacós E. Selective intrauterine growth restriction in monochorionic diamniotic twin pregnancies. Semin Fetal Neonatal Med 2017;22(6):376–82. [CrossRef]
[Pubmed]
9.
Lewi L, Deprest J, Hecher K. The vascular anastomoses in monochorionic twin pregnancies and their clinical consequences. Am J Obstet Gynecol 2013;208(1):19–30. [CrossRef]
[Pubmed]
10.
Valsky DV, Martinez-Serrano MJ, Sanz M, et al. Cord occlusion followed by laser cord transection in monochorionic monoamniotic discordant twins. Ultrasound Obstet Gynecol 2011;37(6):684–8. [CrossRef]
[Pubmed]
11.
Buca D, Pagani G, Rizzo G, et al. Outcome of monochorionic twin pregnancy with selective intrauterine growth restriction according to umbilical artery Doppler flow pattern of smaller twin: Systematic review and meta-analysis. Ultrasound Obstet Gynecol 2017;50(5):559–68. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Debora Ghosh - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Tan Tony Yew Teck - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Tan Terence Hwa Min - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2023 Debora Ghosh et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}